The main finding of our study was that the mean skin temperature was higher in the intervention group than in the control group after 25 min, which lasted until the end of the experiment. The differences between the two groups continued to increase as the experiment progressed. The correlation between mean skin temperature and core temperature is non-linear and multifactorial, but the skin is the primary interface affected by external changes in temperature. The direct clinical relevance of the observed difference in mean skin temperature of 0.93 °C ± 0.59 is uncertain, and not the topic of this article. A priori, an increase in mean skin temperature will contribute to an increased core temperature rewarming rate in hypothermic patients after rescue or a reduced demand for metabolic heat production and oxygen consumption in patients at risk of accidental hypothermia.
We suspect that the observed initial difference between the two groups is attributable to the methodological decision of applying each corresponding layer simultaneously to all four participants present in the chamber simultaneously. The application of the vapor barrier meant that the wrapping of the participants in the control group was slightly delayed (approximately 60–90 s) compared with that in the intervention group, and we suspect that this delay is the main reason for the observed difference during the first 10 min. Therefore, we believe that this difference was of little relevance.
There was a clear difference in humidity levels between the intervention and control groups. Water that evaporated from the clothes appeared to be effectively contained within the vapor barrier, leading to lower levels of humidity outside the vapor barrier in the intervention group. In the control scenario, in which no vapor barrier was present, there was a rapid increase in humidity levels in the model during the first 20 min of the rewarming phase, followed by a period of slow but steady increase over the next 40 min of rewarming. Limiting evaporation inside the vapor barrier and maintaining latent heat close to the body may explain the higher rate of skin temperature increase observed in the intervention group.
Interestingly, our data showed a higher temperature between the insulating blankets and outer shell in the control group than in the intervention group. Some of this difference may be attributable to the isolating effects of the extra layer in the intervention group compared with that those in the control. However, this layer was extremely thin, and we suspect that the latent thermal energy present in the water vapor in the model was a substantial contributor to the temperature difference. The barrier used in the intervention group contained this vapor and, thereby, the thermal energy was closer to the patient, which may be the reason for the faster mean skin temperature rewarming rate in the intervention group.
Henriksson et al. found a higher rewarming rate with either a vapor barrier or wet clothing removal than wrapping a patient wearing wet clothing in an insulating material without a vapor barrier [10]. They found no difference between wet clothing removal and vapor barrier application. However, increasing the amount of insulating material provided similar effects as using a vapor barrier, perhaps because more material meant less vapor could escape. Hagen et al. found a higher rewarming rate when wet clothing was removed and the patient was placed in a vapor barrier compared with wrapping the patient in the vapor barrier with wet clothing still on [17].
Our core temperature measurements showed a slight decrease in core temperature for the entire 60-minute rewarming phase. There may have been slight heat stress for the participants during the application of the monitoring equipment before the study, followed by a slow return to baseline. This may also be attributed to a physiological phenomenon called afterdrop, in which the core temperature continues to decrease after a person is removed from a cold environment. The cold environment cools the more superficial tissues of the body; therefore, thermal diffusion from the core will continue after removal from the cold environment until an equilibrium between peripheral heat loss and central heat production is re-established. This is probably the reason for the delay in the core temperature increase from the surface rewarming observed in our study. We observed a slight decrease in the core temperature in both groups, and the temperatures would have been expected to return to baseline if the experimental period had been longer than 60 min. There was a slight difference between the groups after 50 min; the core temperature was slightly lower in the intervention group than in the control group. Our research participants were not hypothermic; therefore, it is possible that the active external heat source contributed to cutaneous vasodilation, causing increased blood flow to the cooled tissues, and resulting in a faster decrease in temperature and a shorter time until thermal equilibrium was reached. Thermoregulatory vasoconstriction is controlled centrally by the preoptic area of the hypothalamus. Vasoconstriction in a patient with accidental hypothermia continues despite peripheral heat stimuli by cutaneous rewarming for as long as the core temperature decreases [18]. There is no evidence supporting the historical claim that active external rewarming is dangerous; thus, most guidelines recommend active external rewarming as a treatment option [19,20,21]. The differences observed in our study were too small to be considered clinically relevant, and the study was not designed to detect differences in core temperatures between the groups. Therefore, we considered the relevance and importance of this finding to be negligible.
