
記住我

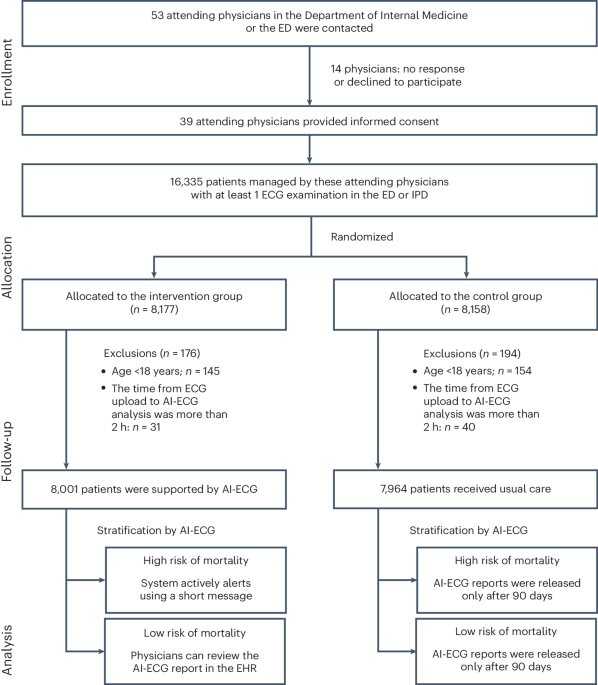


A total of 443 individuals were screened for participation in the PASADENA study, and 316 were enrolled: 105 were assigned to placebo, 105 to prasinezumab 1,500 mg and 106 to prasinezumab 4,500 mg (ref. 4).
Baseline characteristics of the participantsTwo of the six prespecified primary subpopulations (ɑ-synuclein skin positive on skin biopsy sections at baseline and dopamine transporter single-photon emission computed tomography (DaT-SPECT) striatal binding ratio (SBR) ipsilateral putamen <0.6) included fewer than 20% of participants from the mITT population at baseline and were not further analyzed. Thus, only four primary subpopulations were included in the final analyses: (1) MAO-B inhibitors at baseline (yes versus no); (2) Hoehn and Yahr stage (2 versus 1); (3) rapid eye movement (REM) sleep behavior disorder (yes versus no); and (4) data-driven subphenotypes (diffuse malignant versus nondiffuse malignant). Similarly, of the nine exploratory subpopulations, six were included in the final analyses: (1) age at baseline (≥60 years versus <60 years); (2) sex (male versus female); (3) disease duration (>12 months versus <12 months); (4) age at diagnosis (≥60 years versus <60 years); (5) motor subphenotypes akinetic–rigid versus tremor-dominant; and (6) motor subphenotypes postural instability gait dysfunction (PIGD) versus tremor-dominant. All primary and exploratory subpopulations were defined a priori in the statistical analysis plan before database lock of the study. Baseline demographic and clinical characteristics of the placebo and prasinezumab groups were comparable in the subpopulations of patients who received MAO-B inhibitors at baseline versus those who were treatment-naive (Table 2 and Supplementary Table 1), and in the other primary and exploratory subpopulations included in the analyses (Supplementary Table 1).
Table 2 Baseline demographic and clinical characteristics of the whole study population, participants taking MAO-B inhibitors at baseline and those who were treatment-naive at baselineMotor sign progression in the prespecified subpopulationsAnalyses were performed using two estimand strategies: the ‘hypothetical strategy’ assumes a scenario in which the events of start of symptomatic therapy or change in MAO-B inhibitor dose did not occur, and the ‘treatment policy strategy’ in which the treatment effect is estimated irrespective of symptomatic treatment start or changes in MAO-B inhibitor treatment (see Methods for further details).
The placebo groups in each prespecified rapidly progressing subpopulation declined faster than their nonrapidly progressing counterparts in motor function, as assessed by MDS-UPDRS Part III (Fig. 1 and Supplementary Fig. 1); for example, mean (s.e.) changes (with the hypothetical strategy) from baseline to week 52 were 6.82 (1.37) points in participants taking MAO-B inhibitors at baseline versus 5.04 (1.16) points in those who were treatment-naive; 6.34 (1.04) points in participants with Hoehn and Yahr stage 2 versus 2.17 (1.84) points in those with stage 1; 7.04 (1.30) points in those who were ≥60 years at baseline versus 3.83 (1.25) points in those aged <60 years; and 8.40 (1.59) points in participants with the motor subphenotype of PIGD versus 4.70 (1.11) points in those with tremor-dominant phenotype (Fig. 1, Table 3, Supplementary Fig. 1 and Supplementary Table 2).
Fig. 1: Forest plot of prasinezumab effects on motor progression as measured by the MDS-UPDRS Part III (hypothetical strategy) across the primary prespecified subpopulations.
