
記住我


Bone defects of the lower extremities are among the most challenging pathologies to treat in orthopaedic surgery and represent a significant burden of disease for patients and the health care system.1–4 There is a plethora of underlying causes of bone defects including primary bone loss following trauma and secondary bone loss following debridement after trauma or infection, nonunion, or oncologic resection.1,3,4 The aim of bone defect treatment was to achieve consolidation and preserve or restore alignment to allow for weight-bearing in a timely manner. Besides eradication of any associated bone infection,5 treatment options include primary shortening of the bone,6,7 autologous spongiosa,8,9 induced membrane procedure (Masquelet technique),2,10–12 vascularized autograft of the fibula,6,13,14 the use of bone graft substitutes,15,16 and bone transport.17–19 For large defects, osteodistraction is effective but has limitations.17–20
Osteodistraction using external fixation was popularized by Ilizarov in the 1950s.21,22 Good bony healing rates of more than 90% have been described in large bone defects of up to 23 cm.20,23,24 Nevertheless, complications such as pin tract infections, arthrofibrosis, nonunion, and fractures are common, and patients need to tolerate external fixation for 1.74 months per defect centimeter.20
Recently, Barinaga et al and Olesen introduced the plate-assisted bone segment transport “PABST.”17–19 This technique involves osteodistraction using an intramedullary magnetic nail and an internal plate to span the defect during distraction, therefore enabling deformity correction, preservation of length during transport, and quicker weight-bearing without the problems associated with external fixation.17–19,25 Promising results have been demonstrated for PABST with bony healing in femoral bone defects of mean of 9.3 cm at 6.6 months and bony healing in tibial bone defects of mean of 8.9 cm at 10.5 months.19
The purposes of this study were to assess clinical and radiographic outcomes as well as complications following PABST in large bone defects of the lower extremities. The hypothesis was that PABST would show high bony healing rates, satisfactory patient-related outcomes, and acceptable rates of complications and revisions.
MATERIALS AND METHODS Study PopulationThis retrospective, single-center study of prospectively collected data was approved by the local ethics committee. No funding was received. Patients were included if they underwent a PABST procedure from 2018 until 2022 for the tibia or femur and were at least 1 year out from surgery.
Surgical TechniqueAt the authors' institution, indications for the PABST procedure involve bone defects of more than 3 cm of the femur or tibia, most of which are the result of septic or aseptic nonunions following fracture (Figs. 1A, 2A). Rarely, the PABST procedure is performed in tumors.
 FIGURE 1.:
FIGURE 1.: Radiographic images during the PABST procedure of the tibia. A, A 20-year-old man with nonunion following multiple revisions after a pathologic fracture of the lower leg associated with a juvenile bone cyst 6 years ago. B, PABST procedure after resection of the nonunion. C, Before (left image) and after (right image) docking site procedure with autologous bone graft. D, Radiographic follow-up 1 year after PABST procedure demonstrating complete consolidation.
