
記住我


Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition, characterized by inattention, hyperactivity, and impulsivity (American Psychiatric Association, 2022). Initially conceived as a childhood condition, it is now recognized to affect an estimated 2.58% of adults (Song et al., 2021). Consequences of ADHD are far-reaching and include learning, behavioral and emotional problems, lower occupational status, and relationships difficulties (Doggett, 2004; Faraone et al., 2000). Most adults with ADHD have co-occurring conditions, commonly depression and anxiety (De Graaf et al., 2008), autism spectrum disorder (ASD) (Davis and Kollins, 2012), and various addictions, including behavioral addictions (Starcevic and Khazaal, 2017). Consideration of these co-occurring conditions is critical in managing ADHD.
The most effective treatment is stimulant medication (NICE, 2019), which reduces symptoms in 80% of individuals (Barkley et al., 1991; Dittmann et al., 2014; Milich et al., 2001). However, such treatment is not optimal. Issues include significant adverse effects (Mariani et al., 2007), residual symptoms (Aadil et al., 2017), and low adherence (Ishizuya et al., 2021). As such, there is a drive for alternative approaches, with exercise receiving considerable attention and recommendation in treatment guidelines (NICE, 2019). Although exercise can improve ADHD symptoms (Chang et al., 2012; Dinu et al., 2023; Jensen and Kenny, 2004; Piepmeier et al., 2015), concerns have been raised about exercise dependency and specifically withdrawal being greater in those with ADHD (Popat et al., 2021). Although the concept of exercise dependency or addiction is controversial and it is not classified as a disorder in the current Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) or ICD-11, it has been argued to be an addiction (Berczik et al., 2012), and a measure of exercise dependency can be mapped on the seven factors associated with the substance dependence in DSM-IV, which remain in DSM-5 (Downs et al., 2004; Hausenblas and Downs, 2002). Similarly, research has shown those exhibiting exercise dependency score higher on ADHD symptom scales, even if they have no difference in diagnosis (Colledge et al., 2022). The possibility of ADHD worsening withdrawal has been found for nicotine dependence and is thought to underpin difficulties those with ADHD have in quitting smoking (Bidwell et al., 2017; Sweitzer et al., 2018). However, previous research has been inconsistent as to whether it is the inattentive (IA) or hyperactive-impulsive (HI) symptoms (Ameringer and Leventhal, 2012; Bidwell et al., 2017) that link to withdrawal. Similar effects have not been found for cannabis (Chauchard et al., 2018). Other addictions have yet to be investigated.
Given the recommendations and interest in exercise to manage ADHD, and concerns about withdrawal from exercise, it is pertinent to investigate this further. Therefore, the primary aim of this study is to examine the association between ADHD and exercise dependence, specifically to identify which factors might predict exercise dependence as a whole and as individual symptom domains including withdrawal. Unlike the previous study examining this (Popat et al., 2021), the present study considers the role of three common comorbidities (depression, anxiety, and ASD). In addition, given that exercise dependence is associated with overtraining and injury, we aimed to investigate whether ADHD is associated with the presence of overuse injuries.
METHODS Participants and ProceduresData were collected using an anonymous online survey (February 2022–March 2023). Individuals could participate if they were ≥18 years, resident in the United Kingdom, and had a diagnosis of ADHD, either alone or in combination with depression, anxiety, or ASD. Participants were recruited via advertisements on volunteer sites and social media. Those completing the survey had the option of entering a prize draw for a £50 shopping voucher by providing an email address on completion, which was held separately to their survey data and could not be linked.
Measures Participant CharacteristicsParticipants provided demographic data for gender and age. They completed the 18-item Adult ADHD Self-Report Scale (ASRS) scoring statements from 0 (“never”) to 4 (“very often”) (Kessler et al., 2005). Total (18 items, α = 0.80), inattention (IN; nine items, α = 0.67), and hyperactivity/impulsivity (HI; nine items, α = 0.77) scores were calculated (Das et al., 2012; Hines et al., 2012). In addition, the score for the first six screener items was calculated (α = 0.73) because a score ≥14 on these items is indicative of a diagnosis (Kessler et al., 2005, 2007). Participants were asked to indicate if they were receiving medication and specify type (stimulant, nonstimulant, other) and adherence using a previously adapted scale (Safren et al., 2007). In addition, they were asked to state which, if any, of the three co-occurring conditions they had (depression, anxiety, ASD).
