2.1 Trial Design
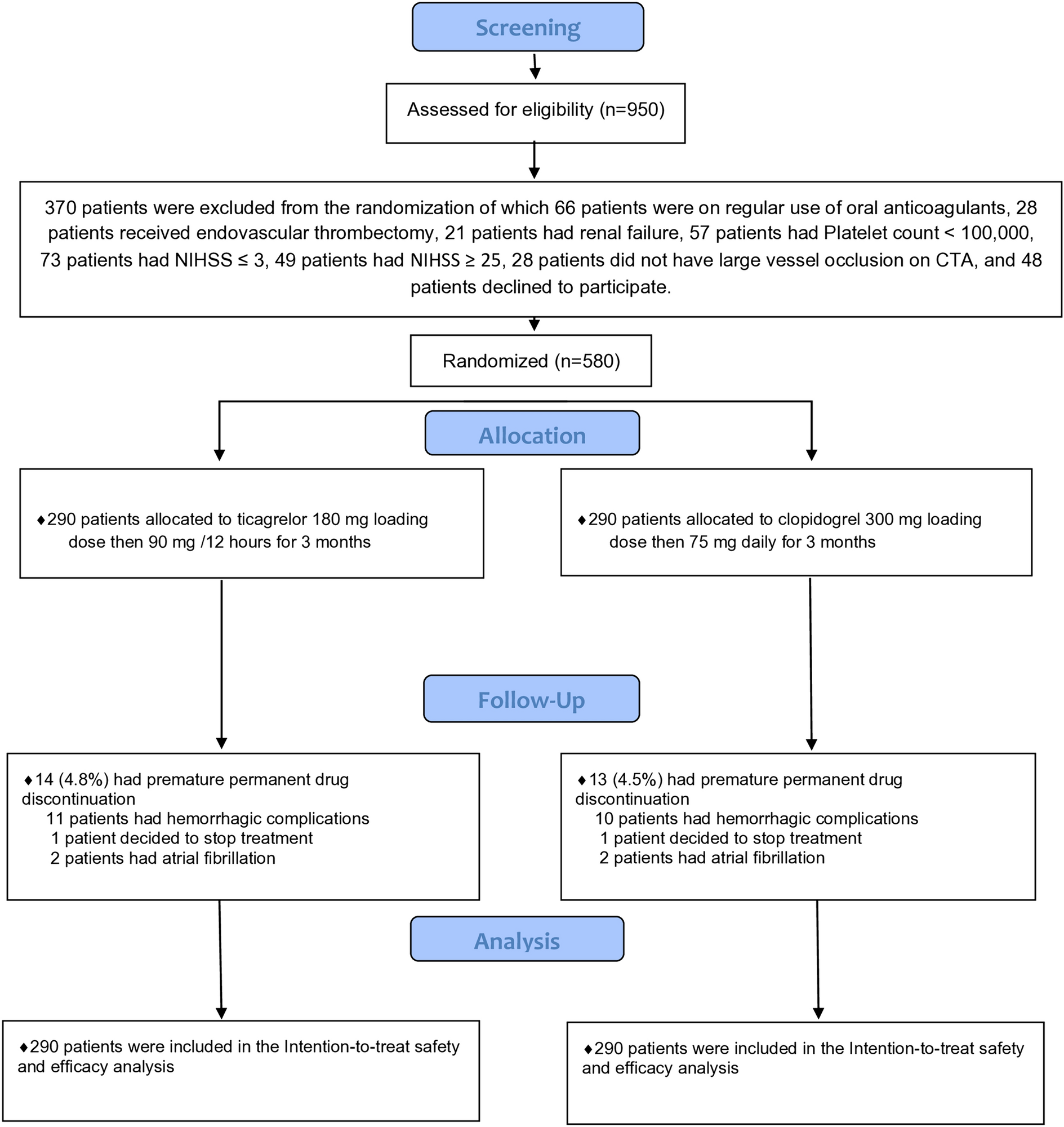
After receiving approval from the ethics council of the Faculty of Medicine at Kafr el-Sheikh University, we executed our single-blinded, randomized controlled study and screened all patients presenting with their first-ever LVO ischemic stroke who sought medical advice in Kafr-Elsheikh Hospital and Nasr City Insurance Hospital during the period from July 1, 2022 to November 1, 2023. The last patient was enrolled in our study on July 15, 2023; we followed up patients for 90 days after stroke onset. In a one-to-one ratio, 580 first-ever LVO stroke participants were randomly assigned to receive loading and maintenance doses of ticagrelor or clopidogrel.
