CIRT presents a promising treatment option for HCC, particularly for patients with unresectable HCC [7,8,9,10]. In Japan, CIRT is already covered by the Japanese health insurance system for HCCs larger than 4 cm. To date, no study has predicted RILD after CIRT, and, therefore, estimating the risk of RILD or preventing serious RILD has been challenging. To the best of our knowledge, this is the first study to determine pretreatment Child–Pugh score B and VS30 < 739 cm3 as risk factors for RILD due to CIRT. Moreover, our study showed that the one-year cumulative incidences of RILD stratified by Child–Pugh class A or B and VS30 < 739 cm3 or ≥ 739 cm3 were 10.3% or 51.8% and 39.6% or 9.2%, respectively. Our findings demonstrate that adhering to the dose constraint of VS30 ≥ 739 cm3 can effectively prevent RILD, providing valuable insights into planning CIRT treatment.
Although there are no reports on the risk of RILD due to CIRT, there are some reports on the risk of RILD after X-ray SBRT or proton beam radiotherapy. Previous studies on SBRT-induced RILD have reported various risk factors, such as V15, VS10, pretreatment Child–Pugh score, mean liver dose, high doses to 800 cm3 of the liver, and lower platelet count [11,12,13]. Hsieh et al. evaluated proton radiotherapy-induced RILD and reported GTV, pretreatment Child–Pugh score, and unirradiated liver volume/standard liver volume as significant risk factors [18]. In the present study, the pretreatment Child–Pugh score and VS30 of the liver were identified as significant risk factors for RILD after CIRT. While direct comparisons between CIRT, proton, and X-ray treatments are challenging because of the differences in radiation quality and dose fractionation, the pretreatment Child–Pugh score consistently emerges as a risk factor for RILD. Moreover, a dose constraint of VS15 ≥ 700 cm3 has been proposed for SBRT according to QUANTEC [18], supporting our finding of VS30 ≥ 739 cm3.
In the past, RILD due to X-rays was classified into classical and non-classical RILD [19]. Classical RILD, which presents with hepatomegaly, anicteric ascites, and elevated alkaline phosphatase, occurs following whole liver irradiation or conventional RT; however, SBRT-induced RILD belongs to the non-classical category. The symptoms of non-classical RILD vary based on SBRT or proton therapy, with the most common and the primary definition considered in this study being a worsening of the Child–Pugh score by two or more points [19]. However, some studies have included criteria such as hepatobiliary enzymes elevated five times above the upper limit of normal or ascites [12, 18]. These differences arise from the absence of a standardized method with high sensitivity and specificity for detecting non-classical RILDs.