Exercise HabitsParticipants were asked to indicate whether they took part in weekly exercise and, if so, whether this was aerobic, nonaerobic, or a mixture. To assess activity levels, the Godin Leisure-Time Exercise Questionnaire was used (Godin, 2011). This requires participants to indicate how much they engage in strenuous, moderate, and mild exercise over a normal 7-day period. Participants indicate the number of 15-minute periods of exercise for each intensity level they complete within a typical 7-day period. For example, if someone typically runs for 60 minutes per week, they indicate four in the strenuous exercise question. A “leisure score index” or LSI is calculated by summing the weighted values ([9 × strenuous] + [5 × moderate] + [3 × light]), such that a higher score indicates greater levels of activity and participants are categorized as “active” (LSI ≥ 24) or “insufficiently active” (LSI ≤ 23) based on this index (Godin, 2011). For all exercise questions, examples of relevant exercise were given to avoid ambiguity.
Exercise DependencyThe Exercise Dependence Scale (EDS), which operationalizes exercise dependence, has been shown to align with DSM-IV for substance dependence (Downs et al., 2004; Hausenblas and Downs, 2002; Ogden et al., 1997), and continues to align with the current DSM-5 criteria of substance dependence (American Psychiatric Association, 2022), was used. It consists of 21 items rated on a 6-point scale (1 = never, 6 = always). These items are summed to give a total score and divided into seven subscales corresponding to tolerance, withdrawal, intention effect, lack of control, time spent exercising, reduction in other activities, and continuance despite problems. Higher scores indicate greater dependency. There are also established cutoff criteria to distinguish individuals deemed at risk of exercise dependence, symptomatic nondependent, or asymptomatic nondependent (Lindwall and Palmeira, 2009). Cronbach's alpha showed good internal consistency for whole scale (α = 0.94) and subscales (α > 0.69).
Overuse InjuriesOveruse injuries were measured using the OSTRC Overuse Injury Questionnaire (Clarsen et al., 2013), which assesses four impacts of overuse through separate questions: pain, performance reduction, volume reduction, and participation reduction. Questions are related to specific body parts, and we selected foot, ankle, lower leg, knee, upper leg, glutes, torso, arms, shoulder, and neck, allowing us to calculate averages for the upper and lower body score. We also calculated overall scores for the four components (pain, participation, volume, and performance). Participation and pain are measured using a 4-point scale (0 = full participation/no pain, 8 = full participation with problems/mild pain, 17 = reduced participation due to problems in area/moderate pain, 25 = cannot participate due to problems in area/severe pain). Volume and performance are measured using a 5-point scale (0 = no reduction, 6 = to a minor extent, 13 = to a moderate extent, 19 = to a major extent, 25 = cannot participate at all).
Data Processing and AnalysisThe survey was completed by 173 individuals. Several exclusions were made before analysis. First, any participants who omitted answers to a key question were removed (n = 29), leaving 144. Second, and given that we relied on self-report, we used a cutoff score on the ASRS such that only participants scoring ≥14 on the screener items were retained with any below that being excluded (n = 18). This resulted in a final sample size of 126 participants. The sample was characterized using demographic, clinical, and exercise measures using frequency counts (categorical variables) and means (continuous variables). To establish which factors predicted exercise dependence, separate linear regressions were used to predict the total EDS score and the scores of individual subscales corresponding to components of dependence. In each case, a blocked regression was adopted with block 1 containing demographic variables (age/gender), block 2 adding LSI for activity level, and block 3 adding clinical measures (ASRS-IA, ASRS-HI, medication use, depression, anxiety, and ASD). Given the small number of participants in some gender categories, only those identifying as male or female were included, giving a sample size of 114. The same approach was used to establish which factors predicted overuse injuries with separate regressions run for lower body, upper body, pain, performance, participation, and volume. No prior study exists to estimate effect size for these analyses. However, previous work reported an effect size of d = 0.44 for increased withdrawal in ADHD (Popat et al., 2021), and as such, we estimated sample size based on a medium effect size. A priori power calculations indicated that a sample size of 113 would be required to identify a medium effect in these analyses (f = 0.15, power = 0.80, α = 0.05).
