
記住我




A 68-year-old man with a history of hypertension and type 2 diabetes presented to the ophthalmology department with a 2-month history of metamorphopsia and decreased right eye visual acuity. The patient’s systemic blood pressure was 140–150/90 mmHg, and his fasting blood glucose was 6.0–7.0 mmol/L. Two months prior, the patient was diagnosed with retinal detachment in the right eye at another hospital after ocular ultrasound and OCT examination and did not receive any ocular therapy because of severe nephropathy. After that, the patient was admitted to another hospital, diagnosed with membranous nephropathy, ischaemic nephropathy, hypoproteinaemia and anaemia, and started treatment with rituximab transfusion 100 mg + 500 mg every week. Light microscopy analysis of a kidney biopsy sample showed irregular thickening of the capillary basement membrane. Immunofluorescence revealed a roughly granular pattern, with IgA, IgG, IgM, C3, λ light chain and κ light chain subepithelial staining. The patient’s serum haemoglobin level was 99 g/L (normal, 129–160 g/L), and his total serum protein level was 37 g/L (normal, 60–80 g/L). In addition, the patient complained of sudden vision loss in the right eye during therapy for membranous nephropathy approximately 45 days prior.
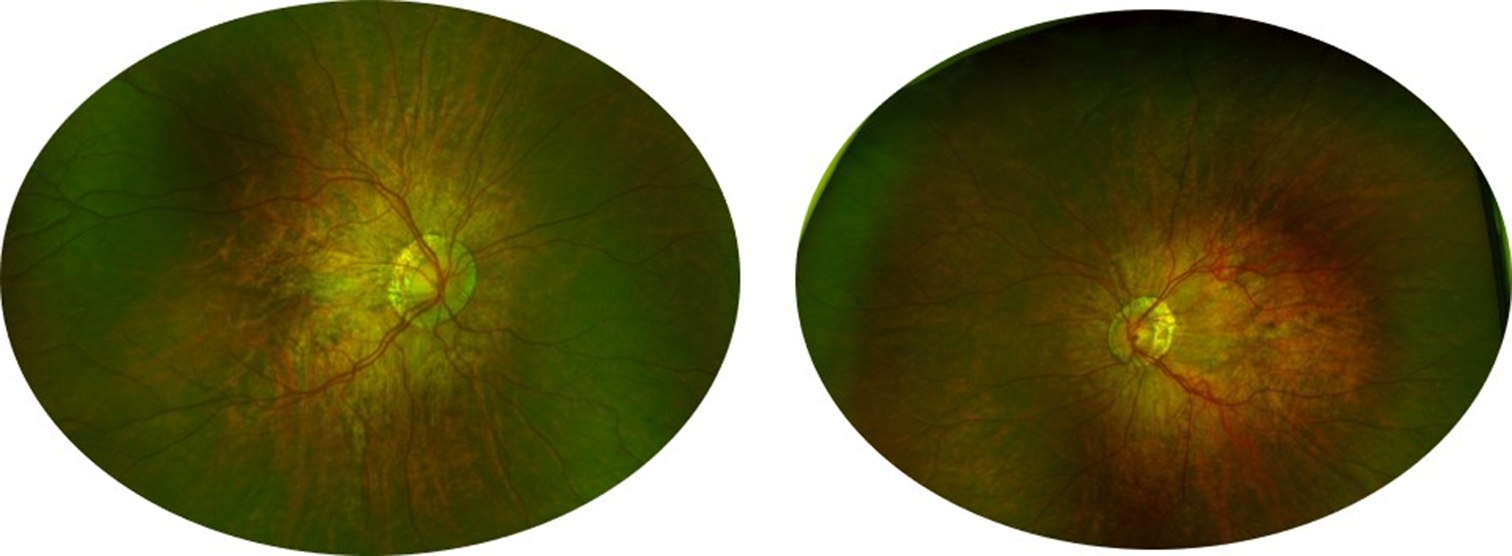
At this visit, the best corrected visual acuity (BCVA) was < 20/800 in the right eye and 20/200 in the left eye. Intraocular pressure was measured at 18 mmHg in the right eye and 16 mmHg in the left eye. The patient had ptosis and poor vision in the left eye since childhood, and the patient had undergone cataract surgery on his right eye 2 years prior; subsequently, normal pupillary and anterior segment examination findings were noted in each eye. A dilated fundus examination of the right eye revealed a bluish grey change at the temporal half of the retina, and an area with rich pigment at the inferotemporal part of the retina. The fundus of the left eye was not clear because of cataract, and yellowish white lesions at the lower temporal part of the posterior pole could be observed (Fig. 1A + B).
