
記住我


Hoarding disorder (HD) is a common and debilitating mental illness that causes personal disability and poses significant health and safety risks (APA, 2013; Tolin et al., 2008). It is marked by difficulty discarding possessions, which results in clutter that often makes living spaces unusable (APA, 2013; Tolin et al., 2008). Cognitive behavioral therapy (CBT) improves symptoms of HD for many (Tolin et al., 2015), but a considerable proportion refuse treatment (44%; Steketee et al., 2010) or drop out of treatment prematurely (10%–29%; Saxena et al., 2011; Steketee et al., 2010). In addition to primary symptoms around difficulty discarding, people with HD have a host of other concomitant difficulties such as sleep disturbance and poor nutrition (Frost et al., 2012; Mahnke et al., 2021). Research is needed to develop alternative approaches for helping people with HD who are not ready to engage in CBT or who do not have access to it.
Imaginal exposure (IE) is an intervention strategy shown to improve symptoms of worry, anxiety disorders, and obsessive-compulsive disorder (OCD) (Abramowitz, 2018; Robichaud and Dugas, 2015). It involves repeatedly evoking mental images of feared and avoided scenarios for sustained periods to practice tolerating (vs. avoiding) uncomfortable emotions and concerns. IE can be used alongside or as a stepping stone to in vivo engagement (i.e., “real life”) exposure (Whiteside et al., 2022), in part because it is more tolerable to imagine a feared scenario than to confront one in vivo. The combination of imaginal and in vivo can be superior to in vivo alone (Abramowitz, 1996; Hunt and Fenton, 2007), although expert clinicians advise against stopping with only an IE when in vivo is also possible (Emmelkamp, 2004; Gillihan et al., 2012). One situation especially appropriate for IE is when the fear is far in the future and cannot logically be disconfirmed (e.g., one is punished for discarding a receipt now needed for their taxes; Gillihan et al., 2012). Thus, IE may be useful alongside criterion standard interventions such as in vivo exposure. Despite suggestions from CBT researchers that IE could reduce hoarding behaviors (Tolin et al., 2007), IE's impact on HD remains unknown.
There are many modalities to facilitate IE, including through writing, recording audio, or speaking with a therapist. All of these have elicited significant symptom improvements in anxiety disorders and OCD, as well as in underlying processes (e.g., emotional avoidance; Berman et al., 2021; Foa et al., 1980; Fracalanza et al., 2014). Certain studies have found that the varying imagined feared scenario is beneficial (Lang and Craske, 2000), whereas others have found that consistent exposure to the same feared scenario is preferable (Sloan et al., 2005). It has been suggested that complex mental images (e.g., picturing a several-minute feared scenario) are more amenable to repetition, whereas simple images (e.g., picturing a snake) are more amenable to varied content (Fracalanza et al., 2014); picturing imagined discarding scenario entails more complex mental imagery.
IE is often included as part of evidence-based CBT practices (Dugas and Robichaud, 2007). Only a few studies have examined IE as standalone techniques, and the methods used in these studies have varied considerably—from, for generalized anxiety disorder, twelve 1-hour therapy sessions (Provencher et al., 2004) to five 30-minute writing sessions (Goldman et al., 2007). Indeed, researchers have called for the need to test a range of procedural variants to determine which variation yields the greatest impact (Fracalanza et al., 2014).
A previous noncontrolled case series found preliminary evidence in support of IE for HD (Fracalanza et al., 2021), which was demonstrated to be feasible, useful, and associated with symptom improvement. This initial case series used the same written IE approach described in the present study (i.e., writing about a feared discarding scenario for 20 minutes per day on three consecutive days), with the exception that this previous study was administered in an in-person group format rather than remotely. This suggested that IE for HD merited further clinical investigation, with a controlled pilot study being a sensible next step.