RESULTS Demographic and Clinical TraitsMost participants identified as female (n = 94, 74.6%), followed by male (n = 20, 15.9%), nonbinary (n = 10, 7.9%), or preferred not to say (n = 2, 1.6%). The average age was 29.21 ± 8.20 (mean ± SD) years. The total ASRS score was 55.07 ± 8.09 (mean ± SD) with similar ASRS-IN (30.05 ± 5.71) and ASRS-HI (25.02 ± 5.71) scores. All ASRS measures were correlated (total vs. IN r = 0.770, p < 0.001; total vs. HI r = 0.906, p < 0.001; IN vs. HI r = 0.429, p < 0.001). Seventy-eight individuals (61.9%) were taking medication, with 72 (57.1%) taking stimulants and two (1.6%) taking nonstimulants, one taking a combination (0.8%), two not specifying (1.6%), and one taking an antidepressant (0.8%). Adherence information was provided by 64 participants and was 82.0% on average. Sixty-five (52%) participants reported having anxiety, 21 (17%) had ASD, and 39 (31%) had depression. Only 44 (34.9%) reported having ADHD alone, although 45 (35.7%) reported having a single co-occurring condition, 31 (24.6%) reported two co-occurring conditions, and six (4.8%) reported having all three of the co-occurring conditions listed.
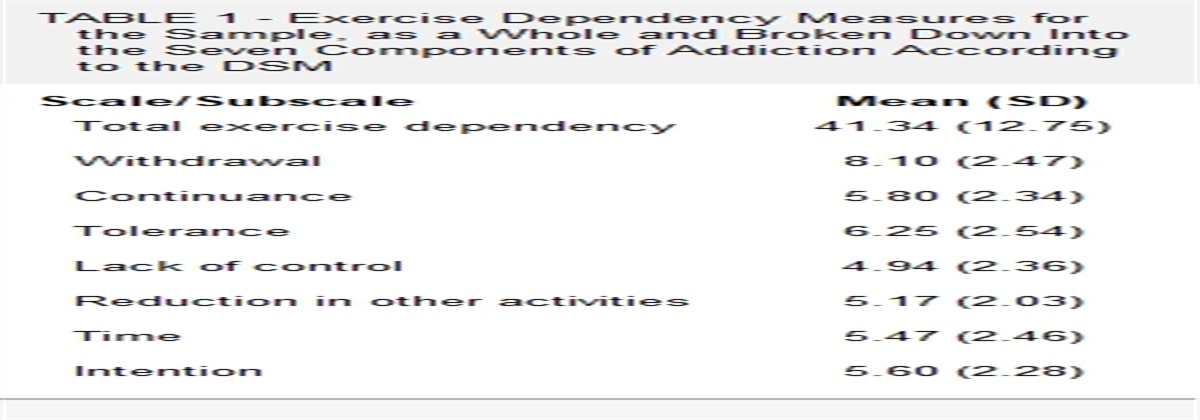
Exercise Habits and DependencyParticipant responses showed that the majority (n = 112, 88.9%) undertook weekly exercise. Of these, 41 (36.6%) engaged in aerobic activity, eight (7.1%) in nonaerobic activity, and the remainder (n = 63, 56.3%) completing a combination. All except two participants reported typical exercise intensity for their most common type of weekly exercise, with 50 (45.5%) reporting high intensity exercise, 54 (49.1%) indicating moderate intensity, and just six (5.5%) reporting low intensity. Perhaps unsurprisingly given this, most participants (n = 95, 75.4%) were classed as active using the LSI, and only 31 (24.6%) were insufficiently active. Table 1 provides the mean score for the EDS total and subscales. Using the previously described method, participants were categorized into different levels of risk (Lindwall and Palmeira, 2009). There were no dependent individuals, but 49 (38.9%) were deemed symptomatic nondependent, and 77 (61.1%) were asymptomatic nondependent.
