
記住我
This research conducted at Razi Hospital, Ahvaz, Iran, between September 2021 and March 2022, involved a double-blind, randomized clinical trial on COVID-19-infected patients who were hospitalized in the infectious ward. In order to qualify for involvement, people were required to fulfill the following conditions: be aged between 18 and 70 years, have received a verified COVID-19 diagnosis via a positive RT-PCR test, nasopharyngeal swab, experiencing respiratory symptoms (such as breathlessness, chest discomfort, and sensations of pressure) with or without an accompanying fever (equal or more than 38 °C) and Spo2 between 90% and 93%. Patients with moderate disease severity were included in this study. Patients who were critically ill and were hospitalized in the intensive care unit (ICU) or had a mild illness and did not need to be hospitalized were not included in the study.
Other inclusion criteria include absence of pregnancy and breastfeeding, without history of diabetes, high blood pressure, heart disease, kidney dysfunction, and psychological disorders like depression, Body mass index less than 35 and more than 18, Vitamin D level above 30 ng/ml, absence of hypomagnesemia that refers to a deficiency in magnesium levels (below 1.7 mg/dL) and hypermagnesemia signifies an excess of magnesium levels (above 2.6 mg/dL), and absence of alcohol and drug abuse. Exclusion criteria included unwillingness to continue participating in the study, hospitalization of the patient in the ICU, Taking antioxidant and anti-inflammatory food supplements such as vitamin E, omega 3, vitamin D, etc. and contraindication, intolerance or allergy to magnesium supplement.
The sample size calculation was based on a previous study by Tan et al. [31] which reported a 60% reduction in the proportion of cases requiring oxygen therapy in the intervention group compared to the control group. With a power of 80%, alpha level of 0.05, and estimated proportions of 61.5% in the control group and 24% in the intervention group, the sample size was determined to be 25 individuals per group. Considering a 20% attrition rate, the final sample size comprised 30 individuals in each group.
$$}\,}\,}_} - }$} \!\mathord} }}}\right.\kern-\nulldelimiterspace}\!\lower0.7ex\hbox}$}}} \right)}}\,}\,}_} - }} \right)}}} \right)}^2}\left[ }_}}\left( } - }_}}} \right)\,}\,}_}}\left( } - }_}}} \right)} \right]} \over }}_}}}}}^}}}}$$
