
記住我





48, XXYY syndrome, as a rare sex chromosome disorder, was first described in 1964. It is estimated to occur in 1:18,000–1:40,000 male births. It presents with a wide variety of physical, psychosocial, and neurocognitive findings. Most of the literature currently focuses on the physiological and psychological disorders of the 48, XXYY phenotype. The wide spectrum of symptom variability is considered to be related to sex chromosome dosage and skewed X-inactivation, but further investigation is still needed to understand these underlying genetic variations and their connection to clinical signs and symptoms [1].
There are few reports of ocular abnormalities in association with 48, XXYY syndrome with only three known cases to date that detail ocular complications, including strabismus, Duane’s syndrome, and retinal dysfunction [5, 11, 13]. Only a single case has been reported wherein high myopia was associated with 48, XXYY syndrome [5]. In that case, bilateral poor visual acuity (BCVA LogMAR 1.0, Snellen 20/200) was found, which was align with the findings from our patient. Notably, although our patient did not exhibit the bilateral extinguished ERG response documented in the previous report [4, 7]. there was a significantly reduced amplitude in light-adapted and flicker ERG.
In this study, we present the case to describe macular dysplasia in a patient with 48, XXYY syndrome. The absence of the foveal pit, protrusion of the inner retinal layer, and elongation of the outer segment were noted on optical coherence tomography with increased vessel density with reduction of the foveal avascular zone on OCTA. Chen etc. reported a case of macular