 FIGURE 2.:
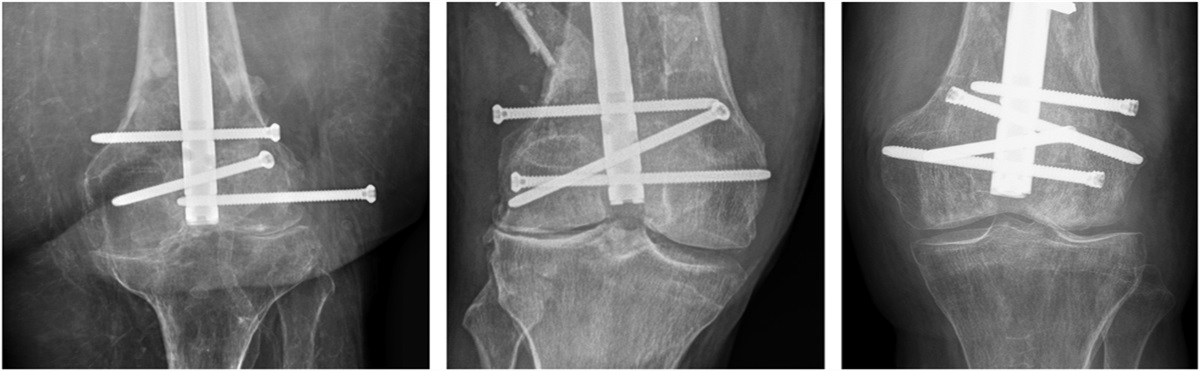
FIGURE 2.: Radiographic images during the PABST procedure of the femur. A, A 53-year-old man following debridement and placement of an antibiotic spacer for septic nonunion. The patient had multiple operative revisions after having sustained a closed comminuted femoral fracture as a result of a motorcycle accident. B, Immediate postoperative radiograph following PABST. C, Radiographs demonstrating completed segment transport. D, Radiographs at 20 months postoperatively following removal of Precice nail, reosteosynthesis, and docking site procedure demonstrating complete consolidation of the docking site and transport callus.
Since sterility is the prerequisite for a successful PABST procedure, all cases (septic and aseptic) were performed in 2 stages. The first stage involves thorough debridement of bone and soft tissues with microbiological samples and implantation of an intramedullary antibiotic (gentamycin and vancomycin) polymethylmethacrylate spacer. An external fixator was not used. Following this first step, intravenous antibiotics are administered until negative microbiology results from intraoperative samples are available. If samples are positive, antibiotics will be continued until the second stage.
For the treatment of osteomyelitis and to optimize timing for a vascularized membrane, the second stage is performed at 6 weeks postoperatively. The antibiotic spacer is removed leaving the surrounding vascularized membrane (Masquelet membrane) intact, soft tissues and bones are again debrided, and microbiological samples are acquired.
A magnetic intramedullary transport nail (Precice, NuVasive, SanDiego) is then implanted. Depending on the location of the bone defect, antegrade (in distal defects) or retrograde (in proximal defects) transport can be performed. If retrograde transport is necessary, the nail is distracted before implantation and subsequently “pulls” the segment during transport. If antegrade transport is possible, the nail is implanted in its retracted/native state thereby allowing for “pushing” of the segment during transport. The nail is then secured by multiple proximal interlocking bolts and usually 1 distal interlocking bolt in the anticipated transport segment.
A metaphyseal/diaphyseal corticotomy is then performed while taking care to avoid excessive heat development. For this reason, oscillating saw blades are not recommended. In the authors' practice, multiple 3.5-mm drill holes are drilled and the corticotomy is finished with an osteotome. Alternatively, a Gigli saw may be used.
Then, plate osteosynthesis is performed by bridging the transport fragment. Stable implants such as large fragment plates are recommended. The plate is fixed using at least 3 bicortical locking screws in each fragment in the tibia and 4 in the femur. Next to the benefit of construct stability, the plate also allows for three-dimensional correction of deformities.
The nail is then lengthened for a few millimeters under fluoroscopic control. This is done to ensure that the nail is adequately working, and the corticotomy is complete. Finally, a nonresorbable suture is placed into the skin just above the nails' magnet so that the patient can later find the correct location for the external controller to allow for daily lengthening.
Antibiotic ManagementPatients were treated with broad spectrum antibiotics intravenously as recommended in currently available guidelines.26 After empirical antibiotic treatment, which has been shown to cover about 95% of causal germs,27 specific antibiotic treatment was continued for 6 weeks based on the final microbiological results. Treatment with biofilm-active antibiotics was preferred whenever possible depending on the culture results.