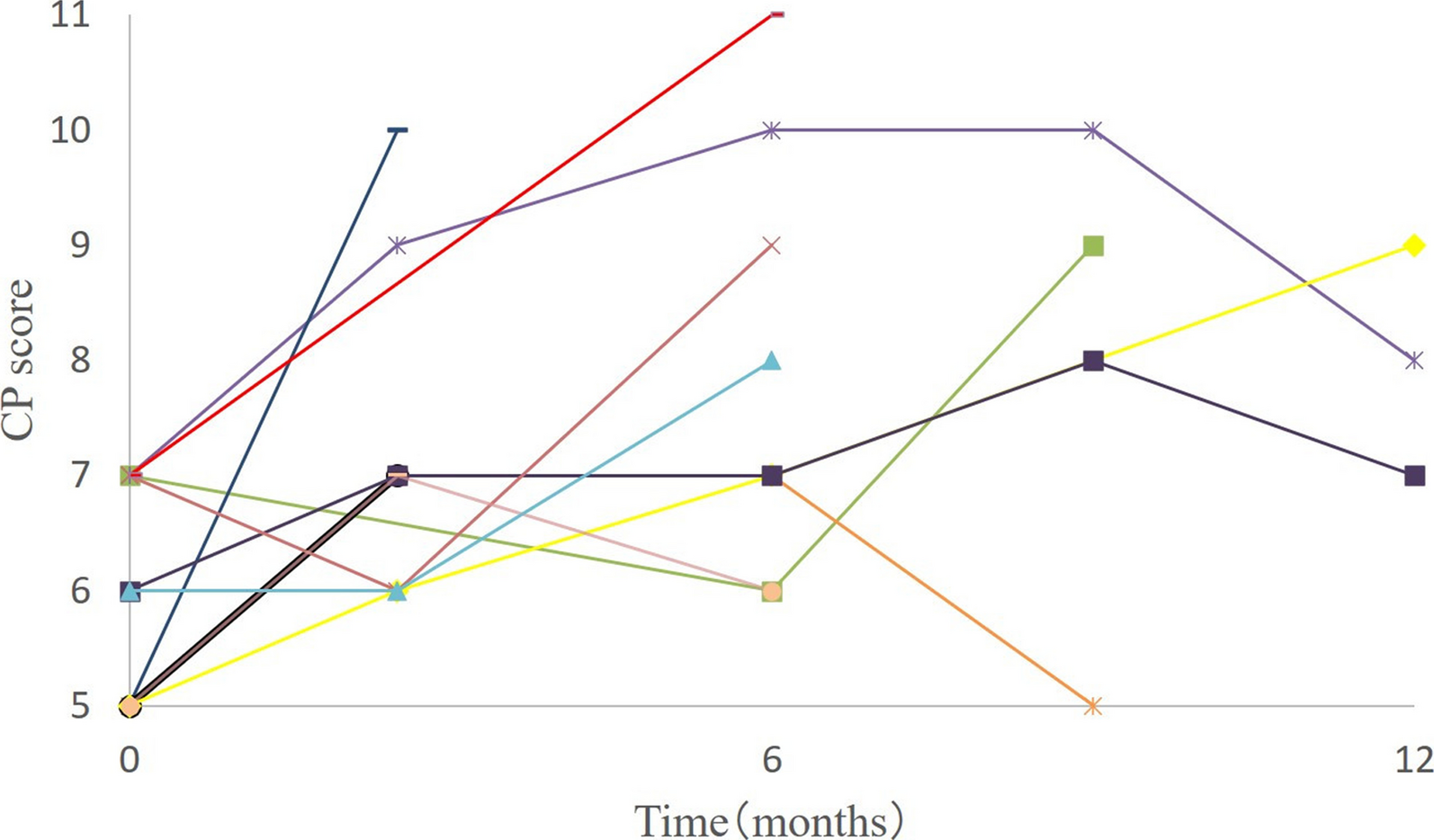
Recovery from RILD has been reported in some cases. Jun et al. reported an improvement in Child–Pugh classification A, but not in B, after SBRT [12]. The present study showed that 43% of patients with pretreatment Child–Pugh classification A showed improvement after RILD, whereas only 25% of patients with classification B showed improvement. These results indicate that recovery from RILD can be difficult; therefore, CIRT must be used to proactively prevent RILD. Although CIRT has shown high local control rates for HCC, new lesions in the liver outside the irradiated field typically recur [7,8,9,10]. In such cases, if RILD from CIRT persists, impaired liver function may complicate definitive local treatments (such as surgery, radiofrequency ablation, SBRT, and CIRT) for new HCC lesions. Therefore, our results suggest that the one-year incidence of RILD can be reduced from 39.6% to 9.2% by setting VS30 ≥ 739 cm3 as a dose constraint in the optimal CIRT treatment planning.
For patients who have undergone treatment for HCC, liver damage can occur for three reasons: HCC recurrence, spontaneous worsening of cirrhosis, and RILD. Patients with HCC recurrence detected after CIRT were excluded from the analysis. In patients with cirrhosis who have maintained Child–Pugh A or B liver function, cirrhosis generally worsens slowly, but RILD occurs within several months of treatment [19]. Therefore, RILD in this study was defined as liver function deterioration within 12 months of CIRT. However, even if the definition of RILD included the time from treatment, spontaneous deterioration of cirrhosis cannot be completely ruled out because both RILD and spontaneous deterioration of cirrhosis are measured using the same Child–Pugh classification of liver damage. Our study has several limitations. First, this was a single-center retrospective study with a small sample size of only 11 cases of RILD. Second, our study included a predefined dose constraint of the volume of the normal liver receiving < 20 Gy (RBE) as > 600 cm3, introducing patient and treatment plan bias. Third, it was difficult to accurately distinguish RILD from spontaneous worsening of liver cirrhosis. Fourth, the number of patients with Child–Pugh classification B was only 10.








留言 (0)