dysplasia with 48, XXYY syndrome. In their study, the degree of macular hypoplasia in patients was less severe than in our case, with better visual acuity, and there was no description of the refractive status [2]. The severity of macular dysfunction and poor BCVA was correlated with the degree of macular dysplasia and high myopia observed. Posterior staphyloma and pronounced choroidal atrophy were also noted. Although both conditions could occur as secondary changes in high myopia patients, such alterations usually require extensive periods to manifest. Given these findings, we propose that fundus changes, notably macular hypoplasia, may represent a hitherto feature of 48, XXYY syndrome [6], Table 1).
In 2010, Ottesen et al. examined the influence of sex chromosome genes and the gene dosage effect, potentially accounting for the increased stature [9]. A similar mechanism may apply to the genes linked to myopia, such as MYP1, ARR3, which are located on the X chromosome, suggesting a parallel between the genetic determinants of height and myopia [8, 10, 14].
In summary, we have documented the first reported macular dysplasia in a patient with 48, XXYY syndrome. Our report further expands the clinical spectrum of this disease. The patient’s decreased visual acuity could be attributed to the combined effects of high myopia and macular dysplasia. We postulate that these macular changes, particularly macular hypoplasia, could represent a previously unidentified aspect of 48, XXYY syndrome.
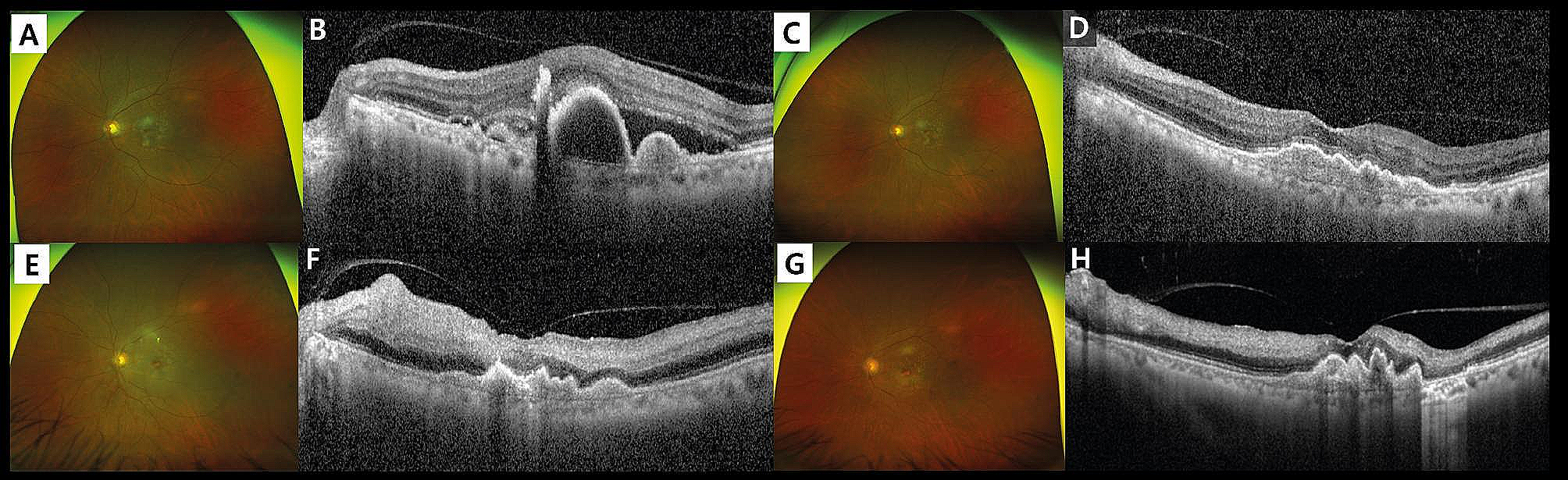
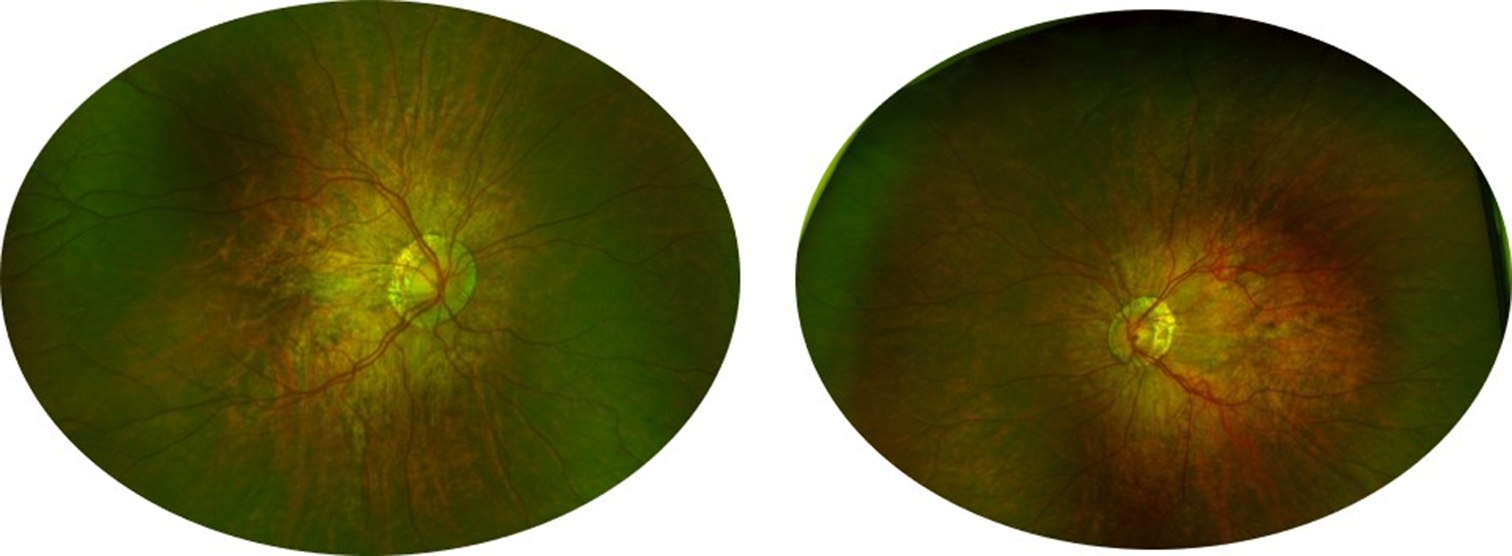
Fig. 1
Fundoscopy showed tessellates fundus, peripapillary and posterior staphyloma.