Postoperative RehabilitationBone segment transport using the magnetic nail is started on postoperative day 7. The nail is usually lengthened 3 times daily using 0.33-mm (0.99 mm/d) steps in the femur and 0.25-mm (0.75 mm/d) steps in the tibia. Seven days after initiation of the transport, plain radiographs are performed to document the transport (Figs. 1B, 2B). Patients are then seen every 2 weeks until transport is complete (Fig. 2C). Weight-bearing during transport is prohibited and is initiated with 20 kg following docking of the nail. Active and passive range of motion exercises of all adjacent joints are started immediately following surgery, once soft tissue swelling subsided.
Re-Charge ProcedureThe maximum stroke of the nail is 8 cm. Therefore, the nail must be retracted (antegrade transport) or distracted (retrograde transport) if transport of more than 8 cm is needed. This can be performed by means of an operation (re-charge) in which the interlocking bolt in the transport segment is removed, the nail is retracted (or distracted), and the bolt in the transport segment is placed again.
Docking Site ProcedureIn the authors' experience, the regenerate bone is generally healing well and reliable. The so-called docking site, which comprises the 2 bone ends of the former defect, is sometimes problematic since consolidation can be prolonged. For this reason, “docking site procedure” is performed after transport in which the bone is debrided and autologous bone graft (lilac crest or “reamer aspirator irrigator”) is placed (Fig. 1C). In some cases, the transport fragment is fixed to the main fragment by using an additional plate.
Data AcquisitionThe electronic medical record database was queried for demographic data such as age, sex, comorbidities, body mass index (BMI), initial fracture type and treatment, microbiological results, last used antibiotics, time from trauma to PABST, time from PABST to re-charge, to the docking site procedure, to the start of weight-bearing, and to full weight-bearing.
Clinical Evaluation and Patient-Reported Outcome MeasuresAll patients who received the PABST procedure (are) were examined in the outpatient department. During transport, patients were seen biweekly for clinical and radiographic follow-up. Once the docking site procedure was concluded, patients were examined every 6 weeks until consolidation is achieved. At minimum 1-year follow-up, patients were contacted to assess pain using the numeric rating scale (NRS) and the lower extremity function scale (LEFS).28,29
Radiographic EvaluationPreoperative radiographs were assessed for bone defect size on anteroposterior radiographs and “radiographic apparent bone gap” (RABG), according to Haines et al,30 in which bone loss is measured on all 4 cortices on standard anteroposterior and lateral radiographs. Standard postoperative radiographs were obtained at day 2, day 14, and every other week until completion of transport and until consolidation or change of treatment strategy (Fig. 1D). Postoperative radiographs were assessed for RABG and consolidation of both the regenerate and the docking site. Bone defects were considered as consolidated if they demonstrated consolidation in at least 3 of 4 cortices (Fig. 2D). If consolidation was difficult to assess, computed tomography was performed. The time from PABST to regenerate consolidation and docking site consolidation were assessed, and consolidation index (months per cm) was calculated.
Statistical AnalysisNormality of data was assessed using the Shapiro–Wilk test. Normally distributed, continuous data were reported as mean with 95% confidence interval (95% CI) if normally distributed and as median with interquartile range (IQR) if skewed. Categorical data were presented as numbers and percentages. Two-tailed P values were calculated and considered significant if P < 0.05. All statistical analysis was performed using Prism software (GraphPad, version 9.5.1, San Diego, CA).
