Brolucizumab is a single-chain antibody fragment binding to VEGF-A and blocking the activation of angiogenic signal transduction [5]. Being an anti-VEGF agent with a smaller molecular weight, compared to other previously approved VEGF antagonists for nAMD, there was anticipation that brolucizumab would hold an advantage over its counterparts. In a preclinical study on non-human primates, brolucizumab showed favorable tissue penetration rates in the retina and RPE/choroid at 42% and 18%, respectively, compared to intravitreal concentrations after vitreous injection [3]. Due to its superior solubility and stability, it was expected to be able to deliver a higher concentration compared to other anti-VEGF agents, thereby enabling prolongation of the injection interval and the potential to alleviate the burden with less frequent injections [1, 2]. According to HAWK and HARRIER clinical studies for 96 weeks, the brolucizumab injection group showed non-inferiority on BCVA and better anatomical outcomes than the aflibercept injection group [4].
However, these initial expectations were overshadowed by concerns, as a strong correlation emerged between brolucizumab and IOI, including a few cases of retinal vasculitis with or without RAO. The occurrence of IOI following the administration of a conventional anti-VEGF agent has been reported [6]. In the HAWK and HARRIER studies, however, the brolucizumab injection group had a significantly higher incidence of IOI at 4.7%, compared to the aflibercept group which had a much lower rate of 0.6% [4]. Similarly, Saba et al. reported that the incidence of IOI was comparable at 4.8% in the 8-month post-marketing surveillance analysis [7].
Most of the reported IOIs were iritis and uveitis, which could subside spontaneously or be reduced after topical or periocular steroid treatments. Visual prognosis of most patients who underwent IOI revealed relatively good during the follow-up period [4]. However, there were several cases with relatively poor visual prognosis, such as retinal vasculitis with RAO [4, 7,8,9]. A retrospective analysis of 26 eyes from 25 patients evaluated retinal vasculitis following the administration of brolucizumab, and 92% of cases of retinal vasculitis were accompanied by anterior chamber inflammation and/or posterior segment inflammation [8]. Among them, occlusive vasculitis was reported in 85% of the eyes. Most cases of retinal vasculitis showed improvement with steroid treatment, but some cases with RAO exhibited limited response even with steroid treatment [8].
Ocular arterial thromboembolic events reported in HAWK and HARRIER studies occurred in a total of 10 cases in the brolucizumab 6 mg injection group, and seven of which occurred concurrently with IOI, compared to 3 cases in the brolucizumab 3 mg injection group [4]. Patients in all IOI cases had cardiovascular risk diseases such as hypertension and cardiac arrhythmias as underlying diseases [4]. In a previous report, Sentaro et al. suggested a possibility that retinal vascular occlusion after brolucizumab injection could occur without vasculitis and IOI [9]. As it is well known that VEGF itself plays an important role in maintaining vascular endothelial cell integrity, it is thought that the VEGF inhibitor itself may interfere with the physiologic function of the vessel and cause occlusion [10, 11]. The mechanism explaining RAO after anti-VEGF injection still has not been fully elucidated. It has been proposed that the relatively potent and long-lasting VEGF inhibitory effect of brolucizumab may lead to the damage of retinal vascular endothelial cells, consequently resulting in retinal vascular occlusion [9]. Unfortunately, a possibility of the association with cardiovascular embolism risk has not been evaluated in this case, because the patient did not want an additional assessment.