Based on these previous studies, the present study investigates whether written IE yields greater improvement in HD symptoms, particularly self-reported difficulty discarding, compared with a control writing (CW) condition. This study also explores the impact of IE on two underlying HD processes: emotional avoidance and intolerance of uncertainty, both of which have been associated with HD (Wheaton et al., 2016; Wheaton et al., 2011). Emotional avoidance is the unwillingness to endure unpleasant internal experiences, which can lead to attempts to suppress negative affect (Berman et al., 2010), and exposure to such unpleasant affect via IE may help to reduce emotional avoidance. Intolerance of uncertainty is the tendency to exhibit negative responses to uncertain situations, which may underlie a difficulty making decisions about which items to discard. Indeed, HD patients commonly report saving possessions because they are unsure if the items will be needed in the future (Wheaton et al., 2016). Tolerating the distress of uncertainty via IE may help reduce intolerance of it.
The present study is the first known randomized controlled pilot trial to test IE for HD. If IE yields significant symptom improvement that surpasses that of CW, this would provide evidence of IE as a promising novel treatment for HD. If it yields nonsignificant symptom change or change equivalent to that of CW, this would fail to demonstrate the efficacy of IE for HD and could speak to either exploration of alternative novel approaches or to the need for future studies of IE for HD to use a different instructional approach than that used here.
METHODS ParticipantsInterested individuals were invited to participate if they were older than 18 years, diagnosed with HD via the SCID-5-RV HD module administered by postdoctoral psychologists or psychiatrists (First et al., 2015), reported clinically significant hoarding symptoms (Saving Inventory Revised [SIR] score >41), and had clutter that impaired living conditions as assessed via clinician-rated videoconferencing (Clutter Image Rating [CIR] score >4). Participants were excluded if they were at risk of suicide (Columbia Suicide Severity Rating Scale >3; Posner et al., 2011) or currently in CBT for HD. Psychotropic medication was allowed if the dose was stable for at least 4 weeks (8 weeks for fluoxetine) before study start. In total, 64 individuals were screened, and 37 met inclusion criteria. Five people screened dropped out before completing study measures, providing a final sample of 32 adults with HD.
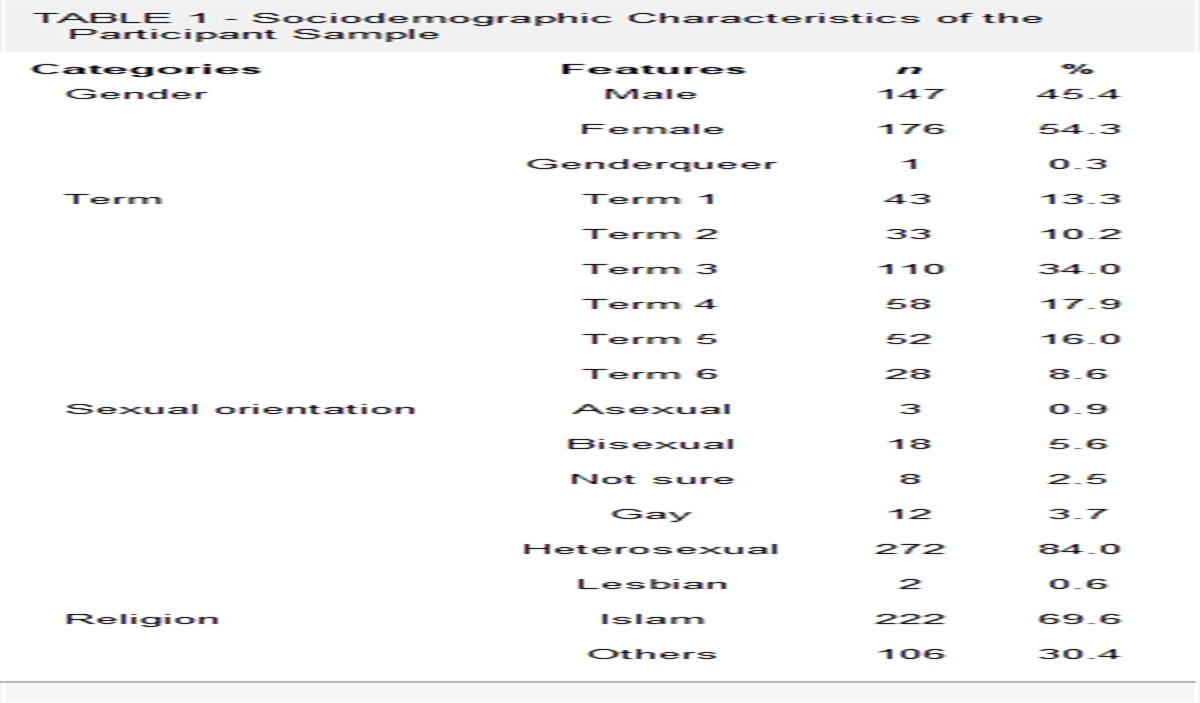
Demographic information about the sample can be found in Table 1. The sample was predominantly female (87%), with a mean age of 52.91 (SD = 13.79; range, 22–73). The mean SIR score (M = 62.50, SD = 12.45) of participants in the current study was comparable to that of other clinical HD samples (e.g., Kellman-McFarlane et al., 2019; Tolin et al., 2010). Most were recruited via online advertisements (83%), whereas others were recruited by invitation if they had participated in a prior study with the laboratory and indicated interest in additional studies.