Fig. 1
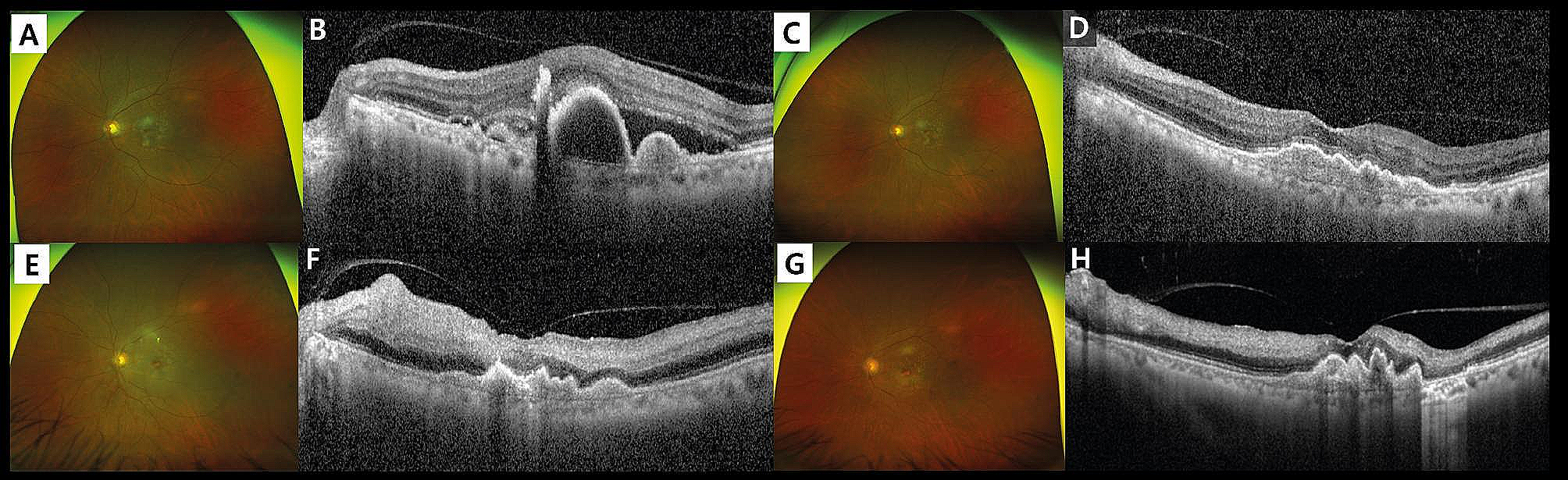
(A) Pseudocolour Ultrawide image of the right eye revealed a bluish grey change at the temporal half of the retina, and an area with rich pigment at the inferotemporal part of the retina; (B) Pseudocolour Ultrawide image of the left eye revealed yellowish white lesions at the lower temporal part of the posterior pole; (C) Color Doppler flow imaging of the right eye presented a proliferative substance on the surface of the retina; (D) Bloodstream map of Color Doppler flow imaging of the right eye, no obvious blood flow signal was observed on the proliferative substance; (E) OCT assessment of the right eye, localized serous detachment of the retina and loss of the outer retinal structure; (F) OCT assessment of the left eye, retinal PED combined with serous detachment of the retina
Colour Doppler flow imaging revealed that the retina under the macular area of the right eye was strongly echoic and slightly elevated, and there was a proliferative substance on the surface of the retina (Fig. 1C + D).
