Intermittent hypoxia caused by OSA
With the improvement of people’s living standards and changes in lifestyle, the incidence of OSA has increased year by year. Intermittent hypoxia due to OSA can cause a number of pathophysiologic changes [11] such as oxidative stress [12], systemic inflammation [13], and sympathetic system activation [14], which are the pathological basis for the many diseases. Thus, intermittent hypoxia is an important part of disease development and should not be ignored.
Solitary pulmonary nodules and thyroid nodules
Figure 2 shows a positive correlation between OSA and SPN (P < 0.001, OR > 1), indicating that the presence of OSA may lead to an increase in the incidence of SPN. However, there were many confounding factors among them. A prospective cohort study [15] showed that age, smoking history, lung disease history, occupational exposure, and family history of cancer may affect the incidence of pulmonary nodules. Sun Ying [16] found a correlation between age, respiratory system diseases, BMI, and the incidence of pulmonary nodules through a study of 69,957 healthy individuals. Chen Liqun’s research [17] also found that individuals with a history of tumors are more likely to detect pulmonary nodules. Therefore, we excluded some variables related to SPN (age, gender, BMI, smoking history, history of lung disease, history of tumors) and found that the results were still significant (Table 2). Similarly, some studies have confirmed an independent correlation between women, age, BMI, metabolic syndrome, thyrotoxicosis, and TN [18,19,20]. So we found a correlation between OSA and TN after excluding age, gender, BMI, and thyroid disease (Table 3). We speculate that OSA may be one of the reasons for the occurrence of SPN and TN. Because we have not comprehensively excluded all confounding factors and there are limited reports on OSA and two diseases, this is only our speculation and further investigation is expected in the future. This study also conducted a correlation analysis between SPN, TN, and some sleep indicators (AHI, LSpO2, MSpO2, TAT, LAT). We found that patients with SPN or TN have lower nighttime blood oxygen concentration and longer apnea time (Fig. 3). Intermittent hypoxia may be a pathological factor in the process of SPN or TN caused by OSA. This is just speculation, and we hope to have relevant pathological research in the future.
Carotid-artery plaques
The development of OSA is accompanied by a degree of hypoxia, which results in enhanced lipid loading in foam cells and susceptibility of endothelial cells to free radical damage, leading to the formation of atherosclerotic plaques. This study confirms that there is a significant correlation between CAP and OSA, and the incidence of the former increased with the severity of the latter. CVD patients generally exhibit atherosclerosis, which inevitably leads to a high incidence of CAP in this research. However, the result was still statistical after adjusting gender, age, related vascular disease, diabetes, and other factors (Table 1). This agrees with much recent research [21,22,23].
Abnormal metabolism
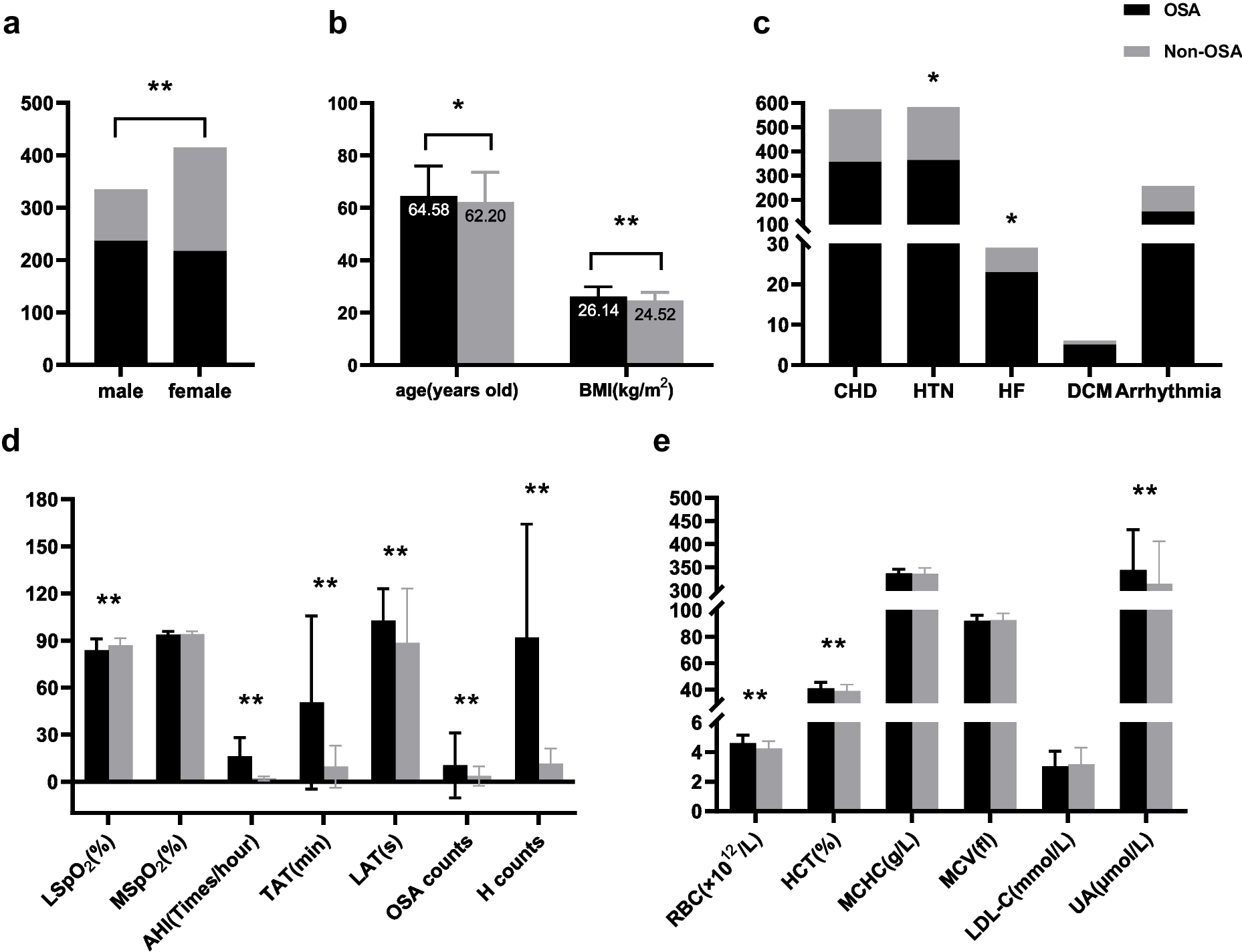