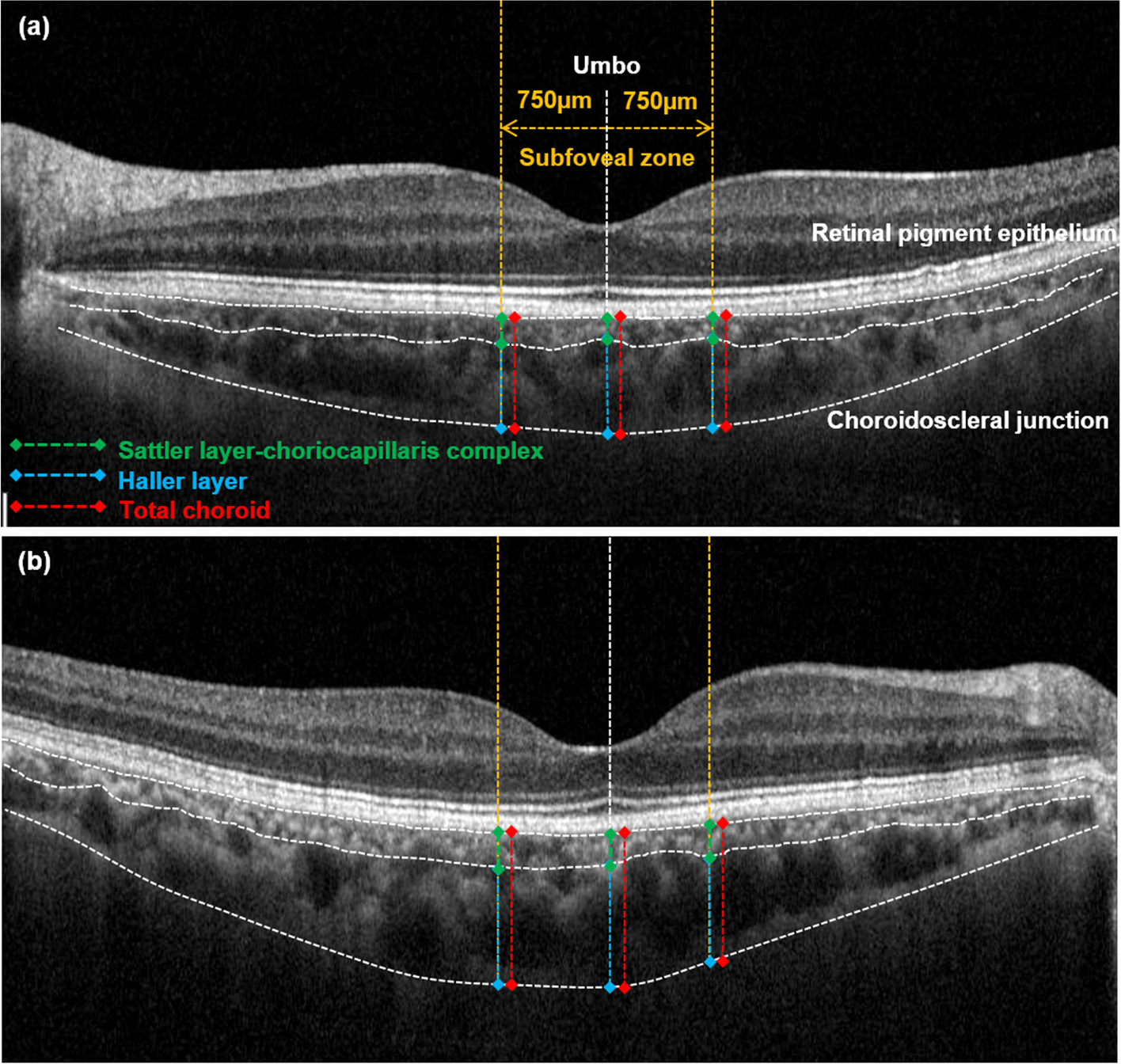
Fig. 2
OCT showed grade 3 macular hypopiasia, extreme choroidal atrophy and staphyloma formation bilaterally.