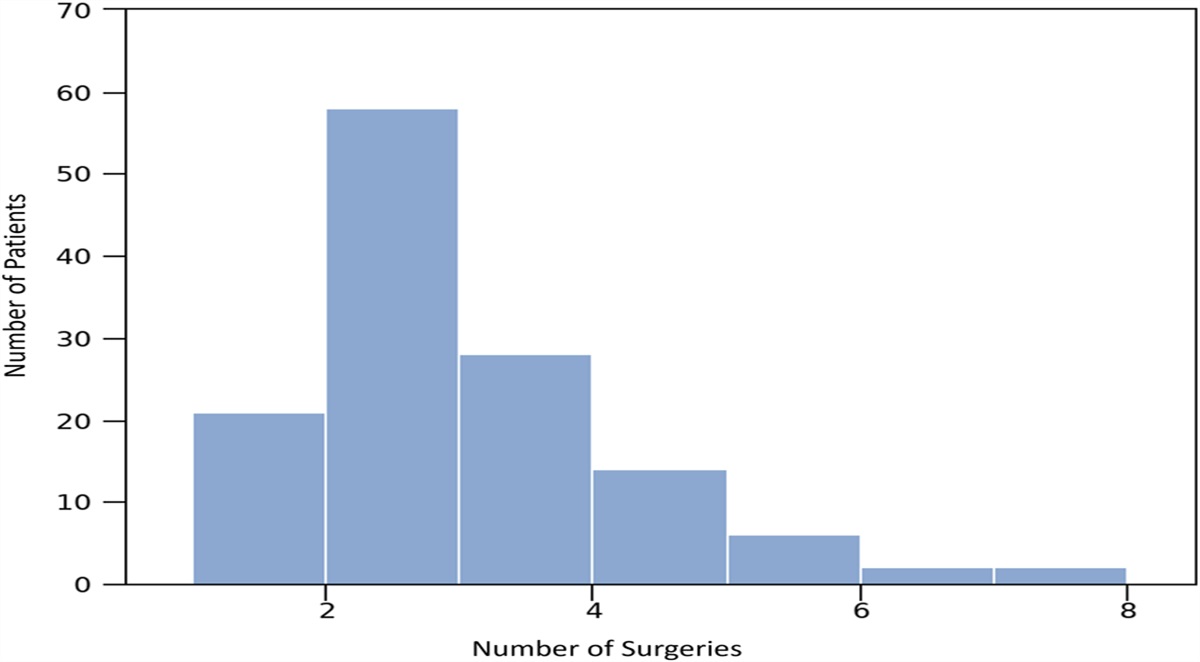
RESULTS Study PopulationA total of 15 patients [13 (87%) male, 2 (13%) female] with a mean age of 51 years (range, 20–75) underwent the PABST procedure. Minimum 1-year clinical and radiographic follow-up data were available for all 15 patients at a mean of 29.1 months (range, 12–52). Indications for the PABST procedure were septic [11 (73%) and aseptic 3 (20%)] nonunions from fractures, as well as sequelae of a juvenile bone cyst [1 (7%)], all resulting in bone defects greater than 3 cm. A third of all patients [5 (33%)] had an open fracture initially (1 type II, 4 type III). Patients underwent at a median of 7 (IQR: 2–15) surgical procedures for limb salvage before PABST procedure. The most common comorbidity was high blood pressure with 7 patients (47%) being affected, followed by obesity (BMI > 30) and renal insufficiency [both 5 patients (33%)]. A total of 2 patients had an ASA score of 1, 11 patients (73%) had an ASA score of 2, and 2 patients had an ASA score of 3. Demographic data of the patient cohort are summarized in Table 1.
TABLE 1. - Demographic Data of the Patient Cohort Demographic Variables Tibia/Femur, n (%) 8 (53)/7 (47) Right/Left, n (%) 6 (40)/9 (60) BMI (kg/m2), mean (95% CI) 28 (25–31) Prior surgeries >5, n (%) 13 (87) Positive microbiological sample*, n (%) 11 (73) Preoperative bone defect size (mm), median (IQR) 60 (40–125) Preoperative RABG (mm), mean (95% CI) 57 (40–73)*Refers to the last surgery before PABST.