It has been confirmed that OSA can cause abnormal lipid metabolism [24]. On the one hand, recurrent intermittent hypoxia during sleep results in elevated levels of hypoxia-inducible factor-1. Lipolysis of adipose tissue and increased biosynthesis in the liver promote LDL-C secretion [25]. A significant correlation between LDL-C and OSA has been shown in numerous studies. However, this study could not exclude the fact that some patients were required to take lipid-lowering drugs for their condition, which had an impact on the results. On the other hand, hyperlipidemia has been implicated as a mechanism linking OSA and coronary heart disease [26]. OSA-induced dyslipidemia worsens the cardiac coronary conditions in CVD patients.
The data showed significant differences in the RBC, HCT, and UA levels between the two groups, which were related to chronic intermittent hypoxia leading to a compensatory response, suggesting that OSA may cause varying degrees of metabolic syndrome [27]. Furthermore, elevated hematocrit may affect hemorheology and lead to hypercoagulation of blood, exacerbating cardiovascular disease. To sum up, the presence of OSA in patients with CVD can lead to metabolic abnormalities, and OSA should be actively improved to avoid disease progression.
Prevention and treatment of OSA
Upper airway collapse is the main pathologic feature of OSA, while age, gender, obesity, nasopharyngeal diseases, and CS are independent risk factors for OSA [28,29,30,31]. In patients with OSA, the prevalence is significantly higher in males than in females, and the prevalence increases with age. In addition, obese patients with submucosal fat deposits in the oropharynx are prone to apnea. Nasal disorders such as rhinopolypus, turbinate hypertrophy, NSD, and chronic rhinitis result in obstruction of nocturnal nasal breathing, making the pressure in the pharyngeal cavity lower than the atmospheric pressure, and then increased pharyngeal transmural pressure leads to airway closure. When nasal obstruction triggers mouth breathing, it increases the incidence of collapse of the lateral pharyngeal wall and tongue root [32, 33], resulting in apnea and hypoventilation. Furthermore, changes in modern lifestyles have exacerbated the occurrence of CS. OSA occurs when a cervical disc herniation or cervical degeneration causes increased compression of the tissues surrounding the pharyngeal airway space, resulting in pharyngeal stenosis [34]. This is consistent with the anatomical impact of cervical morphologic changes on the pharyngeal airway in patients with CS [35]. So, OSA can be avoided to some extent by weight loss, regular and adequate sleep, and improvement of cervical spine morphology. Patients with nasopharyngeal disorders should be motivated to undergo corrective or surgical procedures that will improve ventilation. Continue positive airway pressure (CPAP) is the first-line treatment for patients with OSA, which improves nocturnal hypoventilation and reduces the risk of CVD and multi-organ damage [36]. In conclusion, intermittent hypoxia is worthy of attention. Improving ventilation and correcting intermittent hypoxia are the main methods for treating OSA. This may improve many diseases caused by OSA.
Limitations
Several limitations of this study should be considered. First, as this is a retrospective study, it is not possible to exclude the influence of some patients taking relevant medications due to their condition on the results of the study. Second, this research was based on patients with CVD, and we hypothesize that OSA can still increase the incidence of SPN, TN, and other diseases in the general population. Therefore, we will conduct a large-scale prospective study in the population in the future to further characterize the correlation between OSA and SPN and TN, as well as the mechanisms, on the basis of excluding relevant risk factors.






留言 (0)