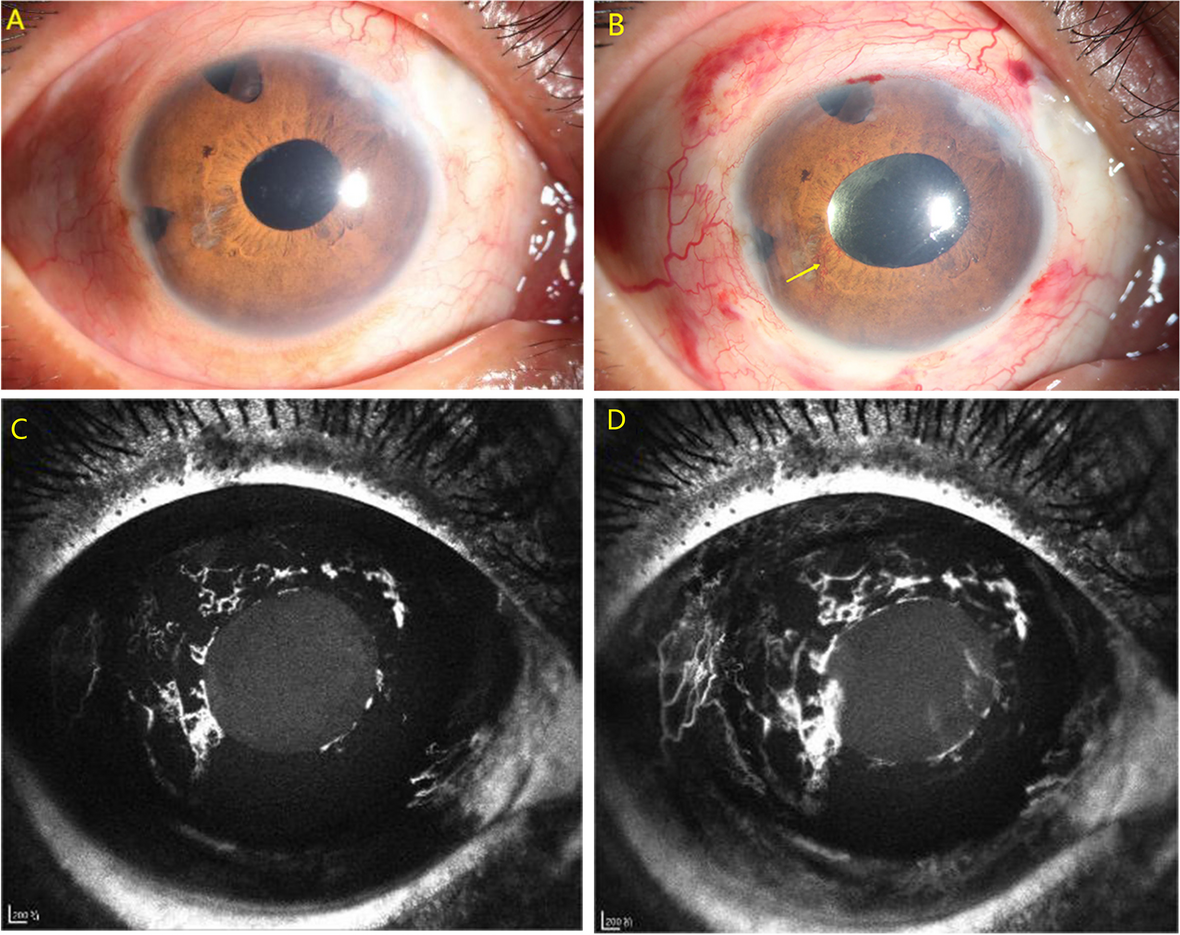
Fig. 3
Optical coherence tomography (OCTA) showed increased vessel density with reduction of the foveal avascular zone bilaterally.