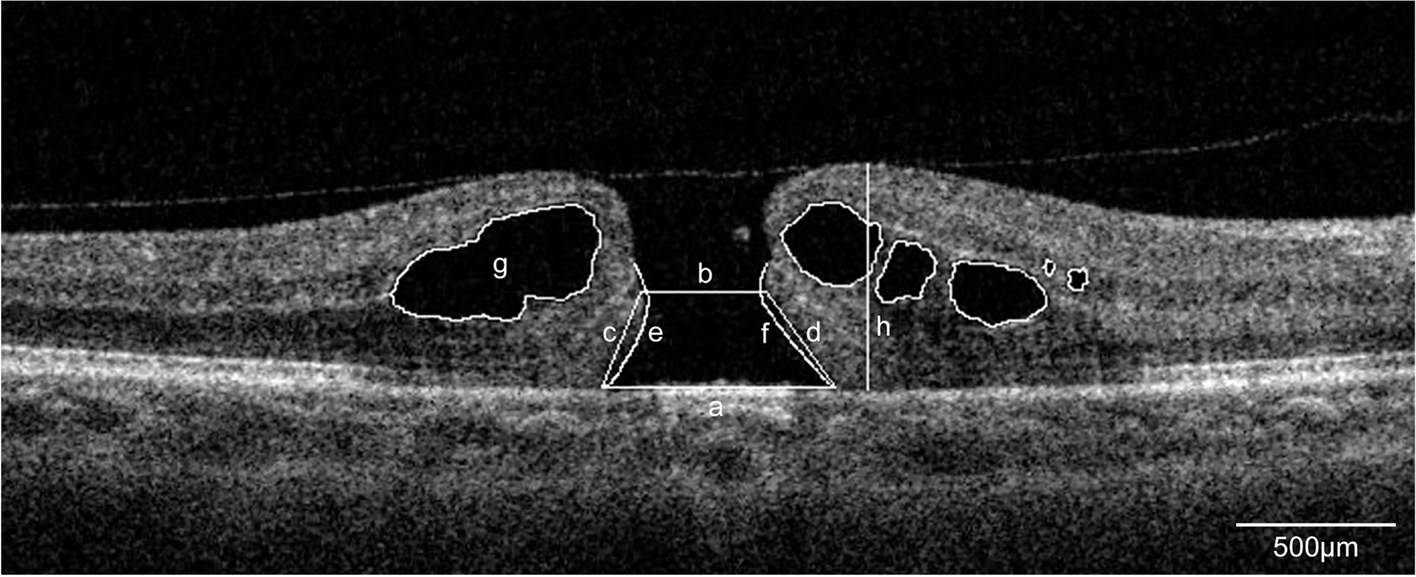
OCT assessment revealed cystic macular edema, localized serous detachment of the retina and loss of the outer retinal structure in the right eye, as well as retinal PED combined with serous detachment of the retina in the left eye (Fig. 1E + F).
FFA of the right eye revealed large window defects in the temporal half of the retina, with a lower-reflectivity irregular edge between the temporal and the nasal retina, and a blocked fluorescence at the inferotemporal part of the retina. ICGA of the right eye showed linear irregular hypofluorescent edges between the temporal half and nasal half of the retina, and a blocked fluorescence at the inferotemporal part of the retina (Fig. 2). Moreover, FFA of the left eye revealed fluorescein leakage in the macular area and the temporal area below the macular area, and ICGA of the left eye demonstrated hyperfluorescence with fluorescein leakage in the temporal area below the macular area (Fig. 3).
Fig. 2
(A) Superior and temporal FFA montage of the right eye, (B) Inferior and posterior FFA montage of the right eye. A&B revealed large window defects in the temporal half of the retina, with a lower-reflectivity irregular edge between the temporal and the nasal retina, and a blocked fluorescence at the inferotemporal part of the retina; (C) Superior and temporal ICGA montage of the right eye, (D) Inferior and posterior ICGA montage of the right eye. C&D showed linear irregular hypofluorescent edges between the temporal half and nasal half of the retina, and a blocked fluorescence at the inferotemporal part of the retina
Fig. 3
(A&B) Early-phase FFA and late-phase FFA of the left eye revealed fluorescein leakage in the macular area and the temporal area below the macular area; (C&D) Early-phase ICGA and late-phase ICGA of the left eye demonstrated hyperfluorescence with fluorescein leakage in the temporal area below the macular area
According to the above examination results, the diagnosis for the left eye was polypoidal choroidal vasculopathy and exudative age-related macular degeneration, while the diagnosis for the right eye was retinal pigment epithelium tears of unclear aetiology.