Patients underwent the PABST procedure at a median of 14 months (IQR: 6–168) following their initial trauma. Depending on patient factors such as nicotine status transport rate ranged from 0.5 mm to 1.0 mm per day split in 2–3 distraction sessions. In 4 of the 15 patients, the osteotomy was done in the metaphysis. Owing to the size and location of the nonunions and hardware traffic, the osteotomy was performed between the metaphysis and diaphysis in 4 patients and the diaphysis in 7 patients. The transport was performed antegrade in 11 patients (73%) and retrograde in 4 patients (27%). A total of 7 patients (47%) underwent re-charge of the nail, and all patients (100%) underwent a docking site procedure. The site of the autologous bone grafting was selected depending on the patients' previous surgeries. Reamer aspirator irrigator was used in 7 patients. Autologous bone graft from the iliac crest was used in the remaining patients, in some cases a combination with allogeneic bone grafting. In addition to the autologous bone grafting described above, additive fixation with screws was performed in 5 cases through the initial plate. In cases requiring correction of alignment, the docking site procedure was combined with additive plate osteosynthesis. Data relevant to the PABST procedure are presented in Table 2.
TABLE 2. - Variables Relevant to the PABST Procedure Variables Relevant to the PABST Procedure Injury to PABST (mo), median (IQR) 14 (6–168) Rate of transport (mm/d), median (IQR) 0.75 (0.5–1.0) Re-charge procedure performed, n (%) 7 (47) PABST to re-charge (mo), mean (95% CI) 3.3 (2.4–4.1) Docking site procedure performed, n (%) 15 (100) PABST to docking site (mo), mean (95% CI) 5.5 (3.8–7.3) Duration of transport (mo), mean (95% CI) 3.5 (2.5–4.5)All patients achieved full weight-bearing at a median of 8.7 (IQR: 6.5–10.3) months. A total of 14 patients (93%) demonstrated consolidated transport callus at a mean of 7.3 (95% CI, 6–8.5) months following PABST, and 9 patients (60%) demonstrated complete consolidation of both the docking site and the transport callus at a mean of 11.5 (95% CI, 7.3–15.3) months. There was 1 patient who had a consolidated docking site, but transport callus had not yet consolidated. Malalignment was observed in 9 of the 15 patients during bone transport. Implant failure was observed in 2 of these cases. In 5 patients, the alignment was corrected by changing the plate osteosynthesis. In 2 cases, the malalignment was corrected using screws through the initial plate. In 2 cases, the malalignment was tolerated.
Of the 6 patients (40%) with radiographic nonunion of the docking site, 2 patients underwent distal femoral replacement (MUTARS, Fa. Implantcast, Germany). However, both patients initially underwent the PABST procedure for bone defects caused by metaphyseal femoral fractures, with the newly generated bone stock now allowing superior stem placement. Four of the 6 patients only had mild symptoms (NRS: 0–3). Clinical and radiographic data are presented in Table 3.
TABLE 3. - Clinical and Radiographic Variables After PABST Clinical and Radiographic Variables after PABST Duration of no weight-bearing (mo), mean (95% CI) 5.7 (4.3–7) PABST to full weight-bearing (mo), median (IQR) 8.7 (6.5–10.3) PABST to transport callus consolidation (mo), mean (95% CI) 7.3 (6–8.5) PABST to consolidation of docking site (mo), mean (95% CI) 11.5 (7.3–15.3) Consolidation index (months/cm), mean (95% CI) 1.9 (1.3–2.5) RABG at 1 y postoperative (mm), median (IQR) 0.1 (0–0.8) LEFS, mean (95% CI) 42 (34–50) NRS, mean (95% CI) 3 (2–4)Subgroup analyses are demonstrated for PABST procedures performed for tibial versus femoral bone defects and obese (BMI ≥ 30) versus normal weight (BMI < 30) patients (see Table, Supplemental Digital Content 1, https://links.lww.com/JOT/C207).
ComplicationsThere were no cases of reinfection during the PABST procedure. One patient had a premature consolidation during transport and required recorticotomy, and 1 patient sustained a fracture of the ilium following bone graft harvesting for the docking site procedure. At the end of bone transport, broken screws in combination with malalignment were observed in 2 of the 15 patients. In these cases, the alignment was corrected with reosteosynthesis by plate as part of the docking site procedure.
