In this study, the impact of grade on staging investigations and treatment of RNETs was explored. Our results suggest that there is minimal role in biochemical staging even though it is ordered excessively by providers irrespective of grade. Staging imaging may be useful in grade ≥ 2 lesions, as these patients had more metastasis at diagnosis, higher recurrence risk, and worse OS. Patients with grade 2 lesions also underwent more anatomic resections, highlighting grade as a potential factor in guiding treatment decision-making. Overall, grade is a valuable marker that should be consistently incorporated into early RNET staging and management guidelines.
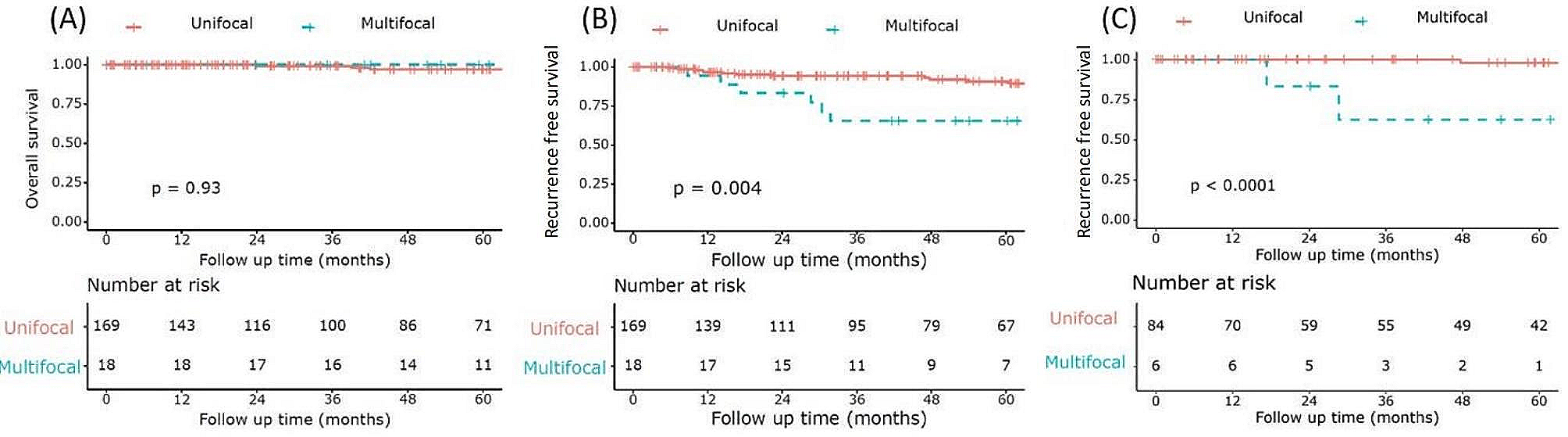
RNETs are often small with low risk features and distant metastases are rare [1] with some studies quoting a rate as low as 4.2% at the time of diagnosis [3]. Our study reported a higher rate of 19%, which is likely influenced by a larger population of grade ≥ 2 disease. When stratified by grade, 1% and 45% of patients with grade 1 and 2 disease, respectively, had distant metastasis at diagnosis which parallels the increasing trend of 2.1% and 31.4% (p < 0.001) reported in literature [22]. The more aggressive tumor biology seen in grade ≥ 2 lesions [22] suggests a need for complete staging and definitive management strategies.
There is variability and lack of clarity in current guidelines for timing, modality and indication of staging for RNETs [5, 6]. NANETS recommend no staging for lesions < 20 mm while ENETS and the National Comprehensive Cancer Network (NCCN) recommend no staging for lesions < 10 mm [5, 6, 23]. In our study, 52% underwent some form of staging even though only 10% of patients had lesions ≥ 10 mm. Apart from urine 5-HIAA and MRI, staging investigations were not associated with grade suggesting a lack of provider understanding of RNET biology. Better adherence to guidelines and incorporation of grade into staging strategies could help stratify resources to improve diagnostic efficacy.
Twenty-four-hour urine 5-HIAA and serum CgA are often performed in conjunction with a diagnosis of a NET. Their role in staging RNETs is controversial and there is limited evidence to support their use. In our study, 27% and 32% of patients underwent urine 5-HIAA and serum CgA staging, respectively, but 97% and 100% of results were negative. Hindgut NETs rarely produce serotonin [24]; therefore, an elevated 24 h urine 5-HIAA test is often non-specific [25] and has no known prognostic value [9]. Serum CgA may have a limited role in predicting extent of disease in small bowel NETs [11]; but its use in diagnosis and prediction of recurrence in RNETs is unclear [10]. False positive results are common, making elevated values, especially those only mildly above the upper limit of normal, difficult to interpret [5, 25]. Our study shows no utility for biochemical staging with urine 5-HIAA or serum CgA for RNETs, regardless, which is concordant with current literature [5, 6, 10, 24, 25].