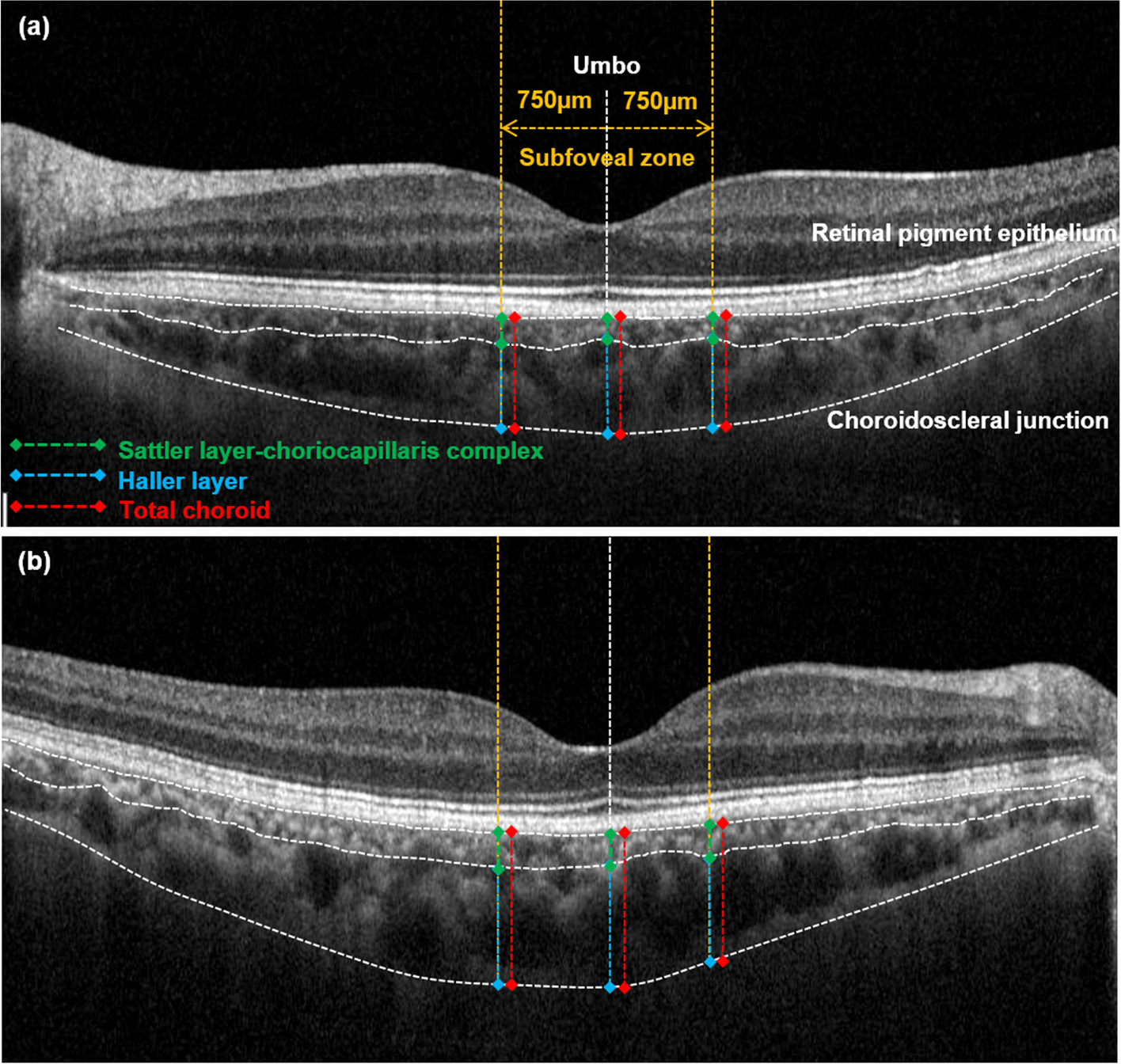
During the FFA and ICGA examinations, additional OCT assessments were performed on both eyes (Fig. 4), which confirmed the above diagnosis.
Fig. 4
(A) OCT assessment of the right eye, the absence of RPE in the temporal area and rolled RPE tissue at the boarder between temporal and nasal retina were observed; (B) OCT assessment of the left eye, PED and retinal neuroepithelial detachment were observed, besides, small finger-like ridges could be seen below the temporal macula
留言 (0)