
記住我
This retrospective study included women who tested 52 positive for HPV viral load between January 2020 and December 2022 at Yuebei People's Hospital. The Ethics Committee of Yuebei People's Hospital gave the go-ahead to the research, which was done in line with the Declaration of Helsinki and its associated rules and regulations. All patients signed a written informed consent form before the examination. As a retrospective study, the clinical data of patients were obtained from the HIS system of Hospital. The data collection process was confidential, and sensitive information of the patients was anonymized during the collection and analysis process, and there were no costs or additional risks to patients.
Inclusion criteria were (1) HPV DNA52 positive patients (2) Patient had TCT results for the same period of time. Exclusion criteria were (1) patients with high-risk HPV16 and/or HPV 18 co-infection. (2) Incomplete information.
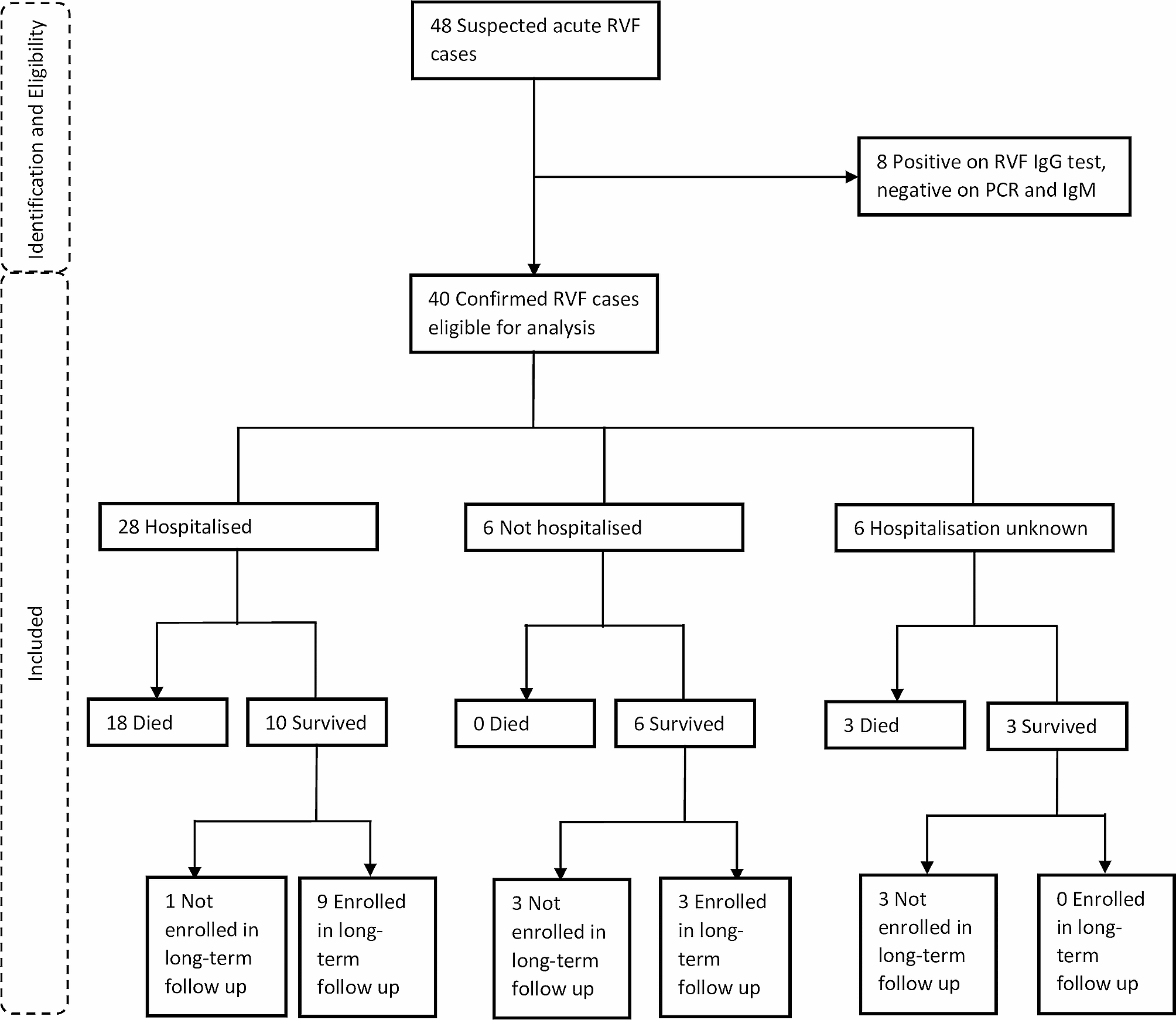
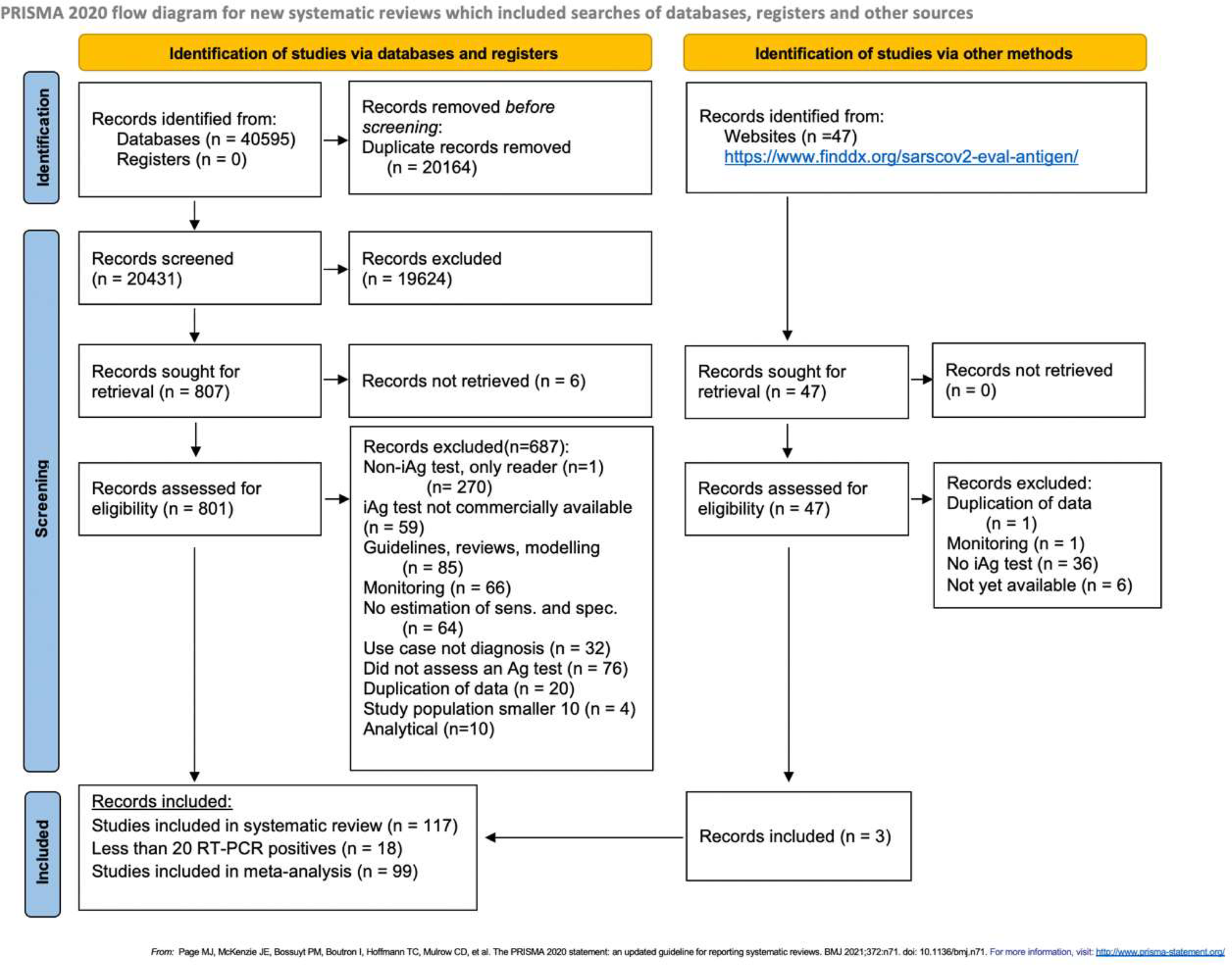
Between 2020 and 2022, a total of 1882 female patients who underwent HPV quantitative testing at Yuebei People's Hospital tested positive, with 533 of them testing positive for HPV52. We omitted 40 patients who tested co-positive with HPV16/18, and we removed 5 patients whom HPV52 viral load could not be calculated. In the end, a total of 488 patients were incorporated (Fig. 1).
Fig. 1
This flow chart that screening the participants in this study
Data collection and groupingClinical data such as patient's age, HPV52 viral load, viral load of other types (without this data it is a single infection), and contemporaneous TCT results were obtained from clinical record through Yuebei People's Hospital's HIS system.
