Shared Area of Focus
The stakeholder leads workshop identified a shared area of focus in axSpA which informed the rest of the programme—patient empowerment through education on the disease and treatment options available, to enable patient involvement in management and ultimately increase treatment adherence. See supplementary materials (Table S1) for more information.
Participants
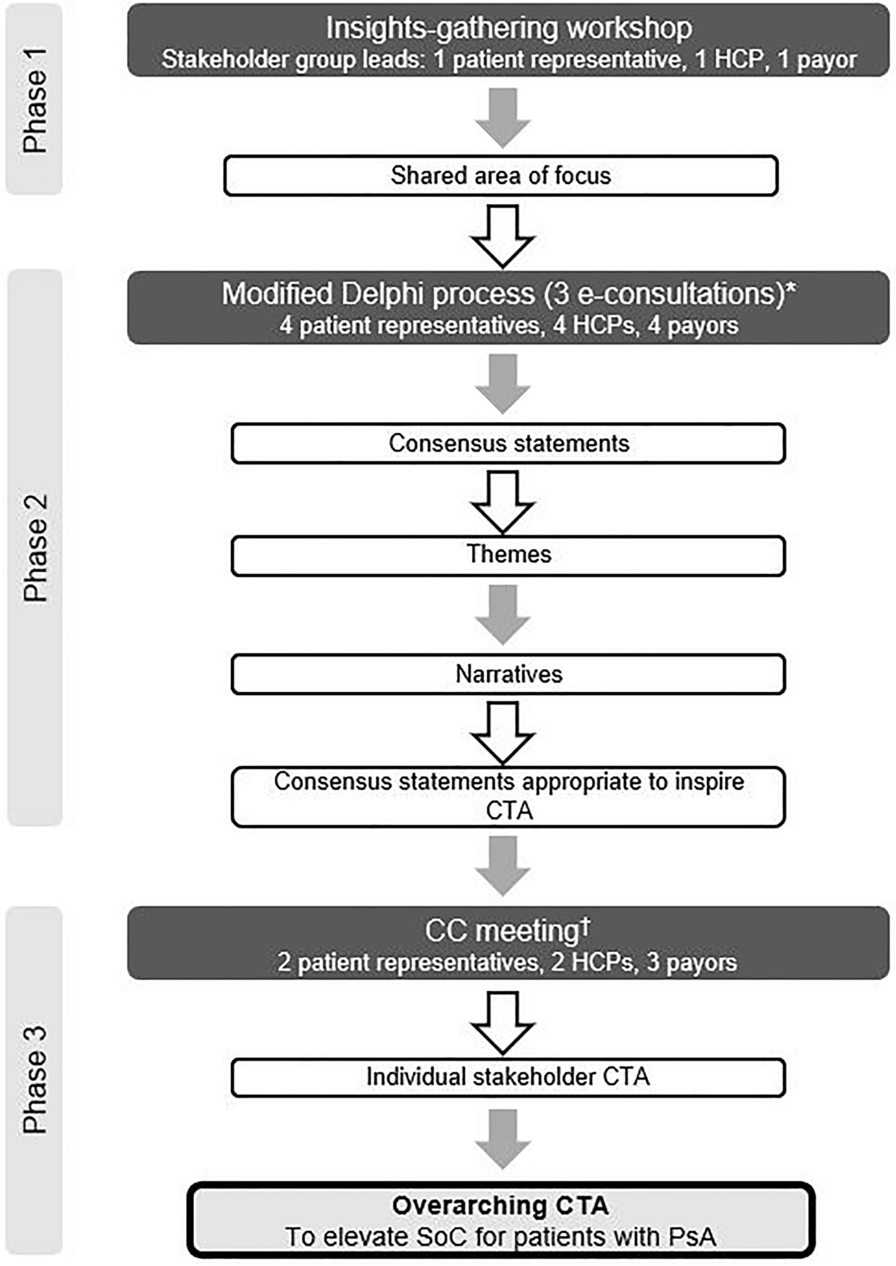
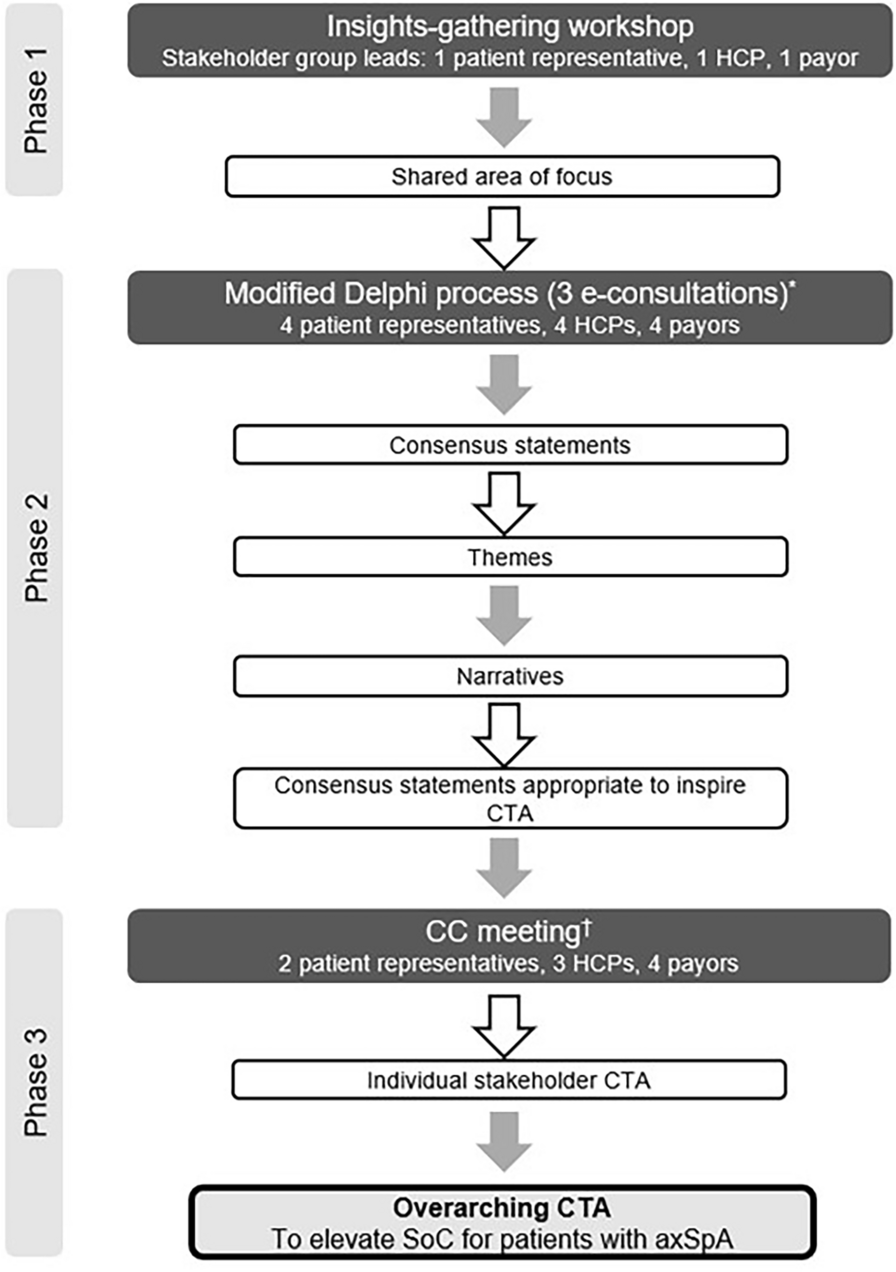
Participants of the axSpA CC were recruited on the basis of their expertise and experience in axSpA (Fig. 1, Table 1).
Themes and Narratives
Following the Delphi process, four key themes emerged that the consensus statements could be divided into.
1. Patient EmpowermentDiscussion Points
After completion of the Delphi process, 21 statements reached consensus, of which 16 were used in the patient empowerment narrative (Tables 2, S2).