DISCUSSIONThe most important findings of this study were that 93% of all bone defects up to 125 mm in length could be closed by means of callus distraction. Nevertheless, a docking site procedure was performed in all patients. No reinfections or wound healing disorders were observed 1 year postoperatively. Another important finding was that a BMI of 30 or higher was associated with significantly worse outcomes.
The size of bone defects for which the PABST procedure is optimal remains undefined. As described above, defects of up to 125 mm were successfully treated, although with the option of re-charging the nail, the authors believe that larger defects are amenable to this procedure as well. According to our own experience, bone defects smaller than 3 cm may consolidate sufficiently with both autologous and allogenic bone grafting or bone graft substitutes. Consequently, the PABST procedure is performed for bone defects larger than 3 cm at our institution.
The consolidation index of the presented patient cohort averaged 1.9 (months/cm), which was higher when compared with bone transport in previous studies.19,31,32 A consolidation index of 1.8/1.9 (months/cm) was previously described for external fixator lengthening.33,34 However, 93% of the presented cases demonstrated bony consolidation at the area of callus distraction with an average RABG of 0.1 mm at the docking site. Consequently, radical debridement can be performed before the PABST procedure without concern of increasing the bone defect size. Radical debridement is paramount to prevent reinfection rates and may be the explanation that we did not encounter any at 1 year postoperatively in this challenging patient cohort. To ensure successful bone transport, it is necessary to perform continuous radiographic monitoring to prevent excessive or retarded transport with the consequence of instability or premature bony consolidation as experienced in 1 case. As a result, the authors recommend weekly radiographic monitoring following the initiation of the PABST procedure.
A docking site procedure was used in all patients ensuing bone transport. Thus far, there is limited experience with failure of bony consolidation of the docking site after the PABST procedure. Olesen et al19 found that failure of bony consolidation of the docking site in the tibia is an issue; however, precise data regarding the number of patients requiring a docking site procedure were not demonstrated. In this study, bone healing at the docking site was not achieved in 40% of patients at 1-year follow-up. Of note, one-third of these cases had metaphyseal bone defects, and the PABST procedure was performed primarily to achieve adequate bone stock in preparation of total knee arthroplasty. On average, the PABST procedure was performed 14 months after initial trauma and multiple surgeries. It remains to be evaluated whether earlier radical debridement and indication for bone transport could also improve bone healing at the docking site. Docking site procedures were performed at a median of 2 months after the bone transport was completed. We hypothesize that a reduction in treatment time, increased patient comfort, and potentially higher rates of healing may be achieved when docking site procedures are performed earlier. However, incomplete bony consolidation at the docking site did not seem to preclude patients from full weight-bearing or did have any effect on pain or functional outcomes. Subsequently, a critical discussion is warranted regarding the importance of bony consolidation at the docking site for the functional outcome and necessity for patients to undergo an additional procedure.
Furthermore, the validity of the LEFS in patients who underwent the PABST procedure is questionable. On average, the patients in this study had a LEFS of 50. According to the literature, a score of 52 in a 70-year-old patient is a functionally good outcome.35,36 Among other things, the LEFS asks for skills, such as running, jumping, and quick changes of direction. These tasks, however, are not realistic in a patient 1 year after PABST procedure. This is especially the case in patients with metaphyseal bone defects and recent arthroplasty. The demonstrated values in LEFS and a mean NRS of 3 are consequently to be classified as good functional results.
A BMI of 30 or greater seems to be a determining factor for outcomes. Preoperative RABG was significantly higher in patients with a BMI ≥ 30 compared with patients with a BMI < 30. This may be explained by higher forces and greater comminution following the initial trauma. Furthermore, in patients with a BMI ≥ 30, the time to callus consolidation and accordingly to full weight-bearing was significantly increased, which may be a consequence of the higher weight and larger initial RABG.
Interestingly, callus consolidation was significantly prolonged in femoral bone defects when compared with tibial defects. In addition, significantly decreased bony consolidation of the docking site was observed in bone defects of the femur. This is surprising due to better soft tissue coverage at the femur and often postulated higher healing potential. However, it is important to note that patients with bone defects of the femur were significantly older in this study. In addition, patients with femoral defects tended to have a higher BMI.