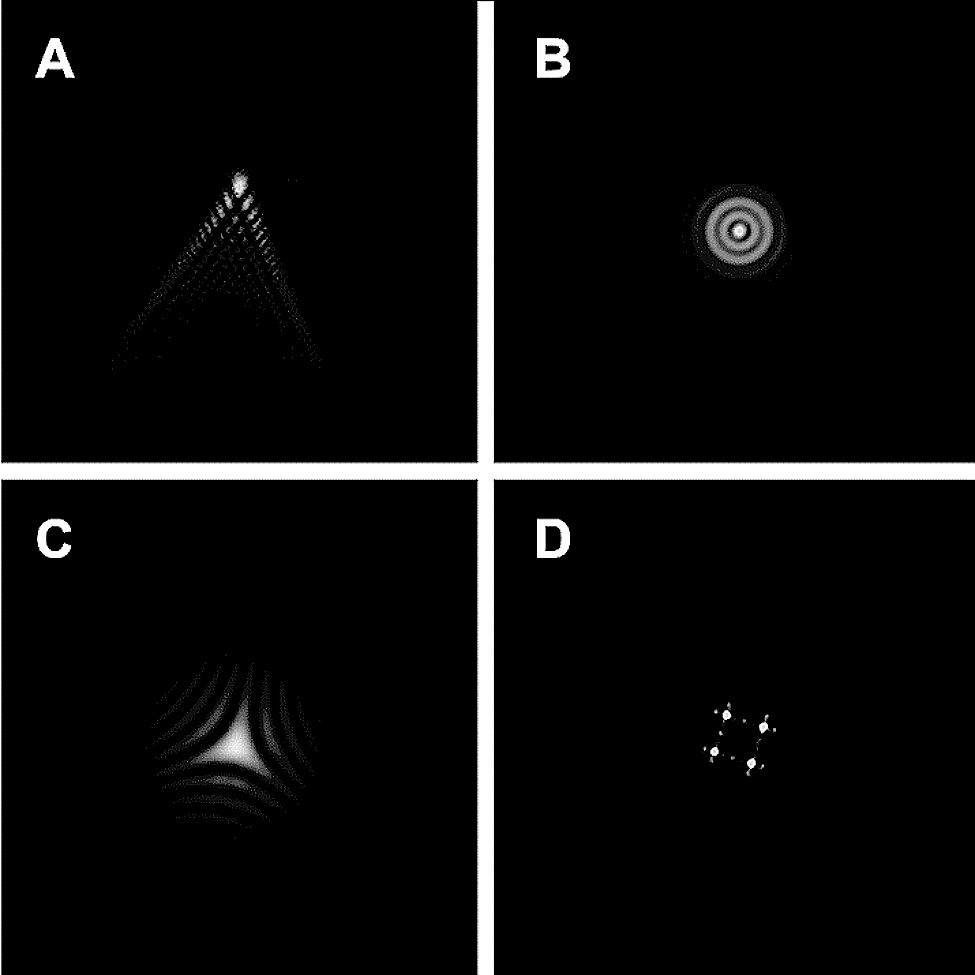
Fig. 4
Dark-adapted 0.01 ERG and Dark-adapted 3.0 ERG ahowed allghtiy peak time delay on the right eye (A-B). Light-adapted 3.0 ERG and Light-adapted 30 Hz ERG showed algnificantli reduced amplltude bllaterally, while peak time delay on the right eye (C-D).
Table 1 Ocular clinical characteristics of 48, XXYY syndrome in previous studies
留言 (0)