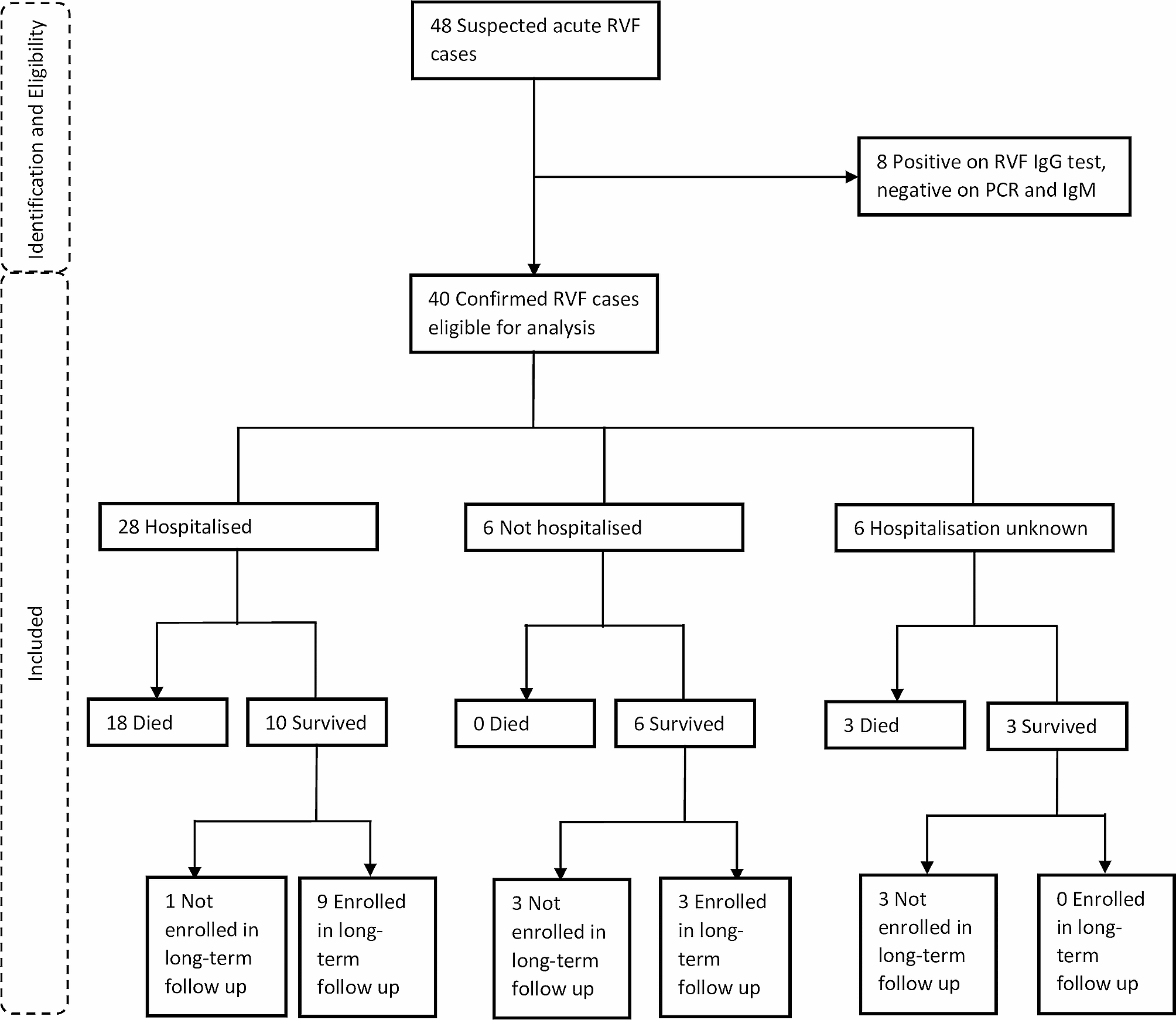
The general scheme of the intervention is shown in Fig. 1. The method of assigning patients to the intervention and control groups was the approach of employing randomized permutation blocks with a block size of 4 (referring to the table associated with random permutations). The participants were randomly allocated in a ratio of 1:1 to the intervention and control group. A computer-generated list was created using random permuted blocks to ensure that the allocation to subjects and investigators remained concealed. The intervention and placebo were kept hidden from researchers, patients, infectious disease specialist and clients. Magnesium supplements and placebo were completely similar in terms of appearance, color, fragrance, and packaging, so that the blinding process could be fully implemented.
Fig. 1
Flowchart of the study protocol
At the study’s inception, the researchers thoroughly briefed the patients on the process of implementing the study and all participants provided written informed consent to partake in the study. Patients had the option to exit the study at any point if they were unwilling to cooperate. The study was conducted in compliance with the Declaration of Helsinki and the protocol of the research was approved by the ethics committee of Ahvaz Jundishapur University of Medical Sciences (Ethical code: IR.AJUMS.REC.1400.0255) and This study is registered on Iranian Registry of Clinical Trials (IRCT) under identifier IRCT20210413050957N1. (The registration date: May 1, 2021).
InterventionParticipants within the intervention group were provided with 300 mg of oral magnesium supplement in the form of magnesium citrate capsules daily, and subjects in the control group received a placebo containing starch. Magnesium citrate powder was obtained from Behan Sar Pharmaceutical Company, and capsules containing magnesium and placebo were prepared by an expert at the Faculty of Pharmacy of Jundishapur University and provided to the study. The placebo capsules contained starch and were similar in appearance to magnesium supplements. The duration of intervention in patients was from the time of admission to the time of discharge from the hospital. In case of changes in the diet and medication protocol of the patients, the changes were reviewed by the research team, and in case of interference with the study objectives, the patient was excluded from the study.
