
記住我


A 68-year-old woman was admitted to the Department of Otorhinolaryngology, General Hospital of Vienna, Medical University of Vienna, with severe right-sided pain exacerbations to further evaluate a right-sided naso—/ oropharyngeal mass. Due to an oncological history of head and neck tumors, there was a strong suspicion of a new or recurring malignant disease.
Medical historyRegarding her oncological history, in 2011 she was diagnosed with a right-sided sphenoid meningioma and a left-sided neck metastasis of a CUP in 2012. The meningioma (08 / 2011) initially had a volume of 23.6 cm3 and infiltrated the cavernous sinus also causing a right-sided abducens palsy. It was treated with gamma-knife surgery with14Gy at the border area and 35 Gy in the center with a 40% isodose line with eleven isocenters (collimators; 4 mm, n = 1; 8 mm, n = 3; 14 mm, n = 1; 18 mm, n = 6).
In May 2012, the patient noticed a suspicious neck lump in level V and therefore underwent a diagnostic lymph node sampling. This turned out to be a lymph node metastasis of an intermediate differentiated squamous cell carcinoma without a clinically apparent primary tumor (CUP). Therefore, she underwent a thorough CUP check-up and subsequently therapy consisting of panendoscopy, completion of left-sided neck dissection and adjuvant radiochemotherapy. Due to the reduced general condition, the patient received only two of five scheduled cycles of cisplatin in a reduced concentration of 30 mg/m2 weekly. According to former CUP treatment recommendations, pharynx, larynx and neck levels Ib to V were radiated