2.2 Participants
We had two parallel groups. The (A) group included 290 patients who received a 180-mg loading dose of ticagrelor during the first 24 hours following stroke onset, followed by 90 mg twice daily from day 2 to day 90. The (B) group included 290 patients who received a 300-mg loading dose of clopidogrel followed by 75 mg once daily from the Day 2 to Day 90).
2.3 Eligibility Criteria
We enrolled males and females aged 18–75 years with their first-ever large-vessel arterial ischemic stroke. Large-vessel stroke was defined according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification when patients had clinical and brain imaging findings of >50% stenosis or occlusion of at least one of the following arterial segments on computed tomography angiography (CTA) or magnetic resonance angiography (MRA) if CTA was contraindicated: intracranial portion of internal carotid arteries, middle cerebral arteries (M1/M2), intracranial portion of vertebral arteries, and basilar artery, and patients had cortical or cerebellar lesions and brain stem or subcortical hemispheric infarcts > 1.5 cm in diameter on CT or MRI, and there were no potential sources of cardiogenic embolism [12].
We did not exclude patients with previous transient ischemic attack (TIA). All patients were ineligible for recombinant tissue plasminogen activator (rt-PA) therapy or thrombectomy to avoid clouding safety assessment [13].
We excluded patients with allergies to any of the studied drugs or who suffered from clinical seizures as a part of their stroke, those with major organ failure, malignancies, or myocardial infarction during the past 6 weeks, and patients who took regular antiplatelets or anticoagulants in the previous week to avoid clouding our drug safety assessment [13].
We excluded patients with a minor stroke (National Institutes of Health Stroke Scale [NIHSS] ≤ 3) or severe stroke (NIHSS ≥ 25), patients who had spontaneous resolution of symptoms before imaging, and patients with history of a CNS disorder (e.g., multiple sclerosis, epilepsy, meningioma). Patients were also not eligible if carotid, cerebrovascular, or coronary revascularization was planned, requiring halting study treatment within 7 days after randomization.
Patients who experienced a cardioembolic stroke either prior to or post-treatment were not included in our study. Cardio-embolic strokes were diagnosed when the patient exhibited a potential cardiac source of embolus such as mechanical cardiac valves, atrial fibrillation (AF), mitral valve prolapse, aortic valve stenosis or calcification, and patent foramen ovale [14]. Patients were diagnosed with clinical AF based on the presence of a conventional 12-lead electrocardiography (ECG) recording that exhibited a minimum of 30 seconds of cardiac rhythm, showing the absence of identifiable recurring P waves and irregular RR intervals (when atrioventricular conduction is not impaired) [15].
We excluded patients with a source of gastrointestinal bleeding such as peptic ulcers, patients with recurrent stroke based on appropriate clinical history, examination, and/or MRI brain findings, and those who had a blood glucose level < 50 or > 400 mg/dL or platelet count < 100,000 or international normalized ratio > 1.4 or prothrombin time > 18.
We excluded patients who were regular users of drugs that affected clopidogrel metabolism, such as proton pump inhibitors, ketoconazole, dihydropyridine calcium channel blockers, and rifampin [16]. We also excluded pregnant or lactating females, patients with venous infarction, and ischemic infarction secondary to hypo-perfusion.