Table 2 Patient empowerment narrativePatient empowerment was defined as “the process by which people are supported to gain sufficient knowledge and skills, to enable them to be as actively involved as they want to be in making decisions that shape their health”. The initial definition was modified as stakeholders felt that knowledge alone was insufficient to empower patients (Table S2). An empowered patient was described as someone who can confidently discuss and proactively bring up symptoms, treatment options and concerns with their HCP. While 83% ‘agreed’ or ‘strongly agreed’ that patient empowerment plays a role in patients demanding higher treatment goals, 17% disagreed, explaining that “higher treatment goals” do not reflect patient objectives, as patients simply want to be well and so they focus on maintaining good results rather than prioritising higher goals.
Stakeholders felt the main barriers to patient empowerment are the lack of easily accessible, trustworthy information, reluctance of patients with axSpA to be involved in their care and the paternalistic approach to medicine by HCPs. Consensus was achieved for all stakeholders having a role in empowering patients with axSpA (Table 2). However, those who disagreed with a role for the pharmaceutical industry felt that HCPs had a greater role, as patients may view industry involvement to be solely based around promotion of their products, thus reducing patient confidence in decision-making. Similarly, the role of payors was challenged as a result of potential conflicting interests i.e. favouring lower costs of treatment.
Insights suggested that patient organisations offer support through educational programmes/workshops directed to all stakeholders. However, one stakeholder felt that HCPs obtain information through professional associations and so joint support is not needed. The need for reliable ways of measuring patient empowerment in axSpA reached consensus (Table 2); patient surveys could be used to understand and monitor the extent of patient involvement in disease management.
Fifty-eight percent of stakeholders recognised variations in patient empowerment with ethnicity, where some ethnicities (in particular, Asian and African) have fewer opportunities than others to engage in their care as a result of cultural and socio-economic factors. Table 3 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient empowerment. Overarching CTA were derived from the CTA specific for each stakeholder group (Tables S3, S4) which were inspired by the consensus statements marked with a superscript dagger symbol in Table 2 and generated at the CC meeting.
Table 3 Overarching CTA and associated stakeholder-specific discussions for the theme of patient empowerment2. Patient KnowledgeDiscussion Points
Of the 15 statements that achieved consensus, 12 were used in the patient knowledge narrative as they succinctly underpinned the current situation, need for change and desired state/action (Tables 4, S5).
Table 4 Patient knowledge narrativeOnly 42% of stakeholders agreed that patients with axSpA are sufficiently knowledgeable about their disease. Further insights from the 58% who disagreed revealed that the current information available to patients with axSpA is not patient-friendly, relevant or accessible, and is not clearly understood. Moreover, all stakeholders highlighted that there is room for improvement in the level of knowledge and creating patient-friendly education tailored to their interests is important. The need to understand available treatment options in addition to disease knowledge was reflected in the revised statement, which included this, reaching 100% consensus (Table S5). All stakeholders advocated the role of exercise in axSpA management (Table 4). However, 8% disagreed that exercise plans should be adhered to as patients have the right to choose. Stakeholders recognised the need for non-judgemental, open discussions between HCPs and patients about adhering to exercise plans.
Open-ended questions about the facilitation of patient empowerment and involvement in care identified important educational topics, e.g. treatment expectations, self-evaluation, comorbidity recognition, influence of lifestyle factors and compliance to treatment plans. All stakeholders voted that patient education should be delivered through face-to-face discussions with their HCP. The use of questionnaires to assess patient knowledge was proposed, while aiming to avoid response bias (i.e. knowledgeable patients may be more likely to engage in questionnaires than those less knowledgeable). Other means of assessing patient knowledge included patient focus groups led by patient representatives and optimised use of existing tools. Alongside patient education, stakeholders felt that HCPs and payors should be educated on their interpersonal skills and the non-clinical impact of axSpA (e.g. family planning, emotional well-being, employment).
All stakeholders acknowledged the need for easily accessible, high-quality, neutral information, but recognised support may be needed to help patients understand what constitutes “high-quality” as a large amount of poor-quality information is available (e.g. social media). Fifty percent of stakeholders disagreed that patient organisations should have the main responsibility for ensuring patients have access to high-quality information (Table S5). Payors felt that patient organisations and HCPs should work together to create, provide and explain education, but that ultimate responsibility for patient education lies with HCPs as they are more informed. The revised statement specifying HCPs subsequently achieved consensus, but challenges of implementation in clinical practice were recognised e.g. HCPs lack time to adequately educate patients (Table 4). Table 5 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient knowledge. See Tables S6 and S7 in the supplementary materials for the CTA per stakeholder.