on both sides with a dosage of 50 Gy, the left level V neck with a boost up to 60 Gy, and the right parapharyngeal space, floor of mouth, soft palate and the junction between oro- and nasopharynx received an additional boost up to 70.4 Gy (2 Gy single dosage). [23, 24]
Signs of ORN were first present in 2016 when the patient presented with maxillary and mandibular ORN.Therefore, she underwent several long-term antibiotic treatments as well as surgical debridements. A partial mandibulectomy was finally performed in 2019, and there have been no apparent signs of ORN since then.
Clinical presentation and treatmentFrom a clinical point of view, the patient now presented with trismus, severe right-sided pain (Numeric Rating Scale / NRS 10/10), a solid lesion in the oropharynx/nasopharynx and complete blockage of the right choana. Due to her former oncological and ORN therapies, she was already entirely dependent on a gastrostomy tube. Further imaging studies were scheduled and sufficient pain management was established. The solid lesion was biopsied transorally and histologically proved to represent inflammatory material without evidence of malignant cells.
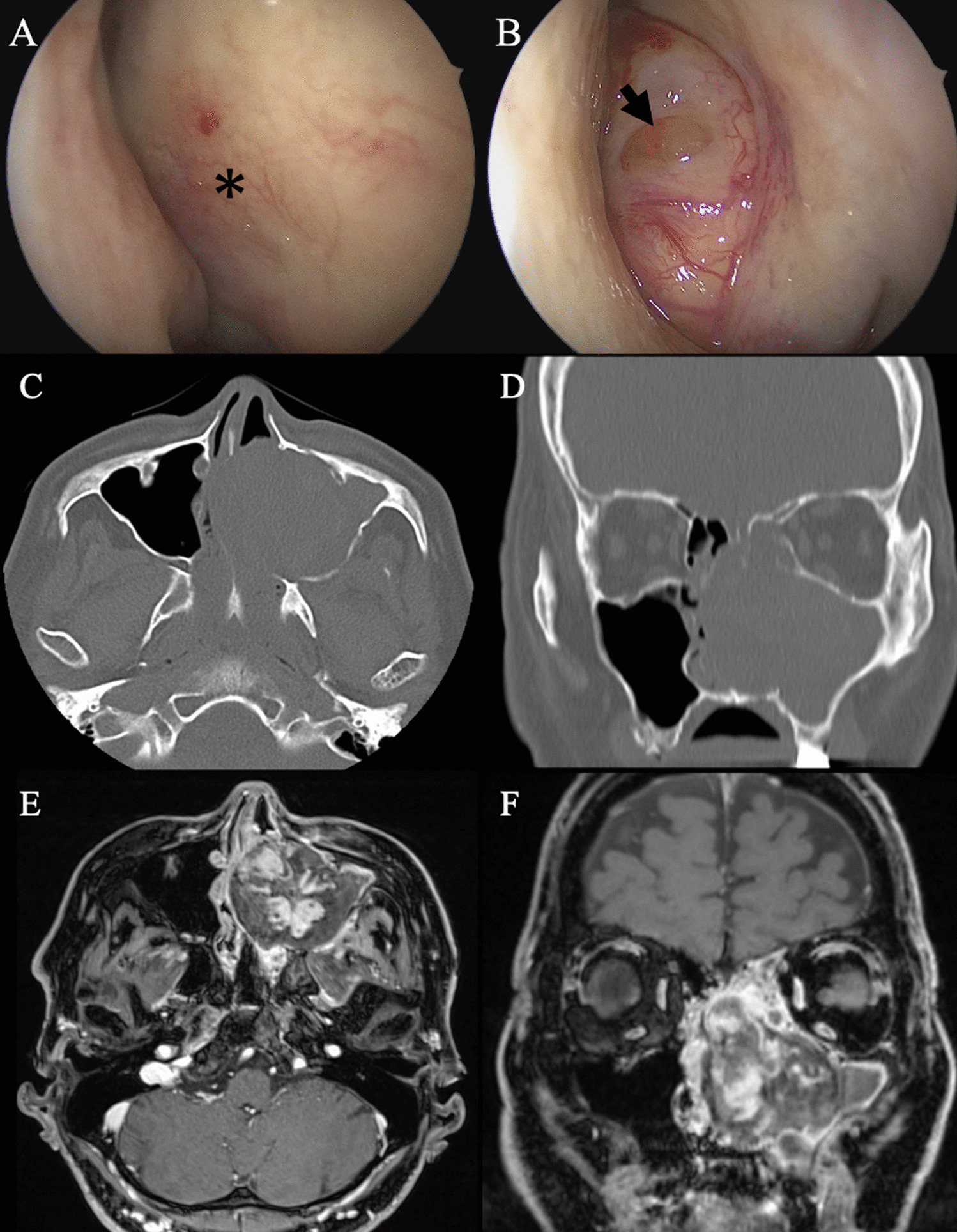
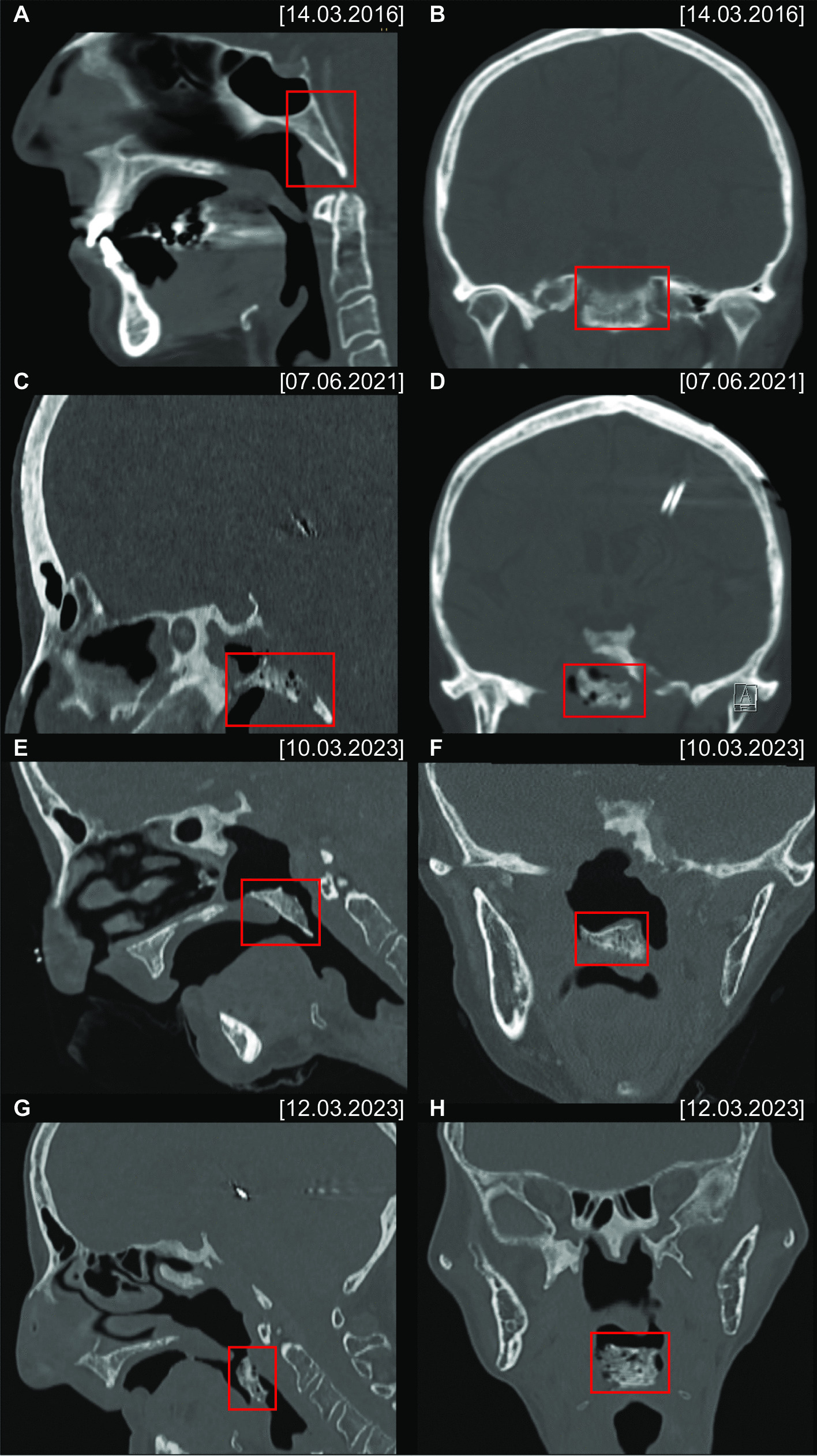
The subsequent head and neck CT scan revealed an advanced ORN of the skull base with subsequent abruption of the ventral part of the clivus with caudal dislocation towards the oropharynx (Figs. 1E, F and A). Soft tissue was present in the former location of the clivus and no pneumocephalus or CSF leakage had developed. Within the next 48 h, a further dislocation of the fractured clival sequestrum occurred, resulting in an almost complete obstruction of the laryngeal inlet with severe dyspnoea (Figs. 1G, H and B).