Imaging plays an important role in staging disease and is necessary to guide subsequent management in many malignancies. CT is the most common imaging modality performed for staging in our study with a 24% rate of disease detection. Liver metastases were identified in 54% of positive CT scans with the majority (57%) in patients with grade 2 or 3 disease while 43% of positive scans did not have grade documented. Of patients with grade 1 disease confirmed from endoscopy who also underwent CT staging, none were found to have liver metastases. Only one patient with grade 1 disease had peritoneal metastasis at diagnosis, but this was identified during surgery and not on the CT scan; therefore, staging CT in this patient would not have been useful. CT is recommended as an initial staging modality by ENETS [6] and other studies [18] because of its accessibility, low cost, and reasonable sensitivity for detection of liver metastases (43–80%) [26, 27]. Based on our findings, we recommend that all patients with grade 2 or 3 RNETs undergo staging with CT of the abdomen and pelvis. Lung metastases in GEP-NETs are uncommon [28, 29]; therefore, staging CT chests are not recommended.
Other imaging modalities for staging were also explored in our study. Amongst 13 patients who received a pelvic MRI, local or regional disease was detected in 62%. As lesions < 10 mm and > 10 mm have a 25% [30] and 61% [31] incidence of regional nodal metastases, respectively, pelvic MRIs can be a useful method in detecting regional disease. As regional lymph node metastases are a poor prognostic factor in RNETs [30,31,32,33], early detection is crucial to guide subsequent management. While 93% of MRIs were limited to the pelvis in our study, and the only abdominal MRI did not identify any metastases, MRIs are thought to have a greater sensitivity in detecting metastatic liver disease (71–99% [27]) compared to CT. ENETS guidelines list MRI as a potential first line modality for tumors > 10 mm [6, 18], suggesting its role in staging high grade lesions. SRS is another imaging modality commonly used for staging NETs, and while it was frequently performed in our study (18%), positivity rates were low (3%). Somatostatin receptors are more commonly found in low grade compared to high grade GEP-NETs and NECs [34], which can be useful for guiding functional imaging. NANETS guidelines emphasize its low sensitivity [5] relative to other imaging and does not recommend it as a staging modality. Similarly, MIBG scans may have utility in imaging pheochromocytomas or paragangliomas but have limited role in RNET imaging [28]. While both ENETS and NANETS highlight endoscopic ultrasound (EUS) evaluation of RNETs [5, 6], its role was minimally explored in our study as only 5 patients underwent EUS after initial endoscopy. The majority of studies suggest high (close to 100%) accuracy in EUS assessment of depth of invasion; but it may be limited in its ability to detect residual disease following biopsy [35]. EUS may have a role in surveillance for recurrence [36].
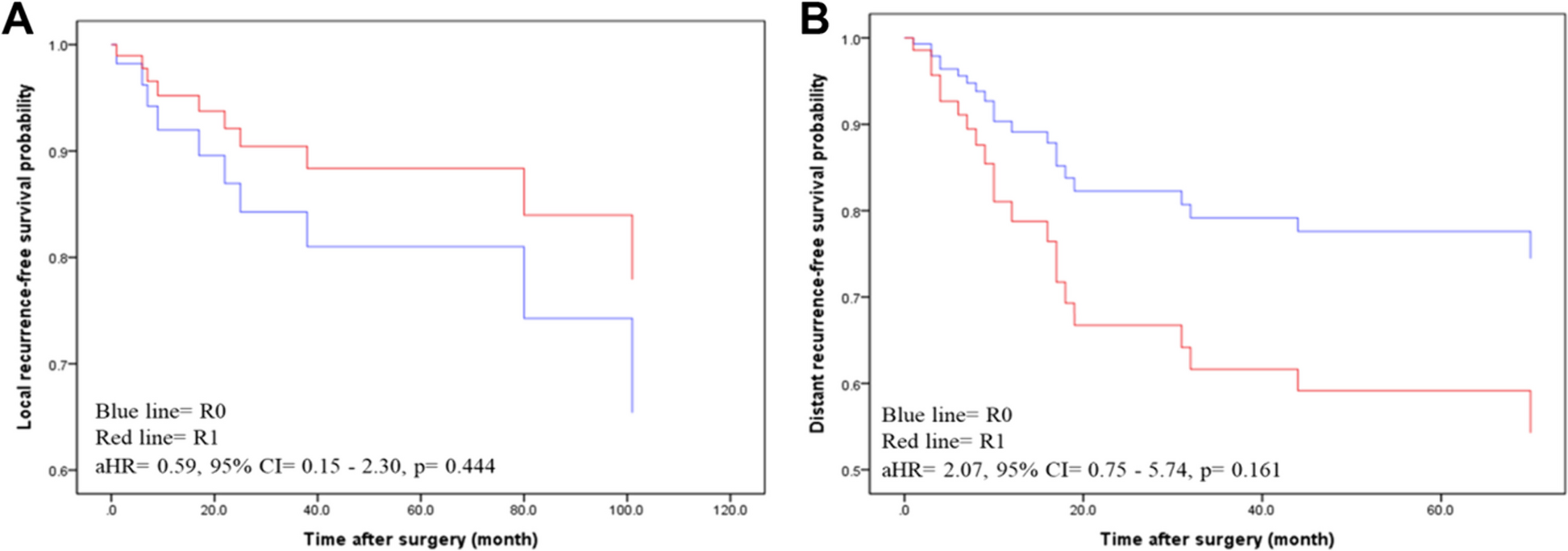
An important consideration in the management of RNETs is the role of further excision (local or anatomical) following initial diagnosis. The presence and/or location of microscopic residual disease can be difficult to discern after initial polypectomy making further intervention difficult. In our study, the presence of positive margins on initial biopsy was the most common reason for further intervention (51%) with 54% identifying residual malignant disease. However, a study by Sun et al. (2023) showed that the presence of positive margins after ESD for RNETs did not impact 5-year progression free survival or OS [37]. In our study, amongst 33% who underwent intervention after biopsy without clear documentation of positive margins, 50% detected malignant disease on final pathology. Further procedural decision-making should not solely rely on margin status but also take into consideration other tumor characteristics.