Table 5 Overarching CTA and associated stakeholder-specific discussions for the theme of patient knowledge3. Patient–HCP ConsultationsDiscussion Points
Consensus was achieved on 20 statements (Table S8), of which 12 were used within the patient–HCP consultations narrative as they succinctly underpinned the current situation, need for change and desired state/action (Table 6). One statement was also used within the optimal initial treatment narrative, as it shaped both narratives (Table 8).
Table 6 Patient–HCP consultations narrativeThe patient–HCP narrative focused on patient-centred care and identified the importance of SDM in elevating the SoC in axSpA. Initial disagreement around recognition of the full patient burden by HCPs highlighted one of many challenges faced within axSpA care. Payors felt that HCPs cannot understand the full burden as they do not experience the disease in daily life, highlighting the importance of the patient voice during consultations. Stakeholders felt that current tools do not capture the full disease burden and thus consensus was achieved that HCPs should be educated on the burden of axSpA through patient experience and that patient-reported outcome tools are required. Despite the need for patient involvement, stakeholders agreed that many patients are not aware of their potential involvement in treatment decisions (Table 6). Several stakeholders felt that this was due to the traditional, hierarchical relationship between patients and HCPs, as well as a lack of patient confidence—rather than unwillingness—to take part (Table S8). Consequently, consensus was achieved that patients with axSpA should be made aware of their role in treatment decisions and asked if they would like to be involved (Table 6).
Further insights demonstrated the need for HCPs to facilitate open conversations where patients feel valued. All stakeholders advocated for a personalised approach to treatment (i.e. based on gender, ethnicity, lifestyle factors, presenting disease features) and 92% recognised the need to align HCP and patient goals before proceeding with treatment (Table 6). Initial disagreement was observed over which stakeholder should have the final say in treatment decisions (Table S8). Stakeholders felt that while it was important to take patient opinions into account to avoid compliance issues, patients may have limited knowledge of clinical considerations or funding restrictions compared with HCPs. Therefore, consensus was reached once the statement was modified to acknowledge that both HCPs and patients should have an equal say and if disagreement remains, further discussions should be had. Although consensus was reached that the main barrier HCPs experience is a lack of time in appointments, those who disagreed suggested that this is a false perception that patient involvement takes time and reflects a reluctance to embrace a patient-centred approach. Table 7 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient–HCP consultations. See Tables S9–S11 in the supplementary materials for the CTA per stakeholder.
Table 7 Overarching CTA and associated stakeholder-specific discussions for the theme of patient–HCP consultations4. Optimal Initial TreatmentDiscussion Points
Seven statements achieved consensus and were used within the optimal initial treatment narrative (Table 8, Table S12).
Table 8 Optimal initial treatment narrativeFifty percent of stakeholders, including payors, agreed that payors are sufficiently educated on axSpA and outcomes of different treatment options but that they are constrained from providing optimal initial care by higher authorities. Payors who disagreed explained that prioritising cost considerations over optimal initial treatment is an outdated belief and, in some countries, (e.g. Germany) there are no major restrictions to prescribing whatever treatment is necessary. Additionally, one payor noted that it is not only healthcare systems that influence optimal treatment but that guidelines created by scientific societies play a role too. Consensus was reached once the initial statement was revised to note that educating payors on the burden of disease and the outcomes of using optimal initial treatments will allow more patients to access the most appropriate biologics to meet their treatment goals (Table S12).
The contrast between cost considerations and personalised treatment was evident and felt to negatively affect treatment decisions and patient outcomes (Table S12). Open-ended questions revealed that cost was seen as the single most important factor in determining which treatment patients with axSpA received. Table 9 contains the overarching CTA and associated stakeholder-specific discussions for the theme of optimal initial treatment. See Tables S13–S15 in the supplementary materials for the CTA per stakeholder.
Table 9 Overarching CTA and associated stakeholder-specific discussions for the theme of optimal initial treatment 





留言 (0)