Although not completely blinded to the intervention, participants reported a higher degree of thermal comfort in the intervention group than those in the control group. Patient comfort is important in mountain rescue, as well as in healthcare. Thermal discomfort exacerbates pain and fear, and shivering is particularly uncomfortable [22, 23]. Providing active external rewarming may increase thermal comfort and the rewarming rate.
One study demonstrated the benefit of combining wet clothing removal before insulating the patient using a vapor barrier, insulating materials, and an outer shell [17]. Wet clothing removal will reduce the amount of thermal energy required to heat the volume of water encased inside the vapor barrier, but usually requires the patient to be undressed and exposed to the elements before being insulated in the wrap. A vapor barrier may still be useful if wet clothing is removed because snow or rain may enter the burrito model during wrapping or there may be residual moisture on the skin resulting is evaporative heat loss for the victim. Rapid, gentle and accurate application of the vapor barrier is essential for its effect. If the barrier is improperly placed, allowing continued vapor escape and heat loss from the model, it loses its function. Appropriate equipment, extensive training, and preparation are required for rescue services to achieve adequate insulation and patient protection without excessive movement of the patient.
Bubble wrap is frequently used as a vapor barrier material because it is believed to provide both a water-impermeable barrier and some level of insulation. However, the insulating properties of bubble wrap are limited, and the pack volume is large [9]. Consequently, rescue services should consider other waterproof materials with smaller volumes to achieve a similar performance.
Limitations
In our study, we wrapped participants in the “burrito” model without removing their wet clothes. The removal of wet clothing may sometimes be advisable, and the combination of wet clothing removal and the use of a vapor barrier can be beneficial compared to only retaining water inside the model. The aim of our study was to evaluate the isolated effect of a vapor barrier, and not to compare the effectiveness of the two