TABLE 1 - Sample Characteristics by Condition (n = 32) Characteristic IE (n = 17) CW (n = 15) Age in years, M (SD) 56.94 (10.74) 48.33 (15.71) Sex, frequency (%) Female 14 (82%) 14 (93%) Male 3 (18%) 1 (7%) Race/ethnicity, frequency (%) White 8 (47%) 10 (67%) Black — — East Asian 4 (24%) 4 (27%) Southeast Asian — — Latin American 3 (18%) — Mixed race 2 (12%) — Other ethnicity — 1 (7%) Highest education, frequency (%) High school diploma — 3 (20%) College diploma 6 (35%) — Bachelor's degree 6 (35%) 10 (67%) Master's degree 2 (12%) — Doctoral degree 1 (6%) 1 (7%) Other 2 (12%) 1 (7%) Employment status, frequency (%) Not working (including student) 5 (29%) 2 (13%) Employed (full or part-time) 9 (53%) 9 (60%) Retired 3 (18%) 4 (27%) Marital status, frequency (%) Single 6 (35%) 9 (60%) Married/common-law 9 (53%) 4 (27%) Divorced 2 (12%) 2 (13%) Widowed — —To increase sensitivity to weekly change, all self-report questionnaires instructed participants to reflect on their experiences “in the past week.”
HD MeasuresThe SIR (Frost et al., 2004) is the criterion standard self-report measure of hoarding symptom severity, comprising three subscales: clutter severity, difficulty discarding, and excessive acquisition. It has excellent internal consistency and good test-retest reliability. A single composite score ranges from 0 to 92, with higher scores indicating greater severity. Internal consistency in the present study was good, α = 0.93.
The Saving Cognitions Inventory (SCI; Steketee et al., 2003) is a self-report measure of beliefs related to discarding possessions, for example, overresponsibility for items and reliance on items for memory. It includes cognitions across four subscales: emotional attachment to items, overresponsibility for items, reliance on items for memory, and need for control over items. The SCI has demonstrated good internal consistency (Steketee et al., 2003) and is a significant predictor of hoarding behaviors (Wheaton et al., 2011). A single composite score ranges from 24 to 168. Internal consistency in the present study was good, α = 0.96.
The Compulsive Acquisition Scale (CAS; Frost et al., 2002) is a self-report measure of the degree to which one feels compelled to acquire possessions. The CAS has good reliability and discriminates compulsive buyers from controls (Frost et al., 2002; Kyrios et al., 2004). A single composite score ranges from 18 to 126. Internal consistency in the present study was good, α = 0.96.
The CIR scale (Frost et al., 2008) is a rating of home clutter, administered virtually by independent evaluators. On a scale of 1–9, degree of clutter is matched to one of nine photographs depicting various levels of clutter; this is done for several rooms in the home. A score of 4 or more in a room indicates clinically significant clutter requiring clinical attention. The CIR has demonstrated high internal consistency, test-retest reliability, and interrater reliability (Frost et al., 2008). Here, a CIR-Total score was calculated by averaging the room scores of the three types of rooms that all participants had (a kitchen, a living room, and a bedroom), for a composite score that ranges from 1 to 9.