2.4 Interventions
We evaluated all patients with their first-ever large-vessel ischemic stroke who presented to Kafr-Elsheikh Hospital and Nasr City Insurance Hospital in the period from September 1, 2021 to September 1, 2023, recording detailed personal history, risk factors assessment, and the onset of stroke. Every patient screened for eligibility had a 12-lead routine ECG and transthoracic echocardiography (TTE) to detect atrial fibrillation and valvular heart diseases before enrolment in the study.
Baseline laboratory examinations (including lipid profiles, liver functions, coagulation profiles, complete blood counts, and fasting and postprandial blood glucose levels and HbA1C), carotid duplex imaging, and continuous cardiac rhythm monitoring for 1 day were performed for all patients after enrolment. Blood pressure was also assessed, and we diagnosed hypertension when systolic blood pressure was > 130 mmHg and/or diastolic blood pressure was > 85 mm/Hg on at least three different occasions [17].
We diagnosed diabetes mellitus when the fasting plasma glucose level was > 126 mg/dL and/or casual plasma glucose was > 200 mg/dL, and/or HbA1C was > 6.5 [17], and we diagnosed admission hyperglycemia when the admission blood glucose value was > 140 mg/dL [18]. Regarding managing hyperglycemia, we aimed to maintain blood glucose levels below 140 mg/dL and 180 mg/dL. We withheld all usual antidiabetic treatments and used periodic subcutaneous regular insulin injections, adjusted according to blood glucose levels. Patients received rapid-acting insulins immediately after meals based on the amount of carbohydrates consumed. Four units of rapid-acting analog insulin were used for standard meals containing 60 g of carbohydrates, and the blood glucose level was followed up every 3 hours. If the blood glucose concentration did not reach the target at 24 and 48 hours, the subcutaneous insulin dose, including long-acting basal insulin, was increased [19].
We diagnosed hyperlipidemia when blood cholesterol was >200 mg/dL, triglycerides were >150 mg/dL, low-density lipoprotein cholesterol (LDL-C) was >100 mg/dL and/or high-density lipoprotein cholesterol (HDL-C) was <40 mg/dL [20]. Regarding the management of hyperlipidemia, patients received rosuvastatin 20 mg daily and ezetimibe 10 mg to achieve LDL-C <70 mg/dL. We chose rosuvastatin as, among the statins, simvastatin, lovastatin, and atorvastatin are metabolized by cytochrome P450 3A4 (CYP3A4), fluvastatin is metabolized by CYP2C9, while rosuvastatin undergoes little metabolism and has limited drug–drug interaction with clopidogrel [21]. After 4–12 weeks of starting anti-hyperlipidemia agents, we performed a follow-up fasting lipid profile [22].
Every patient underwent brain CT and brain MRI using the following stroke protocol: T1W, T2W, fluid-attenuated inversion recovery (FLAIR), diffusion weighted imaging (DWI), T2 gradient-echo, CTA, or MRA (if CTA was contraindicated), from the aortic arch through the circle of Willis. Two neuroradiologists blinded to treatment reviewed CT and MRI source images. Cerebrovascular vessels were divided into segments: supra-clinoid internal carotid artery, first-division middle cerebral artery (M1), second-division middle cerebral artery (M2), basilar artery (BA), and intracranial vertebral artery (VA). A neuroradiologist determined whether any of these vascular segments were occluded. If there was no vascular occlusion, the patient was documented as having no large vessel occlusion. If one or more vascular segments were occluded and the patient was ineligible for thrombectomy or arterial stenting, the case history and NIHSS score were reviewed; if the vascular occlusion was in the appropriate territory to account for the clinical findings, the case was judged as having a large-vessel occlusion.
Our study follow-up was via telephone calls twice per week and a face-to-face interview in the outpatient clinic once per month, and continued for 3 months. If any of our patients complained of symptoms suggesting recurrent stroke in the follow-up calls, they were advised to go to the hospital.
2.5 Outcomes2.5.1 Primary Outcomes
The primary efficacy outcome was a new stroke event (ischemic or hemorrhagic) at 90 days in each group [7], while the primary safety outcome was the rate of hemorrhagic complications evaluated using the PLATO bleeding definition, which classified hemorrhagic complications into three types: major, minor, and minimal bleeding [23].