HPV Genotyping and Viral LoadThe HPV genotyping test kits applied by Yuebei People’s Hospital was provided by 21 HPV genotyping Kit (Shuoshi Biotechnology, Ltd., China, Jiangsu), The test kit was approved by the National Medical Products Administration (NMPA, No. 20153400364). The kit adopts multiplex fluorescent PCR quantification technology, which can rapidly and accurately distinguish 21 HPV genotypes in the test specimen, including 13 HR-HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, intermediate-risk HPV26, 53, 66, 73, 82, and 3 low-risk HPV6, 11, 81, and also simultaneously quantify the viral loads of the 21 HPV subtypes in a standardised manner.
This Kit targets the L1 region of the human papillomavirus genome, using PCR primers and corresponding TaqMan probes (oligonucleotides with a 5' reporter group and a 3' quencher group) for detection, with FAM, HEX and ROX marking the respective subtypes, and running 8 reactions simultaneously for each sample. The preparations for reactions A, B, C, D, E, F and G are used for the simultaneous detection and differentiation of 21 HPV genotypes. In reaction H, t the single-copy gene TOP3 encoding DNA topoisomerase III is amplified as a control to determine the viral copy number in a given sample. The sensitivity of the assay is 20copies /reaction.
Sampling and extract the sample DNA according to kit requirements. The total reaction volume is set to 20 μL, consisting of 2 μL DNA sample, 10 μL nucleic acid amplification reaction liquid, and 8 μL reaction liquid (including specific primers and probes). After mixing all the components, the reaction tube is placed in a fluorescence PCR amplifier for amplification detection. The reaction conditions 77 were as follows: treatment of UNG enzyme at 50 ℃ for 5 min, pre-denaturation at 95 ℃ for 10 min, denaturation at 94 ℃ 78 for 10 s, annealing, extension and fluorescence detection at 58 ℃ for 40 s, cycling 45 times, and storage at 4 ℃.
Finally, subtypes were analyzed according to the HPV subtyping probe fluorescent marker table. The obtained CT values were substituted into the HPV nucleic acid typing quantitative analysis software v1.0 (Shuoshi Biotechnology, Ltd., China, Jiangsu) for transformation. Absolute quantification was mainly performed by establishing a five-point standard curve of HPV and cell log phase. The standard curve was Y = -3.34656 (log10X) + 38.51644. the converted viral load unit was the number of cells (pcs).
ThinPrep cytology test(TCT)Cervical ThinPrep cytology test was interpreted by two senior specialists in the pathology laboratory. The diagnostic results of the TCT were classified according to the Bethesda system by the International Cancer Society (2014), Results were categorized into five classes: negative for intraepithelial lesion or malignancy (NILM), atypical squamous cells of undetermined significance (ASCUS), atypical squamous cells–cannot exclude high-grade squamous intraepithelial lesion (ASC-H), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion(HSIL) and squamous cell carcinoma (SCC). There are 6 cases of ASC-H,5 cases of HSIL and 1 case of SCC. Since there were too few cases and those results need to be referred for the next step of colposcopic biopsy, so we merged them into the TCT results of HSIL. To further validate the relationship between HPV52 viral load and TCT, we divided four categories into two groups for comparison. Given the specificity of ASCUS, it can either indicate a benign lesion or signify a potentially malignant alteration associated with active proliferation. So we grouped TCT subgroups were stratified into groups: one is TCT results of ASCUS or better; the other is TCT results of LSIL or worse.
Statistical analysisSPSS 24.0 (IBM, Armonk, NY, USA) and R language software was used for data processing and statistical analysis. TCT results were used as grouping variables to describe the study population. Age and log-transform-processed HPV52 viral loads were normally distributed continuous variables, quantitative data were expressed as mean ± standard deviation. The type of HPV infection was a categorical variable and was expressed as a percentage. Differences between groups were evaluated using the ANOVA and Kruskal Wallis rank sum tests. p-values < 0.05 were considered statistically significant.
The HPV52 viral load data showed a skewed distribution among the participants, therefore, we processed the HPV52 viral load by log transformation. The results of data analysis were divided into 3 models: model 1 (no covariates were adjusted); model 2(adjusted age); and model 3 (adjusted age and infection types). Confidence intervals (CI, 95%) and odds ratios (OR) were used to screen the adjusted covariates included in the models, while univariate analysis of p values did not yield the same results. A generalized additive model was used to adjust for all covariates, assess nonlinear relationships, and plot smooth curves. In the presence of nonlinearity, we employed a recursive algorithm to determine the inflection point. Then a segmented linear model was constructed based on both sides of the inflection point. The p-value of the log-likelihood ratio test was used to construct the best-fit model. If the p-value was ≤ 0.05, the correlation between viral load and TCT was nonlinear, otherwise it was linear. In the single infection curve, we got two inflection points K1 (8.95); K2 (11.35) (Table 5). In the multiple infection curve, there is only one inflection point K3 (12.095) (Table 6). Multiple infections include both (non-16/18) high-risk and low-risk HPV types.
留言 (0)