TABLE 1 - Exercise Dependency Measures for the Sample, as a Whole and Broken Down Into the Seven Components of Addiction According to the DSM Scale/Subscale Mean (SD) Total exercise dependency 41.34 (12.75) Withdrawal 8.10 (2.47) Continuance 5.80 (2.34) Tolerance 6.25 (2.54) Lack of control 4.94 (2.36) Reduction in other activities 5.17 (2.03) Time 5.47 (2.46) Intention 5.60 (2.28)Regression analysis for the overall EDS score found that demographic variables alone (block 1) did not significantly predict exercise dependency, F(2,111) = 0.152, p = 0.859, but adding LSI (block 2) did result in a significant model, F(3,110) = 5.087, p = 0.002, which was not improved further by the addition of clinical measures (block 3), F(9,104) = 2.318, p = 0.020. The final model predicted 16.7% of the variance, with the only significant predictor of exercise dependency being the LSI, that is, activity level, which was a positive predictor (Table 2). A similar pattern of results was found for withdrawal with the final model accounting for 19.5% of the variance, F(9,104) = 2.795, p = 0.006, but here both LSI and ASRS-HI were significant positive predictors. For tolerance, the same pattern was found, with the final model accounting for 20.8% of the variance, F(9,104) = 3.026, p = 0.003, although LSI was the only significant predictor again. This was also the case for time, F(9,104) = 2.29, p = 0.022, with 16.5%. For intention, only the second model was significant (blocks 1 and 2), accounting for just 9.4% of the variance, F(3,110) = 3.811, p = 0.012, with LSI as the only significant predictor. No models were significant for continuance, lack of control, or reduction in other activities.
TABLE 2 - Coefficients of Significant Predictors for Different Components of Exercise Dependency Independent Variable Significant Predictors R 2 b β t (p) Exercise dependency 0.167 LSI 9.828 0.341 3.671 (<0.001) Withdrawal 0.195 LSI 1.828 0.338 3.702 (<0.001) ASRS-HI 0.096 0.222 2.200 (0.030) Tolerance 0.208 LSI 2.536 0.527 4.814 (<0.001) Time 0.165 LSI 1.861 0.510 3.652 (<0.001) Intention 0.094 LSI 1.549 0.507 3.054 (<0.001)Descriptive statistics for overuse measures are shown in Table 3. For upper body scores, linear regression revealed that all three models significantly predicted overuse injury with the final model accounting for 43.3% of the variance, F(9,104) = 2.663, p = 0.008. Table 4 shows that the significant predictors were age and ASD. A similar pattern was found for lower body scores, with the final model accounting for 38.4% of the variance, F(9,104) = 2.005, p = 0.046. Examination of the different components revealed slight variation on this pattern. Pain was not significantly predicted by models including only demographic (block 1) or demographic and exercise (block 2) variables but was significantly predicted when clinical variables were introduced, F(9,104) = 2.386, p = 0.017, although in the final model, both age and ASD were significant predictors. For performance, models at all three stages were significant, with the final model accounting for 15.9% of the variance, F(9,104) = 2.190, p = 0.028, with age and ASD are significant predictors. The same pattern was found for training volume with 40.1% of the variance accounted for, F(9,104) = 2.219, p = 0.026, and for participation, with the final model accounting for 18.6% of the variance, F(9,104, 2.641, p = 0.009). In summary, increasing age and the presence of ASD, but not any ADHD symptoms, are also associated with greater injury.
TABLE 3 - Overuse Injury Measures From the OSTRC Survey for the Sample Scale/Subscale Mean (SD) Upper body 6.50 (10.19) Lower body 5.99 (9.43) Participation 1.88 (3.22) Volume 1.28 (3.09) Performance 1.22 (0.53) Pain 1.83 (2.93)The primary aim of this research was to examine the association between ADHD and exercise dependency. Our data revealed that most respondents were physically active. No participants met the criteria for exercise dependence. This is not unexpected given that estimates of dependence are as low as 3% (Orhan et al., 2019). However, we did find that approximately 40% were classed as symptomatic nondependent, that is, the next level of risk. This is slightly lower than previously found for ADHD, which reported 54.2% (Popat et al., 2021), but nonetheless indicates that a significant proportion above the lowest risk level (nonsymptomatic, nondependent). Our analyses revealed, unsurprisingly, that activity level was a significant positive predictor of exercise dependency as a whole and of four of the seven DSM-IV criteria for substance dependence on which the EDS is modeled and persist in DSM-5: withdrawal, tolerance, time spent on use, and intention effect. Critically, ASRS-HI was also a positive predictor of withdrawal. This is consistent with previous work which showed that some individuals with ADHD have higher levels of withdrawal than those without the condition (Popat et al., 2021). It also aligns with other work that has indicated that HI symptoms are positively correlated with nicotine withdrawal in healthy individuals (Bidwell et al., 2017) and that, in those with ADHD, it is HI symptoms, not IA symptoms, that predict substance misuse (Elkins et al., 2007) and uptake of smoking (Fuemmeler et al., 2007). Collectively, these results suggest that the heightened withdrawal and risk of dependency related to HI symptoms in ADHD is not specific to nicotine and may also occur in exercise dependency.