Hemorrhagic infarction was detected using a follow-up CT brain scan after 2 days and after 1 week or discharge; additionally, the European Cooperative Acute Stroke Study (ECASS) classification [24] was used to detect the type of hemorrhagic infarction.
2.5.2 Secondary Outcomes
The secondary efficacy outcomes were the rates of patients who achieved a significant reduction in NIHSS (decrease of four points or more) [25] on the day 7 or discharge, the rates of favorable outcome with modified Rankin scale (mRS) of 0–2 [26] after 1 week and 90 days, and rates of a composite of new stroke, myocardial infarction and death due to vascular events during the follow-up period. The secondary safety outcomes were the rate of treatment-related adverse effects assessed by a follow-up questionnaire and the rate of death due to vascular or non-vascular causes in each group.
2.6 Sample Size
After using Power Analysis & Sample Size System (PASS, V12, NCSS), we determined that a total of 524 large-vessel ischemic stroke patients would provide 80% power to detect a relative risk reduction of 35% in new ischemic stroke (primary outcome) in the ticagrelor group as compared with the clopidogrel group, with a final two-sided significance level of 95% and alpha error of 5%, assuming an incidence of new ischemic stroke of 13.6% [27] in the clopidogrel group and an overall dropout rate of 5%. The final size of our trial was 580 patients, 290 patients in each group.
2.7 Randomization and Blinding
Before assigning patients to a group, we collected written informed consent from them or their next of kin.
Our study was single-blinded to the investigators; an independent statistician generated a computer-generated randomization chart with a block size of four in a one-to-one ratio, and participants were randomly assigned to receive either ticagrelor or clopidogrel by a specially trained and qualified nurse. None of the investigators included in the study knew the patients’ assignments. We prepared 580 labels denoting either Drug A or Drug B. According to the randomization chart, these were placed into sequentially numbered opaque sealed envelopes numbered 1–580. Patients were given enrolment numbers starting from 1. Envelopes carrying the same number as the patient enrolment number were attached to the corresponding file. Once opened, the patients were assigned to receive Drug A or Drug B. Drug A comprised ticagrelor pills and Drug B comprised clopidogrel pills. The statistical analysis was performed by an independent statistician who did not know which treatment protocol was assigned for groups A and B. The follow-up calls were made by a specially trained and qualified nurse who was in contact with a neurology consultant; a consultant neurologist and a specially trained nurse conducted the follow-up interviews. All patients were asked not to tell the physician about their treatment. We did not use a placebo in our trial due to a lack of funding and financial support.
2.8 Statistical Analysis of the Data
We used the IBM SPSS software package, version 20.0 (IBM Corp., Armonk, NY, USA), to analyze our data and based all efficacy and safety analyses on the intention-to-treat principle. Both the primary and secondary outcomes underwent separate statistical analyses. Depending on their distribution, as determined by the Shapiro–Wilk test, we described numerical data as mean and standard deviation (SD) or median and interquartile range (IQR). We also reported categorical data using numbers and percentages. The Mann–Whitney U test was used to compare the irregularly distributed numerical data, while Pearson’s Chi-square was utilized to correlate categorical data. In our study, all the data were included. All statistical analyses were two-sided, and differences with a p value of <0.05 were considered statistically significant. To avoid type 1 statistical errors in the analysis of secondary efficacy outcomes, we used correction for multiple comparisons, and secondary efficacy outcomes differences with an adjusted p value of < 0.0125 were considered statistically significant. Survival analysis was performed using the Kaplan Meier test and log-rank method to study the effect of the antiplatelet on the incidence of outcomes during the 3-month follow-up period. The Cox regression method obtained the hazard ratio (HR) at a 95% confidence interval (CI). An HR is considered significant when it does not fall between the lower and upper CI.








留言 (0)