Transdiagnostic Process MeasuresThe Intolerance of Uncertainty Scale (IUS; Buhr and Dugas, 2002) is a self-report measure of distress in the face of uncertainty. It has demonstrated excellent internal consistency, good test-retest reliability, and construct validity (Sexton and Dugas, 2009). A single composite score ranges from 27 to 135, with higher scores indicating greater intolerance. Internal consistency in the present study was good, α = 0.98
The Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011) is a 7-item measure of emotional avoidance. The AAQ-II has shown good internal consistency, reliability, and convergent validity (Bond et al., 2011). A single composite score ranges from 7 to 49, with higher scores indicating greater emotional avoidance. Internal consistency in the present study was good, α = 0.95.
Procedure Random Assignment to Experimental ConditionsParticipants were randomly assigned to the IE condition (n = 17) or the CW (n = 15) condition. Participants in both conditions wrote for 20 minutes on three consecutive days, based on a meta-analysis showing that 15 or more minutes of writing over three or more days has significant and large positive effects on a range of psychological outcomes, whereas writing for fewer days has smaller effects (Frattaroli, 2006). Participants were sent writing instructions daily, on the three consecutive days, via a link. Instructions noted that participants were required to stay focused on their assigned writing topic, write at least 250 words, and that the writing must be timestamped for at least 20 minutes.
Writing Procedures Imaginal ExposureThe IE writing instructions were similar to those from prior research on written IE for generalized anxiety and worry, wherein participants are asked to write about their worst-case scenario coming true in the first person, present tense, and with reference to their emotional experiences, thoughts, and sensations (Goldman et al., 2007; Fracalanza et al., 2014). Instructions were modified from this prior research to ask participants to write about their worst-case scenario related to discarding a possession(s), to ensure relevance to HD concerns specifically. For example, “I donated a jacket that I really like, and now that it's getting cold, I need to spend money that I don't have just to replace it. I'm so anxious about spending money and feel angry at myself for parting with it.” Per prior research on optimizing the effectiveness of brief IE (e.g., Fracalanza et al., 2014), participants wrote about the same scenario on all 3 days. These instructions were also previously used in an initial case series on IE for HD (Fracalanza et al., 2021).
Control WritingThe control group was asked to write about what they would do if they found out that they had a day off. They were asked to write in a factual manner, with no references to emotions or opinions, as per the control procedure in other written IE studies (e.g., Frattaroli, 2006; Goldman et al., 2007). For example, “I get up in the morning and check my emails. I respond to the many unread messages. Then I get my things ready and head out to the beach. I decide to walk there.” All participants wrote about their assigned topics, as reviewed by two independent evaluators (K.F. and T.A.).
AssessmentsParticipants completed the same battery of self-report questionnaires immediately before writing on day 1 (pre), immediately after writing on day 3 (post), and on day 10, 1 week after the intervention (follow-up). The battery included HD measures (SIR, SCI, CAS, and CIR) and transdiagnostic process measures (IUS and AAQ-II). To examine longer-term impact, pre to follow-up was examined.
Interaction With Study StaffStudy staff first interacted with participants through Zoom during the screening process (at which time study staff explained the study procedures to participants) and whenever participants required assistance with study tasks. Throughout the study, study staff and participants maintained regular email communication.
RESULTSWe tested whether written IE (the IE condition) improved HD symptoms and related processes relative to CW (the CW condition). Pre and follow-up scores on all measures, in both conditions, are shown in Table 2.
