
記住我



Optimised usual care was developed based on a) findings from the programme development grant and early work packages [21], exploring variations in NHS prostate cancer care pathways and exercise provision for men on ADT and b) from the SHU research teams’ experience of providing written guidance for control groups in cancer and lifestyle research [34].
Intervention description Optimised usual care (OUC)All participants will receive OUC (including SLI participants). OUC includes endorsement of the NICE guidelines around the benefits of exercise for men on ADT and behavioural support (where appropriate) from key workers during routine clinic appointments. Consenting participants will then undergo a ‘safety to exercise’ check administered over the phone by researchers at Sheffield Hallam University, with support from clinical teams, principal investigators, and the chief investigator where clinical queries arise. Participants will be sent an information pack through the post including a booklet about the NICE guidelines for people on ADT and local and nationally available resources related to lifestyle (e.g. information materials from Prostate Cancer UK (PCUK) [35], Macmillan [36], Cancer Research UK (CRUK) [37]).
The healthcare professional interventionNHS prostate cancer clinical teams will receive a behaviorally informed, bespoke training package and continuous intervention support during recruitment to the STAMINA trial (see Additional file 1) [24]. Training will last up to 3 h and will be delivered face-to-face or remotely depending on local policy and preference. The first training session will be delivered during site set-up and will be centred on four R’s: Recognizing who is suitable for the STAMINA trial, Recommending exercise in line with NICE guidance, Referral to the STAMINA trial and Recording research related information on the ADT log. Follow-up training will be delivered at 6–12 weeks following initiation of recruitment and will focus on supporting lifestyle behaviour change during routine clinic follow-up appointments. In parallel, ad hoc intervention support will be offered and regular feedback on referral performance will be provided via email. Full details of intervention development have been published [24].
The STAMINA lifestyle intervention (SLI)SLI was developed in line with two overarching principles: (1) SLI will be offered as an intrinsic part of a man’s cancer care as opposed to an ‘add-on’ and (2) the intervention will be designed in a way to maximise both efficacy (likelihood of change) and effectiveness (accessibility and generalisability beyond urban areas).
SLI is a behaviourally informed, lifestyle intervention embedded into prostate cancer care to support delivery of NICE (NG131 1.4.19) guidance for people with prostate cancer on ADT (see Additional file 1). The SLI is focussed on supervised exercise training (primarily face-to-face) combining resistance and aerobic exercise with application of the behavioural skills learnt to other patient-negotiated lifestyle goals, including dietary modification. The SLI will be delivered in partnership with NH, a community-based, appropriately trained exercise provider, and will only be available to participants randomised to the intervention arm for 12 months.
SLI participants will be invited to an induction to exercise with a CES to explore their capability, opportunity, and motivation to exercise twice a week for 12 months. The supervised exercise sessions will include both aerobic (30–45 min) and resistance (up to 4 sets, 8–12 reps of major muscle groups) components as recommended by NICE (NG131 1.4.19 [19]) and in accordance with exercise programmes previously shown to be beneficial and safe to men on ADT (e.g. Bourke et al., 2014 [16]). The supervised exercise programme will be tailored to address individual requirements and will be delivered twice weekly for the first 12 weeks, initially one-to-one before transition to small groups (based on satisfactory progress). For the remaining 9 months of the programme, negotiated supervision will be offered (i.e. once a month maximum, once every 3 months minimum).
In parallel to supervised exercise sessions, behaviour change support will be delivered during programme reviews and catch-up calls between the CES and participant, and by completion of a behaviourally informed STAMINA diary. Programme reviews will be scheduled at 12 weeks, 6 months and 12 months following the induction session and will include a review of participant progress and a written summary report. Summary reports will be sent to the referring clinical team via email as part of the feedback loop and for discussion with the participant at their next routine clinic appointment. Catch-ups (face-to-face or over the phone) will also be organised with the CES and participant every 6 weeks to explore participant progress and address any barriers to intervention adherence (where applicable).
During the 12-month intervention period, SLI participants will be provided with a complimentary NH gym membership to support additional, independent exercise behaviour. SLI participants will also be offered one reduced price membership (~ 50%) for a family member to further support their exercise behaviour by addressing social support.