The number of cases in this investigation is limited. Furthermore, the patient population is very heterogeneous regarding localization of the defect (metaphyseal vs. diaphyseal) and defect size. Owing to the long transport and overall treatment time, the follow-up period of 1 year seems to be relatively short; however, most patients achieved consolidation of the transport callus. Finally, some of the patients did just receive arthroplasty after metaphyseal transport around 1 year postoperatively, which obviously has a negative effect on the functional scores.
CONCLUSIONSPABST demonstrated high consolidation rates of transport callus with few complications. Although full weight-bearing was achieved in all patients, complete consolidation of the docking site was only present in 60% of cases.
REFERENCES 1. Nauth A, McKee MD, Einhorn TA, et al. Managing bone defects. J Orthop Trauma. 2011;25:462–466. 2. Nauth A, Schemitsch E, Norris B, et al. Critical-size bone defects: is there a consensus for diagnosis and treatment? J Orthop Trauma. 2018;32(suppl 1):S7–S11. 3. Feltri P, Solaro L, Di Martino A, et al. Union, complication, reintervention and failure rates of surgical techniques for large diaphyseal defects: a systematic review and meta-analysis. Sci Rep. 2022;12:9098. 4. Schemitsch EH. Size matters: defining critical in bone defect size!. J Orthop Trauma. 2017;31(suppl 5):S20–S2S22. 5. Metsemakers WJ, Morgenstern M, Senneville E, et al. General treatment principles for fracture-related infection: recommendations from an international expert group. Arch Orthop Trauma Surg. 2020;140:1013–1027. 6. Ferreira N, Tanwar YS. Systematic approach to the management of post-traumatic segmental diaphyseal long bone defects: treatment algorithm and comprehensive classification system. Strateg Trauma Limb Reconstr. 2020;15:106–11166. 7. Barker KL, Simpson AH. Recovery of function after closed femoral shortening. J Bone Joint Surg Br. 2004;86:1182–1186. 8. Sen MK, Miclau T. Autologous iliac crest bone graft: should it still be the gold standard for treating nonunions? Injury. 2007;38(suppl 1):S75–S80. 9. Keating JF, Simpson AH, Robinson CM. The management of fractures with bone loss. J Bone Joint Surg Br. 2005;87:142–150. 10. Masquelet AC, Fitoussi F, Begue T, et al. Reconstruction of the long bones by the induced membrane and spongy autograft [in French]. Ann Chir Plast Esthet. 2000;45:346–353. 11. Fung B, Hoit G, Schemitsch E, et al. The induced membrane technique for the management of long bone defects. Bone Joint J. 2020;102-B:1723–1734. 12. Mauffrey C, Hake ME, Chadayammuri V, et al. Reconstruction of long bone infections using the induced membrane technique: tips and tricks. J Orthop Trauma. 2016;30:e188–e193. 13. Tsang STJ, Ferreira N, Simpson A. The reconstruction of critical bone loss: the holy grail of orthopaedics. Bone Joint Res. 2022;11:409–412. 14. Feltri P, Solaro L, Errani C, et al. Vascularized fibular grafts for the treatment of long bone defects: pros and cons. A systematic review and meta-analysis. Arch Orthop Trauma Surg. 2023;143:29–48. 15. Ferguson J, Diefenbeck M, McNally M. Ceramic biocomposites as biodegradable antibiotic carriers in the treatment of bone infections. J Bone Joint Infect. 2017;2:38–51. 16. Freischmidt H, Armbruster J, Bonner E, et al. Systemic administration of PTH supports vascularization in segmental bone defects filled with ceramic-based bone graft substitute. Cells. 2021;10:2058. 17. Barinaga G, Beason AM, Gardner MP. Novel surgical approach to segmental bone transport using a magnetic intramedullary limb lengthening system. J Am Acad Orthop Surg. 2018;26:e477–e482. 