TABLE 2 - Means and Standard Deviations on HD Symptoms and Processes by Condition (n = 32) Measure Time IE (n = 17) CW (n = 15) SIR-Total score Pre 62.41 (13.22) 62.60 (11.97) Follow-up 53.41 (16.87) 52.00 (14.05) SIR–Difficulty Discarding subscale Pre 20.65 (4.46) 20.13 (4.19) Follow-up 18.06 (5.52) 17.47 (5.59) SCI Pre 96.76 (35.47) 99.87 (36.33) Follow-up 86.88 (45.04) 77.33 (42.83) CAS Pre 62.88 (29.59) 57.93 (27.68) Follow-up 56.76 (30.47) 47.47 (23.52) CIR-Total score Pre 3.88 (1.46) 3.82 (1.72) Follow-up 3.39 (1.51) 3.38 (1.55) IUS Pre 68.47 (31.63) 72.27 (28.86) Follow-up 65.06 (33.27) 65.47 (30.21) AAQ-II Pre 24.94 (12.40) 28.33 (10.93) Follow-up 22.06 (12.47) 22.13 (11.87)To test whether these pre to follow-up changes were significant in each of the two conditions, we used paired sample t-tests. Examining pre to follow-up change scores in HD symptoms in the IE condition, we found significant improvements in SIR-Total, SIR-DD, CAS, and CIR scores, p's < 0.030, although nonsignificant improvement in SCI score, p = 0.053. However, unexpectedly, we also found significant improvements in the CW condition on these measures, including on the SCI, p = 0.012. Examining pre to follow-up change scores in transdiagnostic processes in the IE condition, we found no significant improvements, p's > 0.086. However, unexpectedly, we found significant improvements in the CW condition on the IUS and AAQ-II, p's < 0.011. These findings are shown in Table 3.
TABLE 3 - Change Score Comparison Between Written IE (n = 16) and CW (n = 15) Conditions Measure Condition Mean % Decrease Within-Condition Pre to Follow-Up Comparisona Cohen's d Between-Condition Comparison SIR IE 14.42 t = 3.84, p = 0.001* 0.93 F = 0.15, p = 0.697 CW 16.93 t = 3.21, p = 0.006* 0.83 SIR-DD IE 12.54 t = 2.64, p = 0.018* 0.64 F = 0.01, p = 0.934 CW 13.25 t = 2.89, p = 0.012* 0.75 SCI IE 10.21 t = 2.09, p = 0.053 0.51 F = 2.01, p = 0.167 CW 22.56 t = 2.93, p = 0.011* 0.76 CAS IE 9.73 t = 2.39, p = 0.029* 0.58 F = 1.14, p = 0.294 CW 18.07 t = 2.32, p = 0.036* 0.60 CIR IE 12.63 t = 3.64, p = 0.002* 0.88 F = 0.04, p = 0.843 CW 11.63 t = 3.00, p = 0.010* 0.78 IUS IE 4.98 t = 1.10, p = 0.285 0.27 F = 0.69, p = 0.413 CW 9.41 t = 2.96, p = 0.010* 0.76 AAQ-II IE 11.56 t = 1.83, p = 0.087 0.44 F = 1.55, p = 0.222 CW 21.88 t = 3.61, p = 0.003* 0.93Note: Mean % Decrease indicates pre to follow-up symptom decrease by condition, as a percentage of baseline score.
aCalculated using paired t-tests.
*Significant change at p < 0.05.