The second aim of this research was to consider whether ADHD measures predict overuse injury, which might be expected if those individuals show greater signs of dependency. The results revealed that age was a significant predictor of all overuse measures. Much of the research to date on overuse injuries has focused on young or professional athletes who have therefore resulted in a relatively limited age range. However, one study that included a broader population did identify age as a risk factor (Trone et al., 2014) aligning with the current findings. Interestingly, there was no link between ADHD symptoms and overuse injury, but the presence of ASD was a significant positive predictor. The exact reasons for this are not clear. From the design of the current study, we cannot be certain whether the risk is associated with ASD per se or ASD when co-occurring with ADHD. Irrespective of this there are several reasons this might arise. For example, the greater risk could be associated with motor difficulties in ASD including weak neuromuscular interaction (Nadeem et al., 2021) or the restricted and repeated behaviors that can arise (Nekar et al., 2022), which may increase the risk of overuse injury. Recent research has indicated that individuals with ASD also often show symptoms of hypermobility (Nisticò et al., 2022), although it is unclear that being hypermobile increases risk of overuse injury (De Smet et al., 1998; Junge et al., 2015). Given the high co-occurrence of ASD and ADHD, it is important to investigate any links with overuse injury further before recommending exercise as a management strategy in ADHD.
This work should be interpreted in line with its strengths and limitations. Although the data were collected using an anonymous online survey, which would encourage honesty, participants self-reported their ADHD diagnosis, albeit in a way that we could confirm with an established screening survey (Kessler et al., 2005, 2007). However, we did not verify their diagnosis of ADHD, or any comorbidities, with a structured clinical interview, which can be seen as a limitation. Despite this, it should be noted that the final sample had the characteristics of an ecologically valid group of the population with ADHD, evidenced through inclusion of those with common comorbidities at similar rates to be expected in the general population with ADHD (Davis and Kollins, 2012; De Graaf et al., 2008) and adherence at rates typical of individuals with ADHD who take medication (Safren et al., 2007). Although the sample was restricted to those residing in the United Kingdom and female dominated, it does exceed the required size to obtain adequate power; as per our power calculations, the latter could be considered a strength given the male-dominated research in ADHD (Dinu et al., 2022). It is noteworthy that over 80% of our sample undertook weekly exercise, which is higher than typically reported for the general population (Sport England, 2022). This could be indicative of self-selection bias, or it could reflect the fact that those with ADHD may be more physical activity than those without (Weissenberger et al., 2018). In addition, although we relied on self-report, which could be considered a limitation, previous research has suggested that this can be reliable if answers are known to individuals and questions are unambiguous and relate to recent activities, require a thoughtful response, and will not lead to undesirable disclosures (Kuh, 2001; Owston et al., 2011). Finally, given the anonymous survey data collection, it is possible that individuals could have completed the survey multiple times. Examination of the data indicates that this was not the case, but future studies should use different techniques to avoid this.
CONCLUSIONSGiven the need for alternative interventions in ADHD, and the potential of exercise to be used, it is critical that we fully understand any associated risks. The current study adds to the mounting evidence that individuals with ADHD may experience greater withdrawal from exercise than those without and suggests that it is the HI symptoms that are central to this. In addition, the presence of ASD was associated with overuse injury. The exact reasons for this are unclear but warrant further investigation.
DISCLOSUREAll authors have read and approved this article for submission. All authors contributed to the conceptualization of the study. A.V.R. and E.J.D. conducted analyses. All authors contributed to interpretation of findings and the initial draft with E.J.D. revising the draft for submission. All authors consent to be held accountable.