Current ENETS, NANETS and NCCN guidelines recommend local or endoscopic resections for tumors ≤ 20 mm and anatomic resections for tumors > 20 mm with a strong emphasis on tumor size [5, 23, 38]. Although ENETS and NCCN factors grade into decision-making when secondary resection is incomplete, it is not emphasized in initial procedural planning [6, 23]. In our study, the rate of local and anatomic resections was lower in patients with grade 1 compared to grade 2 disease. Within patients with grade 1 disease, local surgical resections were more commonly performed than anatomic resections. Several studies have shown that endoscopic resection techniques are adequate in completely resecting localized RNETs with one study quoting a 99% en bloc section rate [12]. A large Canadian study showed that TEM is effective for primary excisions and completion re-excisions with low recurrence rates (5%) [39]. Endoscopic full thickness resections (eFTR) are comparable to TEM [40], and are more effective than repeat biopsy of the scar [35] in achieving progression free survival and OS [37]. Endoscopic resection may be more efficient and less invasive compared to transanal resections [40] and could be considered for RNETs with low grade disease. In comparison, patients with grade 2 disease had a higher rate of R2 resections compared to those with grade 1 disease (33% vs. 2%) suggesting a need for radical interventions [30, 32]. They also underwent more anatomic than local resections, despite all lesions were smaller than 10 mm, suggesting that surgical decision-making should incorporate grade in addition to tumor size. Lastly, declining rates of 5-year OS based on grade (grade 1: 98%, grade 2: 67%, grade 3: 10%) parallels that reported by Weinstok et al. (grade 1: 87.7%, grade 2: 47.6%, grade 3: 33.3%) [41], which further highlights its role in the preoperative treatment algorithm [4, 41].
While tumor size is known to be a significant prognostic factor [5, 6, 42], recent studies have suggested that it may be insufficient in guiding staging, surgical decision-making [43] and prognosis [44]. RNETs ≥ 20 mm are scarce, making it difficult to assess statistical outcomes for this population [43]. Additionally, evaluation of tumor size at diagnosis may not be accurate if only a biopsy or partial polypectomy was performed. Few studies in other NETs such as appendiceal and gastroduodenal [45, 46] are exploring the incorporation of grade into their management algorithms. Other cancers such as breast have already incorporated grade into clinical prognostic staging [15]. With increasing literature evidence that grade is an important prognostic indicator for RNETs [22, 47], consideration of its addition to management algorithms is likely warranted.
Limitations
This study is limited by its retrospective design. Despite collecting 13 years’ worth of data, the population size was limited due to the low incidence of RNETs; therefore, it was not possible to perform regression or prediction analysis. A portion of our patient data were collected from regional cancer centres, where more aggressive disease tends to be referred, which may explain our higher rates of metastasis. We were unable to collect data on all patients in the province due to limitations in data sharing. Data for grade, tumor size, depth of invasion and specimen margin were often missing from old pathology reports, which limited the population size available for analysis. Results must also be interpreted with the limitation that data collection was performed prior to the 2019 World Health Organization change in grading criteria [48]. Six patients with grade 3 tumors did not undergo any intervention limiting their assessment. EMR or ESD data is not included as these were not commonly performed during the study period. Indication for further procedures may be inaccurate as margin data were often missing from pathology reports and documentation by physicians were often vague.





留言 (0)