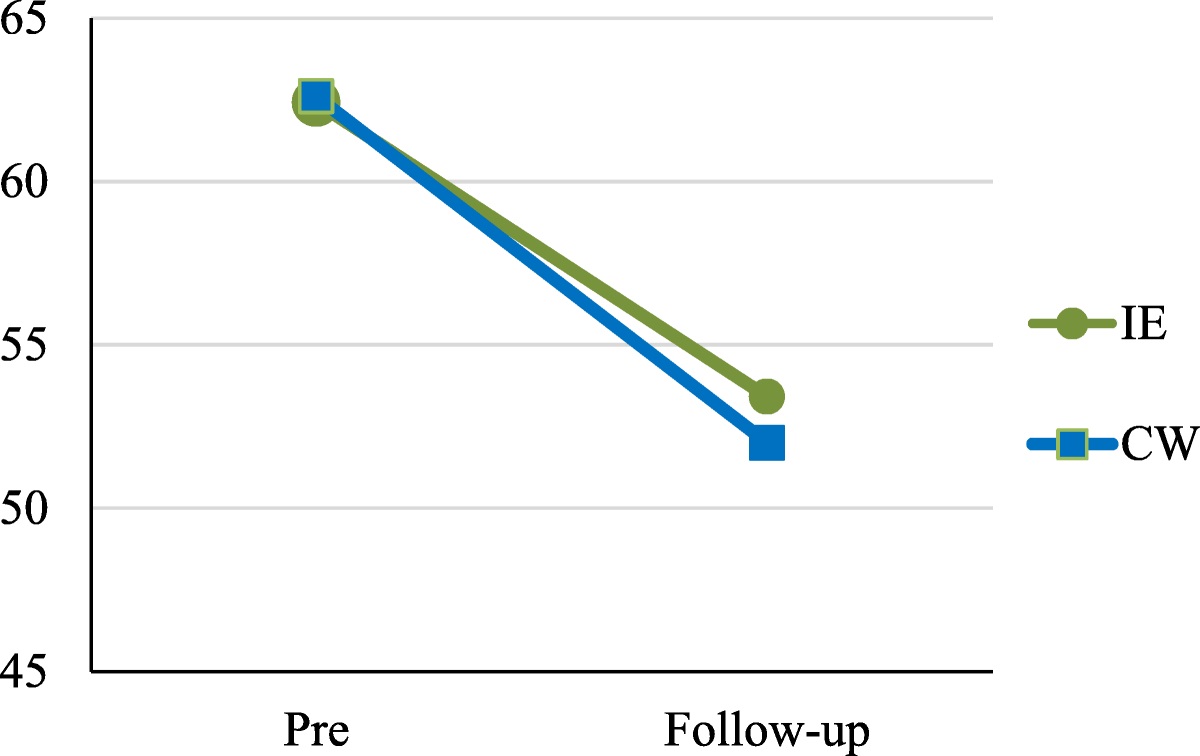
To compare these symptom changes between conditions, we conducted a one-way analysis of covariance to determine if there was a significant difference between conditions (IE vs. CW) on the follow-up score for each measure (e.g., the follow-up SIR score), controlling for the pre score for each measure (e.g., the baseline SIR score). We found that improvements did not significantly differ between the IE condition and the CW condition on any of our measures. These findings are summarized in Table 3 for all measures and for SIR score specifically in Figure 1.
 FIGURE 1:
FIGURE 1: SIR score change from pre to follow-up (IE vs. CW condition).
DISCUSSIONThe present study was a pilot to explore whether IE—a technique that has shown utility in improving worry and anxiety disorders (Deacon and Abramowitz, 2004; Fracalanza et al., 2014)—could be useful in improving HD symptoms and transdiagnostic processes (e.g., avoidance of emotion) in people with HD. A previous case series had found promising results for this approach (Fracalanza et al., 2021). This is the first study to assess IE for HD compared with a CW condition.
We found that, from pre-to-post in the IE condition, there were significant improvements in several HD symptoms and related processes (with medium to large effects); however, the same was true in the CW condition, and when comparing pre-to-post change scores between conditions, improvements were no greater in the IE condition than in the CW condition. Overall, results suggest that although patients in both groups showed symptom improvement, IE worked no better than CW. We discuss the implications of these pilot findings below.
These general improvements in HD symptoms aligned with previous findings on IE for HD (Fracalanza et al., 2021), but results failed to indicate that confronting the mental imagery of discarding—the core fear in people with HD—and its associated emotions reduces difficulties discarding any more than neutral, unrelated writing. This is inconsistent with exposure therapy for anxiety disorders and OCD, which has demonstrated that facing fears—whether in real life (i.e., in vivo exposure) or in the imagination (i.e., IE)—helps improve symptoms associated with that anxiety much more than control approaches (Deacon and Abramowitz, 2004; Foa and McLean, 2016). Surprisingly, IE did not yield significant improvement on intolerance of uncertainty or emotional avoidance, which had been tested as potential mechanisms through which IE might work.
Four interesting possibilities arise from these results. First, the unexpected symptom reduction in the control group may derive from methodological confounds such as regression to the mean, demand characteristics, common factors such as attention from knowledgeable professionals, or expectancy effects (Kazdin, 2003; Price et al., 2008). If so, this serves to reinforce the importance of control groups for methodological rigor.