methods. Therefore, we chose not to remove the clothing to ensure a more consistent amount of water in the model. This approach achieves better standardization and increased internal validity than the other. However, this may be at the expense of external validity, as in a real-life scenario, the combination of wet clothing removal and the use of a vapor barrier could be beneficial. It is also important to note that in a real-life scenario, placing the heat source closer to the patient than demonstrated in our study would probably be advisable.
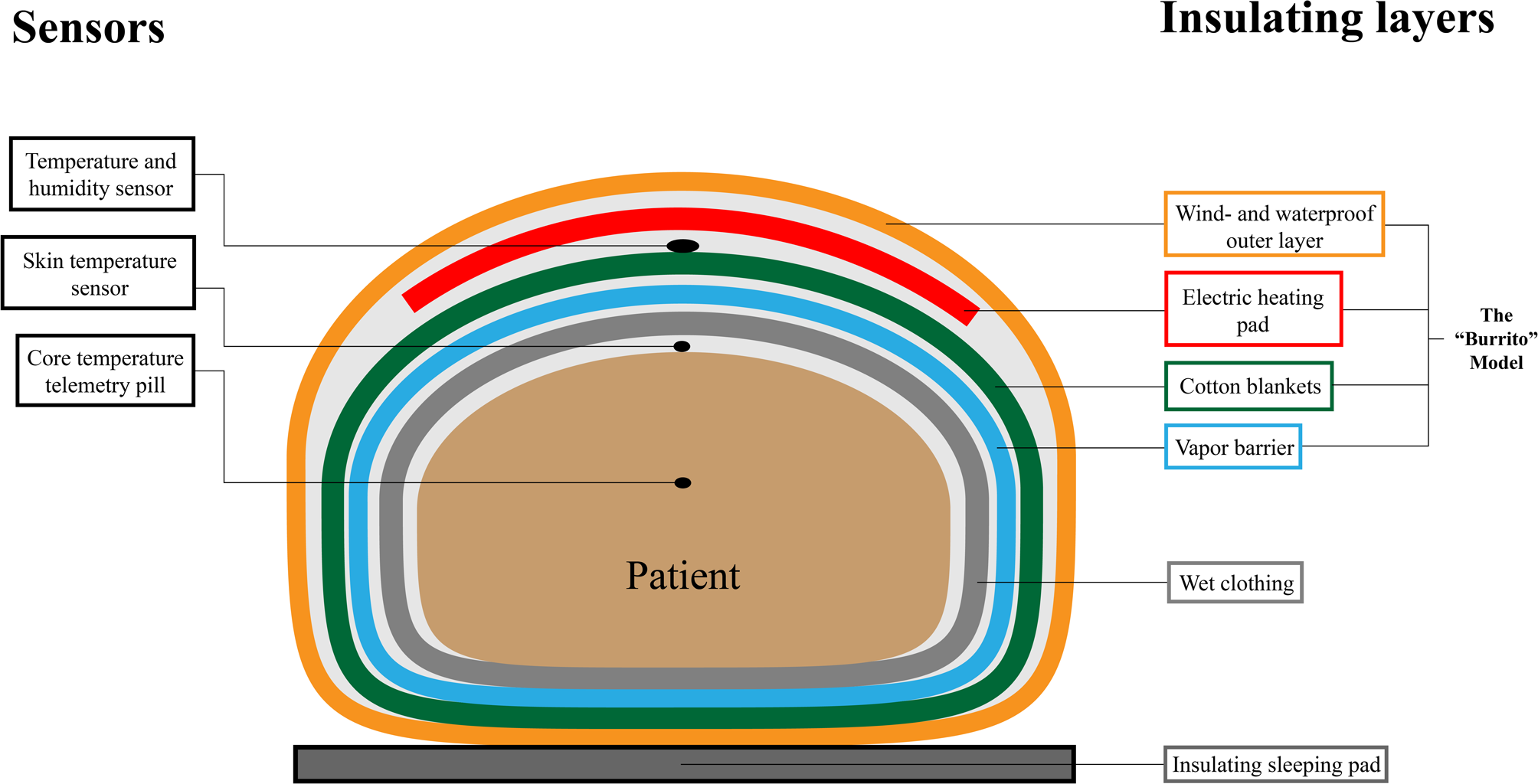
The vapor barrier used in our study (ASAP JONA 200) has a semi-permeable membrane (1213 g/m2/24 h) which may allow some vapor to escape over time. However, as shown in Fig. 3, the product worked as intended and we achieved a low and stable humidity outside the barrier. Since the objective of this study was to evaluate the general principle of limiting evaporation, and not to investigate specific products, we believe our results to be valid. It is also possible that the absorbing qualities of this blanket may have had an impact on the measured outcome.
Cotton blankets are not the optimal source of insulation in a mountain rescue scenario, and other materials such as wool, down, Primaloft or other would probably have yielded higher rewarming rates. However, we do not believe that it would significantly affect the results of our study as our primary goal was to evaluate the effect of eliminating evaporative heat loss, and the amount of insulation was identical in the two scenarios.
Another potential limitation of our study is that the outer layer of our model was impermeable to water vapor, creating an additional vapor barrier at the exterior of the model. This is in accordance with the guidelines for the care of patients under harsh conditions, where a wind and waterproof outer shell is recommended.
Lastly, an important limitation of our study is that water distribution in the garments may not have been complete. It is difficult to assess the impact this may have had, as uneven water distribution may have contributed to regional differences in skin temperature. However, there is no reason to believe that this affected one group of individuals differently from others.







留言 (0)