The exercise professional interventionCommunity-based CESs and gym management/operational/front-of-house staff will receive a behaviourally informed, role-specific, bespoke training package with ongoing intervention support during delivery of the SLI (see Additional file 1). Level 1 training will comprise three online modules providing high-level information about prostate cancer, the SLI, patient confidentiality and operational procedures. All management, operational, sales, fitness and front-of-house staff will be invited to complete the online modules with a mandatory 80% pass mark. Staff responsible for the delivery of SLI (i.e. fitness managers, rehab specialists and personal trainers) will be invited to level 2 training which targets knowledge, confidence and skill related to delivering supervised exercise and behavioural support to men with prostate cancer. Level 2 training will be delivered face-to-face on site at NH over one full day. Ongoing tapered intervention support will be offered in the form of a weekly telephone call for up to 4 weeks followed by a monthly meeting with all CESs involved in the delivery of SLI. Full details of intervention development have been published [38].
Criteria for discontinuing or modifying allocated interventionsThe risks of the supervised exercise programme in men on ADT are minimal, with no increase in the risk of serious adverse events reported in a systematic review of RCTs evaluating the delivery of such programmes in these men [22]. All recruited men will continue to be under the care of their treating cancer clinician, who will be aware of their participation in the trial. In line with standard clinical care, cessation of the SLI at any time will be at the discretion of the clinicians or the participants themselves. Pauses to the programme will be accommodated for health-related reasons, holidays (up to 2 weeks maximum) and modification will be considered for individual cases (e.g. to remote sessions).
Strategies to improve adherence to interventionsIntervention adherence will be monitored weekly by the research team at SHU by reviewing SLI participants’ attendance at supervised exercise sessions, to identify those who have dipped below 75% attendance. CESs at each NH site will upload data relating to attendance and completion of aerobic and resistance exercise components of the SLI after each session using a REDCap web-based reporting software. Researchers will download, compile, and clean the data on a weekly basis. The database will track adherence relative to the number of prescribed sessions to date and produce “alerts” once a SLI participant drops below 75% adherence. This alert with suggested actions will be sent onto the NH fitness manager who will identify and deliver behavioural support in line with the COM-B [30] model of behaviour change (i.e. data verification, identify required behavioural support and deliver behavioural support). If a participant’s attendance remains below 75%, a maximum two further alerts are sent. A record of all alerts sent and subsequent actions will be maintained.
Relevant concomitant care permitted or prohibited during the trialThe protocol does not restrict participant access to usual care services. The usual care delivered at each site is documented at the point of site inclusion in the trial, at 12 months after the site opening and at 12 months after the last participant at the site is recruited. Participants also self-report their usual care received at 3-, 6- and 12-month post-randomisation. Should the trial team become aware of any new referrals to services, the nature of the referral will be established and discontinuation in the SLI considered.
Provisions for post-trial careShould participants disclose anything to the trial team which puts them or anyone else at risk, the trial team may feel it necessary to report this to the appropriate persons. Additional exercise support outside of the SLI is not provided by CESs, and no specific aftercare is planned as part of the trial.
The NHS Sponsor is a member of the Clinical Negligence Scheme for Trusts (CNST) which provides indemnity cover for clinical negligent harm only. The Sponsor has an agreement in place with NH and therefore CNST indemnity extends to cover this service provider and their staff who have a duty of care to research participants.
OutcomesOutcome data will be collected via participant self-report postal/online questionnaires and follow-up assessments with a local research nurse, or delegate, at 3-, 6- and 12-month post-randomisation. Supported completion of questionnaires by site staff can be requested by participants. If supported follow-up is required, wherever possible a research nurse, or delegate, who is blind to the participant’s allocation will offer telephone follow-up to participants who are unable to complete assessments independently. If site staff are subsequently unblinded, additional and subsequent data collection will be completed by an alternative researcher who is blinded to allocation.
Primary outcomesDisease-specific QoL and fatigue at 12-month post-randomisation were measured by FACT-P [26] and FACIT-F [27]. The FACT-P [26] incorporates primary QOL domains: Physical Well-Being, Social/Family Well-Being, Emotional Well-Being, and Functional Well-Being with the addition of a prostate cancer-specific subscale. The FACIT-F [27] assesses perceptions of fatigue over the last 7 days.
Secondary outcomesSecondary endpoints will be measured at 3-, 6- and 12-month post-randomisation and are as follows:
Questionnaire outcomesPhysical, Social/Family, Emotional and Function wellbeing, assessed using FACT-P [26] subdomains
Cancer-specific fatigue (FACIT-F [27].)
Leisure time physical activity assessed using the Godin [28] questionnaire.
Fear of recurrence and psychological distress markers assessed using FCR4 [29] and FCR7 [29].