Second, it could be that the writing itself, separate from its topic, was helpful for HD. Clinical trials testing the efficacy of emotion-related writing interventions for other disorders have sometimes found that CW conditions improve symptoms as much as the experimental intervention (e.g., Baikie et al., 2012; see Qian et al., 2020 for review), and the effects of such interventions are more apparent in studies that included a no writing control condition. This has led previous researchers to suggest that trials include experimental writing, CW, and no writing conditions in order to best capture the effects of an intervention (Qian et al., 2020). The present study's CW could have been particularly likely to yield positive results, as participants writing about a day off may have thought about the things they most enjoy rather than working, which could have elicited positive mood and been briefly therapeutic. Accordingly, future studies may wish to compare IE writing to a no writing control condition.
Third, IE may only be measurably impactful when administered with other approaches, such as within a full course of CBT for HD. Perhaps IE as an augmentation to CBT boosts the potency of the treatment, or perhaps it helps people to engage in in vivo exposures that they would otherwise refuse because it feels too difficult or overwhelming to do. In clinical practice, this is often how IE helps (Moscovitch et al., 2009). IE may also be more effective when verbally administered with a therapist, such as reading aloud a script, and future studies testing its efficacy may wish to use this approach. Indeed, previous researchers have called for the need to test a range of procedural variants to determine which variation of IE yields the greatest impact (Fracalanza et al., 2014), and perhaps the version as delivered in the present study is not “high dose” enough.
Fourth, IE may simply not be helpful for HD symptoms. Decades of research have found it helpful for anxiety and OCD, but its benefits for other disorders are less clear (e.g., eating disorders; Butler and Heimberg, 2020). People with HD may not extract expected benefits from imaginally facing their worst discarding-related fears. Indeed, the relationship between hoarding and anxiety is still unclear, with some research suggesting that neither anxiety sensitivity nor intolerance of uncertainty relate to hoarding symptoms (although they may relate to hoarding-related cognitions; Ayers and Dozier, 2015; Grisham et al., 2018). If anxiety is not a core contributor to the maintenance of HD, then IE approaches—generally used to address disorders of anxiety—may accordingly not be efficacious for HD. However, more testing is needed before determining this.
There were several limitations to this study, some of which may account for the nonsignificant difference between conditions. These include the small sample and the limited “dose” of IE; future studies may wish to recruit larger samples and/or to increase duration of the writing. Future studies may further improve the potency of IE by increasing the “emotional valence” of the writing, for example, by encouraging participants to delve deeper into their emotional experience while writing. This could include practices such as reading the imaginal script aloud repeatedly with a clinician or voice recording the script and then listening to recordings between sessions. In the present study, writing instructions remained consistent across days, but future studies could have participants write about different feared scenarios on different days. It is also noteworthy that this study was conducted entirely remotely and in the context of the global COVID-19 pandemic, and it is unclear how this may have impacted results, as the consequences of engaging remotely versus in-person are unknown.
CONCLUSIONSOverall, people with HD are an underserved population with high rates of dropout and/or refusal from the criterion standard CBT treatment, and thus the exploration of low-investment and low-therapist-intensive interventions for them is of great interest. This study did not find that written IE over 3 days yields greater improvement in HD symptoms than CW does. At the same time, both IE and CW conditions showed significant pre to follow-up changes. Thus, these findings support continued exploration of the utility of novel interventions for HD and the potential of IE, although using a different approach. For example, virtual reality discarding may offer a more immersive approach to make feared discarding scenarios more real, or having a patient do in vivo discarding (e.g., throw out an old cookbook) alongside imaginal writing about a chain of events that culminate in a core fear (e.g., forgetting how to cook) may be more effective than applying either approach separately. Preparing people for in vivo discarding and reengaging people who would otherwise refuse discarding altogether remain important obstacles to tackle.