Adj., adjusted; MAO-B, monoamine oxidase B; MDS-UPDRS, Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale; RBDSQ, Rapid Eye Movement Sleep Behavior Disorder Screening Questionnaire. Error bars represent 80% confidence interval (CI).
Table 3 Change from baseline at week 52 in the subpopulations of participants taking MAO-B inhibitors at baseline and those who were treatment-naive at baselineParticipants with and without MAO-B inhibitors at baselineWith the hypothetical strategy, the mean (s.e.) change from baseline to week 52 in MDS-UPDRS Part III score in the entire PASADENA placebo population was 5.57 (0.90) points (Table 3). The corresponding mean (s.e.) change from baseline in the placebo group of the subpopulation of participants taking MAO-B inhibitors was 6.82 (1.37) points, compared with 5.04 (1.16) points in the placebo group of the treatment-naive subpopulation (Table 3 and Fig. 2a). The differences in adjusted means from baseline at week 52 in the pooled prasinezumab group versus placebo were −2.66 points (80% CI, −4.87, −0.45; relative reduction (RR), −39.0%) in the subpopulation of participants taking MAO-B inhibitors at baseline and −0.87 points (80% CI, −2.69, 0.94; RR, −17.3%) in the subpopulation of participants who were treatment-naive (Table 3 and Fig. 2a). Results from the groups receiving low and high doses of prasinezumab were comparable (Supplementary Tables 3 and 4).
Fig. 2: Prasinezumab effect on motor signs progression assessed using MDS-UPDRS Part III in participants taking MAO-B inhibitors at baseline and those who were treatment-naive at baseline.
a, Hypothetical strategy. b, Treatment policy in OFF state. c, Treatment policy in ON state. The MDS-UPDRS endpoints were analyzed using mixed models for repeated measures. Error bars represent s.e. MAO-B inhibitors at baseline: prasinezumab pooled n = 77; placebo n = 38; treatment-naive at baseline: prasinezumab pooled n = 134; placebo n = 67. MAO-B, monoamine oxidase B; MDS-UPDRS, Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale.
Similar results were observed when MAO-B inhibitor subpopulation MDS-UPDRS Part III data were analyzed with the treatment policy strategy, both in OFF state (difference in adjusted means, −2.60 points; 80% CI, −4.51, −0.70; RR, −54.3%) (Table 3 and Fig. 2b) and in ON state (difference in adjusted means, −2.60 points; 80% CI, −4.57, −0.63; RR, −62.2%) (Table 3 and Fig. 2c).
Mean (s.e.) changes (with the hypothetical strategy) from baseline to week 52 in MDS-UPDRS Part II and Part I scores in the entire PASADENA placebo population were 2.75 (0.37) and 0.77 (0.30) points, respectively (Table 3). The mean (s.e.) changes from baseline to week 52 in MDS-UPDRS Part II score in the placebo subpopulations who were treated with MAO-B inhibitors and treatment-naive at baseline were 2.40 (0.64) and 2.89 (0.47) points, respectively, and the corresponding values for MDS-UPDRS Part I score were 1.28 (0.47) and 0.38 (0.37) points, respectively (Table 3). No differences were found between the prasinezumab and the placebo groups on MDS-UPDRS Part II and Part I, using either the hypothetical or treatment policy strategies (Table 3).
Participants with Hoehn and Yahr stage 1 and 2With the hypothetical strategy, the mean change (s.e.) from baseline to week 52 in MDS-UPDRS Part III score in the placebo group of the Hoehn and Yahr stage 2 subpopulation was 6.34 (1.04) points, compared with 2.17 (1.84) points in the placebo group of the Hoehn and Yahr stage 1 subpopulation (Fig. 1 and Supplementary Table 2). The differences in adjusted means from baseline at week 52 in the prasinezumab group versus placebo were −2.55 points (80% CI, −4.19, −0.9; RR, −40.2%) in the Hoehn and Yahr stage 2 subpopulation and 3.14 points (80% CI, 0.32, 5.95; relative change, +144.7%) in the Hoehn and Yahr stage 1 subpopulation (Fig. 1 and Supplementary Table 2).
When the MDS-UPDRS Part III data for the Hoehn and Yahr stage 2 subpopulation were analyzed with the treatment policy, the differences in adjusted means in OFF state and ON state were −1.33 points (80% CI, −2.76, 0.11; RR, −35.1%) and −1.51 points (80% CI, −3.02, 0.00; RR, −54.1%), respectively (Supplementary Table 2).
The mean changes (s.e.) (with the hypothetical strategy) from baseline to week 52 in MDS-UPDRS Part II score in the placebo groups of the Hoehn and Yahr stage 2 and stage 1 subpopulations were 3.01 (0.43) and 1.68 (0.70) points, respectively, and the corresponding values for MDS-UPDRS Part I score were 1.05 (0.33) and −0.18 (0.65) points, respectively (Supplementary Table 2). No differences were found between the prasinezumab and the placebo groups on MDS-UPDRS Part II and Part I, using either the hypothetical strategy or treatment policy (Supplementary Table 2).