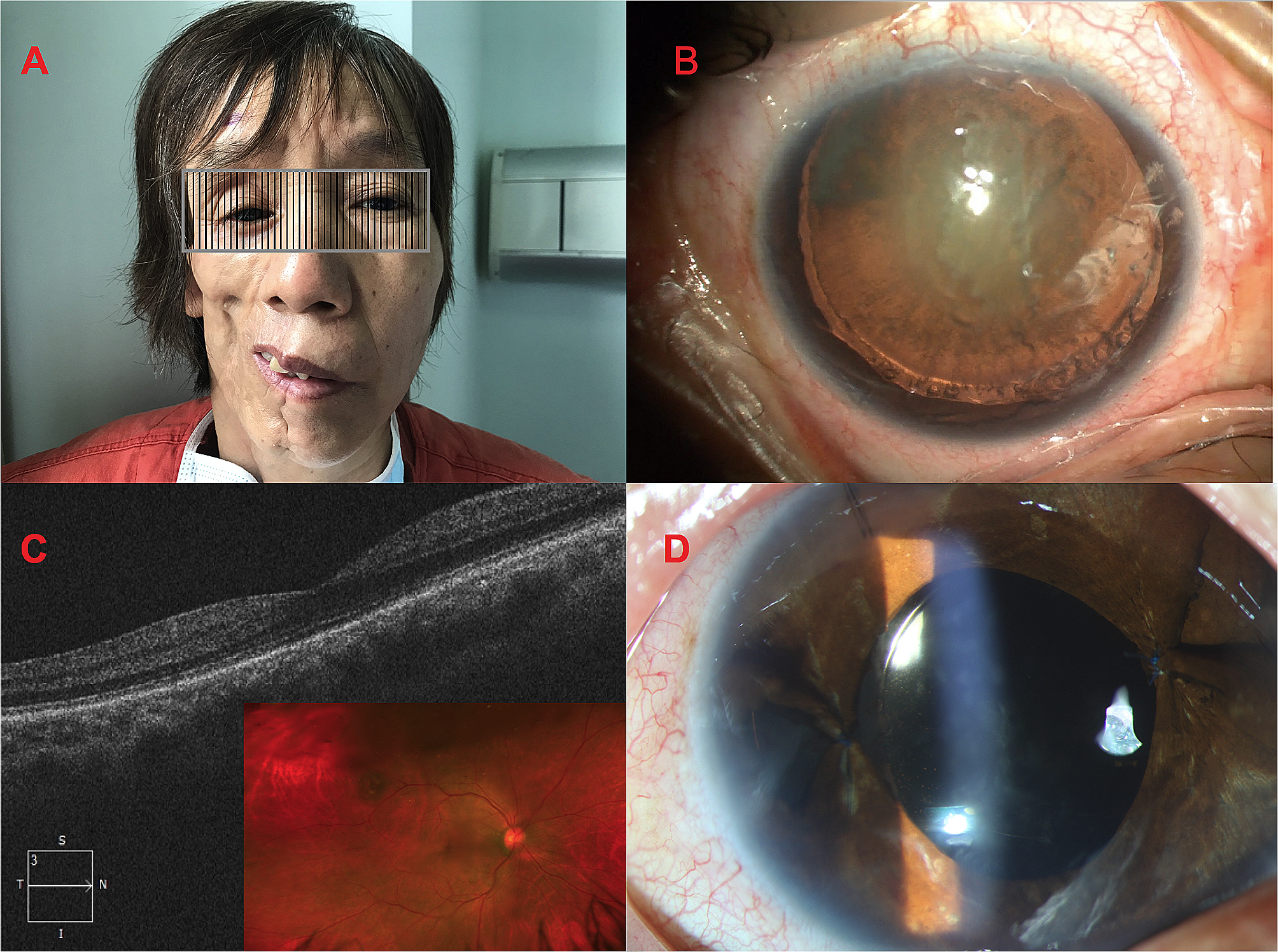
In this case, the patient presented typical CRAO findings two days after administering the third monthly injection of intravitreal brolucizumab. Unlike other RAO patients previously reported after injection of brolucizumab, the patient had no underlying cardiovascular disease such as hypertension, diabetes, or dyslipidemia. In addition, there was no gross evidence of IOI in the comprehensive ophthalmologic examinations performed before or after the occurrence of CRAO, and there was no improvement even with a steroid treatment. It is thought that there is a possibility of occlusive vasculitis due to the presence of microscopic or minimal inflammatory signs, which could be detected under retinal imaging tools such as fundus photography or FFA.
Although the incidence can be rare, this case shows the possibility of retinal vascular occlusive events without definite evidence of IOI in eyes without cardiovascular risk factors for RAO. Since the visual prognosis after the occurrence of CRAO is poor, the possibility of CRAO after intravitreal brolucizumab treatment should always be in consideration and careful observation is required during the short-term follow-up period after the intravitreal brolucizumab injection for nAMD patients with old age, even if the patient does not have any other comorbid cardiovascular disease history.







留言 (0)