No funding was received for this research.
This study was approved by the Institutional Ethics Committee (LRU.DP-21.22-27186) of King's College London.
All data are available on reasonable request to the corresponding author.
The authors declare no conflicts of interest.
REFERENCES Aadil M, Cosme RM, Chernaik J (2017) Mindfulness-based cognitive behavioral therapy as an adjunct treatment of attention deficit hyperactivity disorder in young adults: A literature review. Cureus. 9:e1269. American Psychiatric Association (2022) Diagnostic and statistical manual of mental disorders (5th ed, text revision ed). Washington, DC: American Psychiatric Association. https://doi.org/https://doi.org/10.1176/appi.books.9780890425787. Ameringer KJ, Leventhal AM (2012) Symptom dimensions of attention deficit hyperactivity disorder and nicotine withdrawal symptoms. J Addict Dis. 31:363–375. Barkley RA, DuPaul GJ, McMurray MB (1991) Attention deficit disorder with and without hyperactivity: Clinical response to three dose levels of methylphenidate. Pediatrics. 87:519–531. Berczik K, Szabó A, Griffiths MD, Kurimay T, Kun B, Urbán R, Demetrovics Z (2012) Exercise addiction: Symptoms, diagnosis, epidemiology, and etiology. Subst Use Misuse. 47:403–417. Bidwell LC, Karoly HC, Hutchison KE, Bryan AD (2017) ADHD symptoms impact smoking outcomes and withdrawal in response to varenicline treatment for smoking cessation. Drug Alcohol Depend. 179:18–24. Chang YK, Liu S, Yu HH, Lee YH (2012) Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch Clin Neuropsychol. 27:225–237. Chauchard E, Hartwell KJ, McRae-Clark AL, Sherman BJ, Gorelick DA (2018) Cannabis withdrawal in adults with attention-deficit/hyperactivity disorder. Prim Care Companion CNS Disord. 20:26738. Clarsen B, Myklebust G, Bahr R (2013) Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. Br J Sports Med. 47:495–502. Colledge F, Buchner U, Schmidt A, Wiesbeck G, Lang U, Pühse U, Gerber M, Walter M (2022) Individuals at risk of exercise addiction have higher scores for depression, ADHD, and childhood trauma [original research]. Front Sports Act Living. 3:761844. Das D, Cherbuin N, Butterworth P, Anstey KJ, Easteal S (2012) A population-based study of attention deficit/hyperactivity disorder symptoms and associated impairment in middle-aged adults. PloS One. 7:e31500. Davis NO, Kollins SH (2012) Treatment for co-occurring attention deficit/hyperactivity disorder and autism spectrum disorder. Neurotherapeutics. 9:518–530. De Graaf R, Kessler RC, Fayyad J, ten Have M, Alonso J, Angermeyer M, Borges G, Demyttenaere K, Gasquet I, de Girolamo G (2008) The prevalence and effects of adult attention-deficit/hyperactivity disorder (ADHD) on the performance of workers: Results from the WHO world mental health survey initiative. Occup Environ Med. 65:835–842. De Smet L, Ghyselen H, Lysens R (1998) Incidence of overuse syndromes of the upper limb in young pianists and its correlation with hand size, hypermobility and playing habits. Chir Main. 17:309–313. Dinu LM, Phattharakulnij N, Dommett EJ (2022) Tryptophan modulation in individuals with attention deficit hyperactivity disorder: A systematic review. J Neural Transm. 129:361–377. Dinu LM, Singh SN, Baker NS, Georgescu AL, Singer BF, Overton PG, Dommett EJ (2023) The effects of different exercise approaches on attention deficit hyperactivity disorder in adults: A randomised controlled trial. Behav Sci (Basel). 13:129. Dittmann RW, Cardo E, Nagy P, Anderson CS, Adeyi B, Caballero B, Hodgkins P, Civil R, Coghill DR (2014) Treatment response and remission in a double-blind, randomized, head-to-head study of lisdexamfetamine dimesylate and atomoxetine in children and adolescents with attention-deficit hyperactivity disorder. CNS Drugs. 