18. Kähler Olesen U. Plate-assisted segmental bone transport with a lengthening nail and a plate: a new technique for treatment of tibial and femoral bone defects [in German]. Unfallchirurg. 2018;121:874–883. 19. Olesen UK, Nygaard T, Prince DE, et al. Plate-assisted bone segment transport with motorized lengthening nails and locking plates: a technique to treat femoral and tibial bone defects. J Am Acad Orthop Surg Glob Res Rev. 2019;3:e064. 20. Aktuglu K, Erol K, Vahabi A. Ilizarov bone transport and treatment of critical-sized tibial bone defects: a narrative review. J Orthop Traumatol. 2019;20:22. 21. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part I. The influence of stability of fixation and soft-tissue preservation. Clin Orthop Relat Res. 1989;238:249–281. 22. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989;239:263–285. 23. Papakostidis C, Bhandari M, Giannoudis PV. Distraction osteogenesis in the treatment of long bone defects of the lower limbs: effectiveness, complications and clinical results; a systematic review and meta-analysis. Bone Joint J. 2013;95-b:1673–1680. 24. Yin P, Ji Q, Li T, et al. A systematic review and meta-analysis of Ilizarov methods in the treatment of infected nonunion of tibia and femur. PLoS One. 2015;10:e0141973. 25. Barakat AH, Sayani J, O'Dowd-Booth C, et al. Lengthening nails for distraction osteogenesis: a review of current practice and presentation of extended indications. Strateg Trauma Limb Reconstr. 2020;15:54–61. 26. Tucci G, Romanini E, Zanoli G, et al. Prevention of surgical site infections in orthopaedic surgery: a synthesis of current recommendations. Eur Rev Med Pharmacol Sci. 2019;23:224–239. 27. Baertl S, Walter N, Engelstaedter U, et al. What is the most effective empirical antibiotic treatment for early, delayed, and late fracture-related infections? Antibiot (Basel). 2022;11:287. 28. Naal FD, Impellizzeri FM, Torka S, et al. The german lower extremity functional scale (LEFS) is reliable, valid and responsive in patients undergoing hip or knee replacement. Qual Life Res. 2015;24:405–410. 29. Binkley JM, Stratford PW, Lott SA, et al. The lower extremity functional scale (LEFS): scale development, measurement properties, and clinical application. North American orthopaedic rehabilitation research network. Phys Ther. 1999;79:371–383. 30. Haines NM, Lack WD, Seymour RB, et al. Defining the lower limit of a “critical bone defect” in open diaphyseal tibial fractures. J Orthop Trauma. 2016;30:e158–e163. 31. Holm I, Nordsletten L, Steen H, et al. Muscle function after mid-shaft femoral shortening. A prospective study with a two-year follow-up. J Bone Joint Surg Br. 1994;76:143–146. 32. McNally M, Ferguson J, Kugan R, et al. Ilizarov treatment protocols in the management of infected nonunion of the tibia. J Orthop Trauma. 2017;31(suppl 5):S47–S54. 33. Horn J, Grimsrud Ø, Dagsgard AH, et al. Femoral lengthening with a motorized intramedullary nail. Acta Orthop. 2015;86:248–256. 34. Rozbruch SR, Kleinman D, Fragomen AT, et al. Limb lengthening and then insertion of an intramedullary nail: a case-matched comparison. Clin Orthop Relat Res. 2008;466:2923–2932. 35. Stasi S, Papathanasiou G, Korres N, et al. Validation of the lower extremity functional scale in community-dwelling elderly people (LEFS-Greek); determination of functional status cut-off points using TUG test. Eur Geriatr Med. 2013;4:237–241. 36. Davenport SJ, de Morton NA. Clinimetric properties of the de Morton Mobility Index in healthy, community-dwelling older adults. Arch Phys Med Rehabil. 2011;92:51–58.
留言 (0)