DISCLOSUREThis study was supported by the National Institute of Mental Health K23MH092434 (Dr. Rodriguez), the Stanford Small Grants Program (Dr. Rodriguez), a NARSAD Young Investigator Award from the Brain and Behavior Research Foundation (Dr. Fracalanza), and a National Institute of Mental Health T32MH019938 (Dr. Raila). Drs. Fracalanza, Raila, and Avanesyan report no additional financial or other relationships relevant to the subject of this article. Dr. Rodriguez has served as a consultant for Allergan, BlackThorn Therapeutics, Rugen Therapeutics, and Epiodyne, and receives research grant support from Biohaven Inc., and a stipend from APA Publishing for her role as Deputy Editor at The American Journal of Psychiatry.
The study was conducted according to acceptable research standards. It received Stanford University School of Medicine institutional review board approval, and informed consent was obtained from all study subjects.
All authors have read and approved the submitted article. A summary of the contribution(s) of each author is as follows: K.F. contributed to the conceptualization, methodology, and writing of original draft. H.R. contributed to the analysis, writing of original draft, and review and editing. T.A. contributed to data collection. C.I.R. contributed to funding acquisition, supervision, and resources.
REFERENCES Abramowitz JS (1996) Variants of exposure and response prevention in the treatment of obsessive-compulsive disorder: A meta-analysis. Behav Ther. 27:583–600. Abramowitz JS (2018) Getting over OCD: A 10-step workbook for taking back your life (2nd ed). New York: Guilford Press. American Psychiatric Association (2013) Obsessive compulsive and related disorders. In Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC. Ayers CR, Dozier ME (2015) Predictors of hoarding severity in older adults with hoarding disorder. Int Psychogeriatr. 27:1147–1156. Baikie KA, Geerligs L, Wilhelm K (2012) Expressive writing and positive writing for participants with mood disorders: An online randomized controlled trial. J Affect Disord. 136:310–319. Berman NC, Hezel DM, Wilhelm S (2021) Is my patient too sad to approach their fear? Depression severity and imaginal exposure outcomes for patients with OCD. J Behav Ther Exp Psychiatry. 70:101615. Berman NC, Wheaton MG, McGrath P, Abramowitz JS (2010) Predicting anxiety: The role of experiential avoidance and anxiety sensitivity. J Anxiety Disord. 24:109–113. Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, Waltz T, Zettle RD (2011) Preliminary psychometric properties of the acceptance and action questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 42:676–688. Buhr K, Dugas MK (2002) The intolerance of uncertainty scale: Psychometric properties of the English version. Behav Res Ther. 40:931–945. Butler RM, Heimberg RG (2020) Exposure therapy for eating disorders: A systematic review. Clin Psychol Rev. 78:101851. Deacon BJ, Abramowitz JS (2004) Cognitive and behavioral treatments for anxiety disorders: A review of meta-analytic findings. J Clin Psychol. 60:429–441. Dugas MJ, Robichaud M (2007) Cognitive-behavioral treatment for generalized anxiety disorder: From science to practice. New York: Routledge. Emmelkamp PM (2004). Behaviour therapy with adults. In Lambert MJ (Ed) Bergin and Garfield's handbook of psychotherapy and behavior change (5th ed, pp 393–446). New York: John Wiley & Sons. First MB, Williams JBW, Karg RS, Spitzer RL (2015) Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV). Arlington, VA: American Psychiatric Association. Foa EB, McLean CP (2016) The efficacy of exposure therapy for anxiety-related disorders and its underlying mechanisms: The case of OCD and PTSD. Annu Rev Clin Psychol. 12:1–28. Foa EB, Steketee G, Turner RM, Fisher SC (1980) Effects of imaginal exposure to feared disasters in obsessive-compulsive checkers. Behav Res Ther. 18:449–455. Fracalanza K, Koerner N, Antony MM (2014) Testing a procedural variant of written imaginal exposure for generalized anxiety disorder. J Anxiety Disord. 28:559–569. Fracalanza K, Raila H, Rodriguez CI (2021) Could written imaginal exposure be helpful for hoarding disorder? A case series. J Obsessive Compuls Relat Disord. 29:100637. Frattaroli J (2006) Experimental disclosure and its m
留言 (0)