28:1059–1069. Doggett AM (2004) ADHD and drug therapy: Is it still a valid treatment? J Child Health Care. 8:69–81. Downs DS, Hausenblas HA, Nigg CR (2004) Factorial validity and psychometric examination of the exercise dependence scale-revised. Meas Phys Educ Exerc Sci. 8:183–201. Elkins IJ, McGue M, Iacono WG (2007) Prospective effects of attention-deficit/hyperactivity disorder, conduct disorder, and sex on adolescent substance use and abuse. Arch Gen Psychiatry. 64:1145–1152. Faraone SV, Biederman J, Spencer T, Wilens T, Seidman LJ, Mick E, Doyle AE (2000) Attention-deficit/hyperactivity disorder in adults: An overview. Biol Psychiatry. 48:9–20. Fuemmeler BF, Kollins SH, McClernon FJ (2007) Attention deficit hyperactivity disorder symptoms predict nicotine dependence and progression to regular smoking from adolescence to young adulthood. J Pediatr Psychol. 32:1203–1213. Godin G (2011) The Godin-Shephard leisure-time physical activity questionnaire. Health Fitness J Canada. 4:18–22. Hausenblas HA, Downs DS (2002) Exercise dependence: A systematic review. Psychol Sport Exerc. 3:89–123. Hines JL, King TS, Curry WJ (2012) The Adult ADHD Self-Report Scale for screening for adult attention deficit-hyperactivity disorder (ADHD). J Am Board Fam Med. 25:847–853. Ishizuya A, Enomoto M, Tachimori H, Takahashi H, Sugihara G, Kitamura S, Mishima K (2021) Risk factors for low adherence to methylphenidate treatment in pediatric patients with attention-deficit/hyperactivity disorder. Sci Rep. 11:1707. Jensen PS, Kenny DT (2004) The effects of yoga on the attention and behavior of boys with attention-deficit/hyperactivity disorder (ADHD). J Atten Disord. 7:205–216. Junge T, Larsen LR, Juul-Kristensen B, Wedderkopp N (2015) The extent and risk of knee injuries in children aged 9-14 with generalised joint hypermobility and knee joint hypermobility—The CHAMPS-study Denmark. BMC Musculoskelet Disord. 16:143. Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, Howes MJ, Jin R, Secnik K, Spencer T (2005) The World Health Organization Adult ADHD Self-Report Scale (ASRS): A short screening scale for use in the general population. Psychol Med. 35:245–256. Kessler RC, Adler LA, Gruber MJ, Sarawate CA, Spencer T, Van Brunt DL (2007) Validity of the World Health Organization Adult ADHD Self-Report Scale (ASRS) screener in a representative sample of health plan members. Int J Methods Psychiatr Res. 16:52–65. Kuh GD (2001) The National Survey of Student Engagement: Conceptual framework and overview of psychometric properties. Lindwall M, Palmeira A (2009) Factorial validity and invariance testing of the exercise dependence scale-revised in Swedish and Portuguese exercisers. Meas Phys Educ Exerc Sci. 13:166–179. Mariani JJ, Mariani JJ, Levin FR (2007) Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addictions. 16(sup1):45–56. Milich R, Balentine AC, Lynam DR (2001) ADHD combined type and ADHD predominantly inattentive type are distinct and unrelated disorders. Clin Psychol. 8:463–488. Nadeem MS, Murtaza BN, Al-Ghamdi MA, Ali A, Zamzami MA, Khan JA, Ahmad A, Rehman MU, Kazmi I (2021) Autism—A comprehensive array of prominent signs and symptoms. Curr Pharm Des. 27:1418–1433. Nekar DM, Lee DY, Hong JH, Kim JS, Kim SG, Seo YG, Yu JH (2022) Effects of augmented reality game-based cognitive-motor training on restricted and repetitive behaviors and executive function in patients with autism spectrum disorder. Healthcare (Basel). 10: NICE (2019) Diagnosis and management of ADHD in children, young people and adults. Available at: https://www.nice.org.uk/guidance/ng87/chapter/Recommendations#managing-adhd. Accessed March 1, 2023. Nisticò V, Iacono A, Goeta D, Tedesco R, Giordano B, Faggioli R, Priori A, Gambini O, Demartini B (2022) Hypermobile spectrum disorders symptoms in patients with functional neurological disorders and autism spectrum disorders: A
留言 (0)