Participants with and without REM sleep behavior disorderWith the hypothetical strategy, the mean change (s.e.) from baseline to week 52 in MDS-UPDRS Part III score in the placebo group of the subpopulation with REM sleep behavior disorder was 7.76 (2.01) points, compared with 4.98 (1.01) points in the placebo group of the subpopulation without REM sleep behavior disorder (Fig. 1 and Supplementary Table 2). The differences in adjusted means from baseline at week 52 in the prasinezumab group versus placebo were −2.76 points (80% CI, −5.78, 0.25; RR, −35.6%) in the subpopulation with REM sleep behavior disorder and −1.03 points (80% CI, −2.63, 0.57; RR, −20.7%) in the subpopulation without REM sleep behavior disorder (Fig. 1 and Supplementary Table 2).
When the MDS-UPDRS Part III data for the subpopulation with REM sleep behavior disorder were analyzed with the treatment policy, the differences in adjusted means in OFF state and ON state were −1.21 points (80% CI, −3.92, 1.49; RR, −22.2%) and −0.04 points (80% CI, −2.80, 2.71; RR, −1.1%), respectively (Supplementary Table 2).
The mean changes (s.e.) (with the hypothetical strategy) from baseline to week 52 in MDS-UPDRS Part II score in the placebo groups of the subpopulations with and without REM sleep behavior disorder were 2.19 (0.86) and 2.82 (0.42) points, respectively, and the corresponding values for MDS-UPDRS Part I score were 1.28 (0.60) and 0.69 (0.34) points, respectively (Supplementary Table 2). No differences were found between the prasinezumab and the placebo groups on MDS-UPDRS Part II and Part I, using either the hypothetical strategy or treatment policy (Supplementary Table 2).
Participants with diffuse and nondiffuse malignant phenotypesWith the hypothetical strategy, the mean change (s.e.) from baseline to week 52 in MDS-UPDRS Part III score in the placebo group of the diffuse malignant subpopulation was 12.29 (3.45) points, compared with 4.76 (0.91) points in the placebo group of the nondiffuse malignant subpopulation (Fig. 1 and Supplementary Table 2). The differences in adjusted means from baseline at week 52 in the prasinezumab group versus placebo were −7.86 points (80% CI, −12.90, −2.82; RR, −64.0%) in the diffuse malignant subpopulation and −0.77 points (80% CI, −2.20, 0.66; RR, −16.2%) in the nondiffuse malignant subpopulation (Fig. 1 and Supplementary Table 2).
When the MDS-UPDRS Part III data for the diffuse malignant subpopulation were analyzed with the treatment policy, the differences in adjusted means in OFF state and ON state were −2.58 points (80% CI, −6.18, 1.02; RR, −49.9%) and −2.76 points (80% CI, −6.67, 1.15; RR, −72.4%), respectively (Supplementary Table 2).
The mean changes (s.e.) (with the hypothetical strategy) from baseline to week 52 in MDS-UPDRS Part II score in the placebo groups of the diffuse malignant and nondiffuse malignant subpopulations were 4.08 (1.53) and 2.47 (0.37) points, respectively, and the corresponding values for MDS-UPDRS Part I score were 1.59 (1.13) and 0.76 (0.29) points, respectively (Supplementary Table 2). No differences were found between the prasinezumab and the placebo groups on MDS-UPDRS Part II and Part I, using either the hypothetical strategy or treatment policy (Supplementary Table 2).
Participants in the prespecified exploratory subpopulationsA greater beneficial effect for prasinezumab versus placebo was also shown in all prespecified exploratory subpopulations with more rapidly progressing disease compared with their nonrapidly progressing counterparts (Supplementary Fig. 1 and Supplementary Table 2); for example, the differences in adjusted means in MDS-UPDRS Part III scores (with the hypothetical strategy) for pooled prasinezumab versus placebo in participants with age at baseline ≥60 years and <60 years were −1.89 points (80% CI, −3.90, 0.12; RR, −26.9%) and −0.61 points (80% CI, −2.58, 1.36; RR, −15.9%), respectively (Supplementary Fig. 1 and Supplementary Table 2). Results from the groups receiving low and high doses of prasinezumab were comparable for the exploratory as well as the primary subpopulations (Supplementary Tables 3 and 4).
Sensitivity analysesAt baseline, the subpopulations might have differences in baseline characteristics (for example, participants treated with MAO-B inhibitors had a longer disease duration, lower DaT-SPECT SBR and different proportions of patients with Hoehn and Yahr stage 1 and 2 compared with the treatment-naive population, whereas the MDS-UPDRS Parts I, II and III scores were comparable) (Table 1). Therefore, the primary analyses were repeated for all subpopulations including all baseline characteristics as covariates. These analyses resulted in the same pattern of results as the primary analyses (results not shown).
留言 (0)