Adverse effects of ADT assessed using trial specific ADT Symptom Index.
Perceptions of capabilities, opportunities and motivations to perform a target behaviour assessed by the COM-B [30] Questionnaire.
Physical measuresFunctional capacity and body composition assessed by blood pressure, chair sit-to-stand, waist and hip circumference and weight.
Safety Health economicsGeneric quality of life assessed using EQ-5D-5L [31] questionnaire
Costs of the intervention and of health care resource use
Cost per incremental QALY using EQ-5D-5L [31] questionnaire
Patient preferences and willingness to pay for exercise programmes as assessed by the DCE [32].
Moderator/mediatorsModerator and mediator variables which influence engagement with and benefit from the intervention will also be measured.
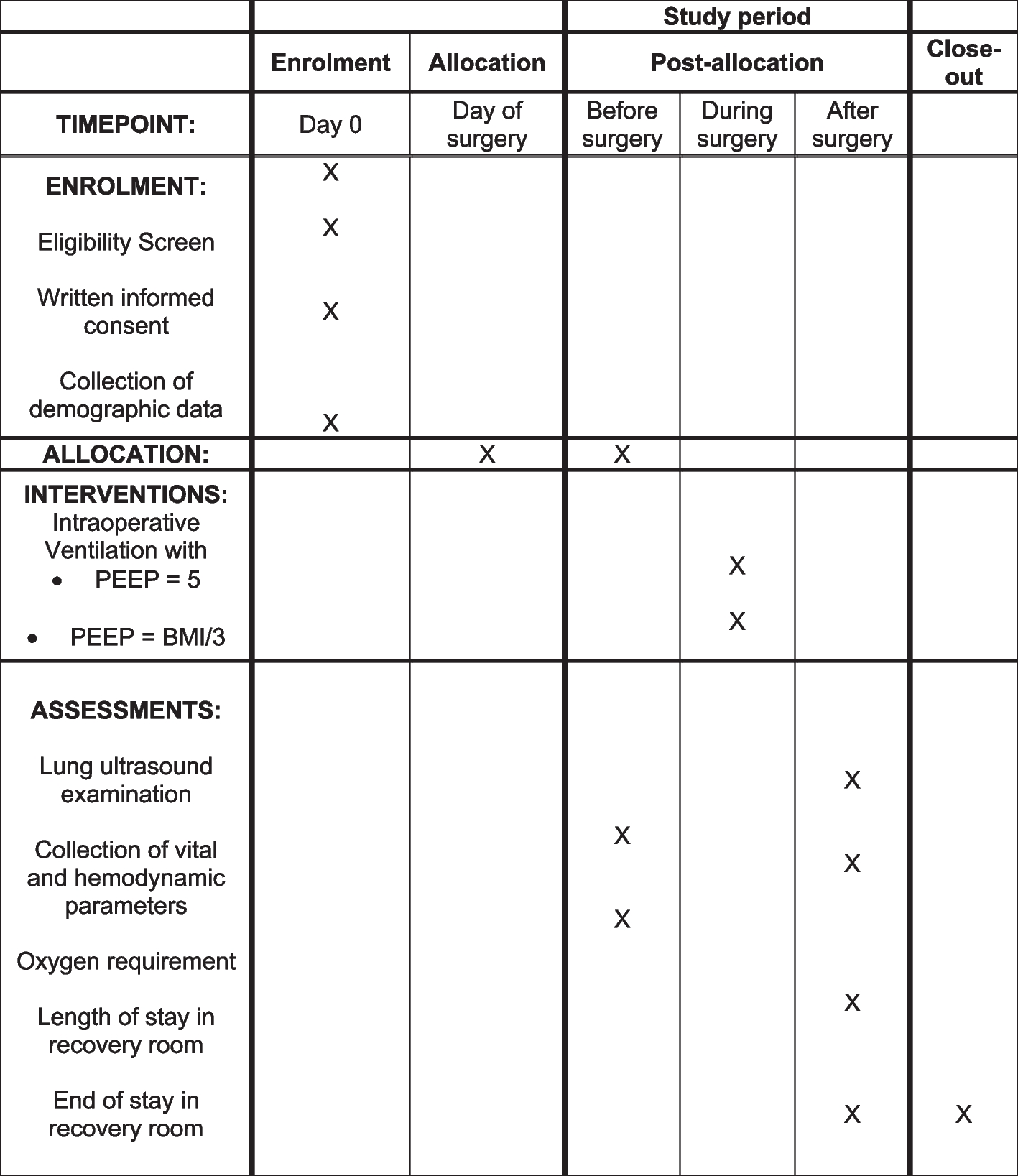
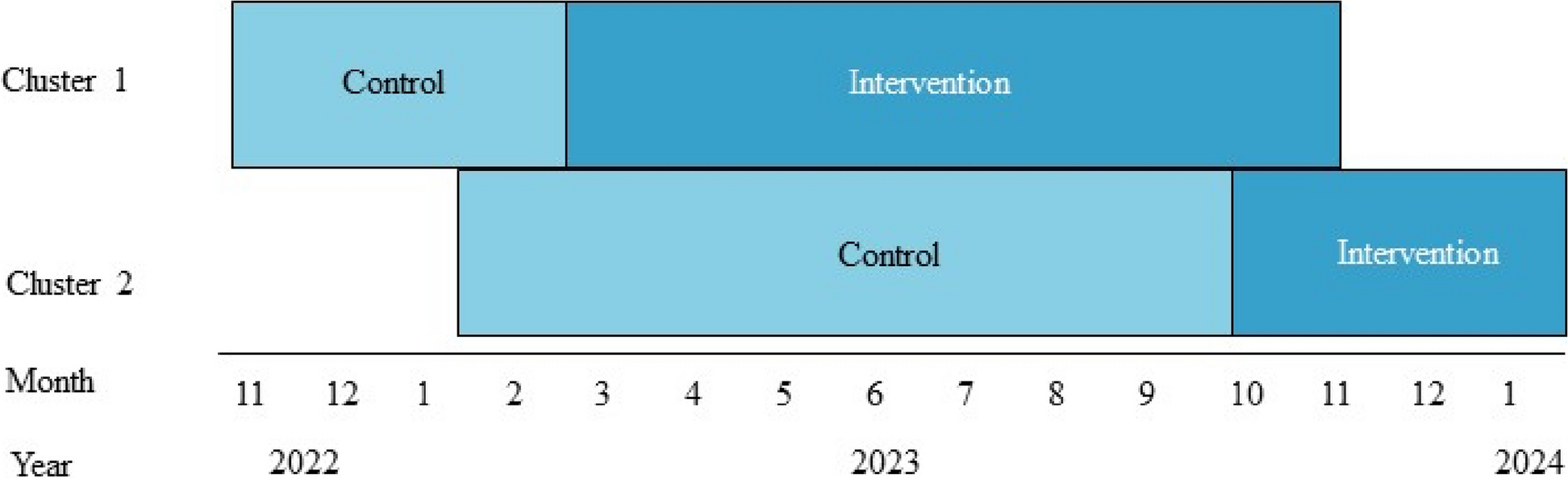
Participant timelineThe trial timeline for participants is presented in Fig. 1, outlining the schedule of enrolment and interventions, and in Fig. 2, outlining the schedule of assessments.
Fig. 1
Schedule of enrolment and interventions
Fig. 2 Sample size
Sample size A total sample size of 697 men (313 OUC, 384 SLI) is required to provide 90% power to detect a small to moderate effect size of either 0.33 in FACT-P [26] (8 point difference) or 0.35 in FACIT-F [27] (3 point difference) at the 5% significance level. Calculations assume a maximum standard deviation of 24 (FACT-P [26]) and 8.6 (FACIT-F [27]) and 30% loss to follow-up by 12 months [38]. Clustering at the level of the CES in the intervention arm is accounted for using an intracluster correlation coefficient (ICC) of 0.05 [39], a coefficient of variation of 0.6 to account for variation in the number of men each CES will deliver the intervention to, an average cluster size of 6 participants (range 1 to 14) per CES and 64 CES.
The sample size calculation takes into account the correlation between the two primary endpoints based on methodology by Micheaux et al. [40]. A correlation between FACT-P [26] and FACIT-F [27] of 0.7 (95% confidence internal (CI): 0.58–0.78) was observed at baseline in the pilot data [16]. The lower bound of the CI for the correlation estimate (0.58) was incorporated into the calculations. After accounting for multiple testing with correlated continuous multiple primary endpoints, the adjusted alpha level is 0.02768.
RecruitmentTo ensure recruitment of 697 men within an 18-month period, the internal pilot green progression criteria for recruitment was set as at least 4 men per site per month from a minimum of 12 NHS Trusts based on a minimum of 40 men from each site, per year, over a total recruitment period of 18 months. Additional sites will be added during the recruitment period to deliver the overall sample size of 697 if required.
留言 (0)