Data about the physical dimensions of the body and past medical recordsInformation pertaining to age, weight, height, past medical conditions, prescribed medications, blood pressure, serum lipids, random blood glucose, and respiratory condition was obtained by examining medical records.
Dietary intakeNutritional intake of patients was done by recording of 24-hour dietary recall at both the start and conclusion of the research. The N4 software was utilized to analyze data on dietary intakes, with national food composition tables serving as a reference for the analysis of food intake.
Primary and secondary outcomeThe confirmatory result of this study was the number of patients who needed oxygen therapy. Secondary outcomes included SaO2, respiratory rate, fever, hs-CRP and TNF-α levels, the well-being and psychological state of individuals’ lives and mental health.
MeasurementsTo measure biochemical variables, 7 cc of blood were taken from the patients at the beginning of the study and on the day of discharge from the hospital. Diaclone Research’s ELISA kits from Besançon, France were employed to evaluate the levels of hs-CRP and TNF-α concentration. To assess serum magnesium concentration, the measurements were conducted using an auto-analyzer utilizing a photometric method (BT-3500, Biotecnica Instruments, Rome, Italy) using Biosystem Kits (Barcelona, Spain). Depression status of patients was measured by Beck Depression inventory-II (BDI-II). The research conducted by Hamidi and colleagues, Persian version of the questionnaire was utilized, demonstrating satisfactory validity (alpha = 0.92) and reliability (r = 0.64) [32]. Individuals participating in the study filled out a self-report inventory consisting of 21 items. The items were rated on a scale of 0–3, where a higher score indicates more severe symptoms. The total score of the questionnaire is then classified into the following categories [33]: for scores ranging from 14 to 19, it indicates a mild level of depression. Scores between 20 and 28 suggest a moderate level of depression, while scores between 29 and 63 indicate a severe level of depression. The patients’ anxiety was evaluated by Spielberger State-Trait Anxiety Inventory (STAI). In Abdoli et al.‘s study, the Persian version of the questionnaire was employed, indicating acceptable validity (alpha = 0.88) and reliability (r = 0.64) specifically for measuring state anxiety [34].
The researchers employed the SF-36 questionnaire to evaluate the quality of life of individuals in this study. The SF-36 is a frequently employed survey that individuals fill out on their own, providing a comprehensive assessment of their quality of life related to health. It consists of 36 items grouped into eight subscales, which are further classified into two broad components: the physical component summary (PCS) and the mental component summary (MCS). The physical component summary comprises evaluations of 10 items related to physical functioning, 4 items related to role-physical, 2 items related to bodily pain, and 5 items related to general health perceptions. The mental component summary comprises the following subscales: social functioning (2 items), role-emotional (3 items), mental health (5 items), and vitality (4 items). Additionally, there is a single item that separately assesses changes in health. The scores for all items are assigned numerical codes, summed together, and then transformed into a scale ranging from 0 to 100. In this scale, a score of 0 represents the poorest condition, while a score of 100 indicates the best condition [35]. In 2006, Montazeri et al. conducted a study in Tehran, Iran, to validate the SF-36 questionnaire among a healthy population aged 15 years and above. The study confirmed the reliability of the questionnaire by calculating Cronbach’s alpha coefficients, which ranged from 0.77 to 0.90 for the subscales and the overall scale [36].
Statistical analysesThe quantitative data were expressed as the mean value accompanied by the standard deviation. On the other hand, qualitative data was presented in the form of percentages and numerical counts to describe the status of these measurements. The Kolmogorov-Smirnov test was employed to validate the normal distribution. The study employed the Independent T-test and chi-square test to evaluate and draw comparisons between groups’ results at the beginning and conclusion of the study. Changes from the initial baseline were analyzed within each group using a paired samples t-test. The analysis of covariance (ANCOVA) test was used to account for confounding factors. All ANCOVA models were adjusted for weight, serum magnesium levels at baseline, and calorie intake. The data underwent analysis with SPSS19 software, and if the P-value was less than 0.05, it was deemed statistically significant.
留言 (0)