Fig. 1
CT scans in the bone window (sagittal: A, C, E, G; coronal: B, D, F, H) show severe radio osteonecrosis of the anterior skull base with a chip fracture of the clivus (red rectangle) and the progredient dislocation
After ruling out any possible cervical spine instability, the patient’s airway was secured with an awake tracheostomy and the clival sequestrum was removed transorally (Fig. 2C). The pathohistological workup of the 2.2 × 2.1 × 0.5 cm bone fragment revealed infected osteonecrosis with abundant actinomyces and coccoid bacterial infection. After consultation of an infectious disease specialist, the patient was put on metronidazole and ceftriaxone for only 10 days. Because of a treatment acquired Clostridium difficile colitis, the further planned long-term antibiotic treatment had to be postponed. The patient was finally discharged pain-free (NRS 0–1/10) and decannulated without CSF fistula after a total inpatient stay of 20 days. The interdisciplinary Skull Base Board further recommended a primarily conservative treatment approach with the implementation of HBO therapy.
Fig. 2
VRT-reconstruction of the CT scans (A on March 10th 2023 and B on March 12th 2023) showing that the dislocation of the fractured clivus caused an almost complete obstruction of the laryngeal inlet within 48 h (A + B). The final picture of the dislocated clival sequestrum after successful transoral removal (C)
留言 (0)