
記住我
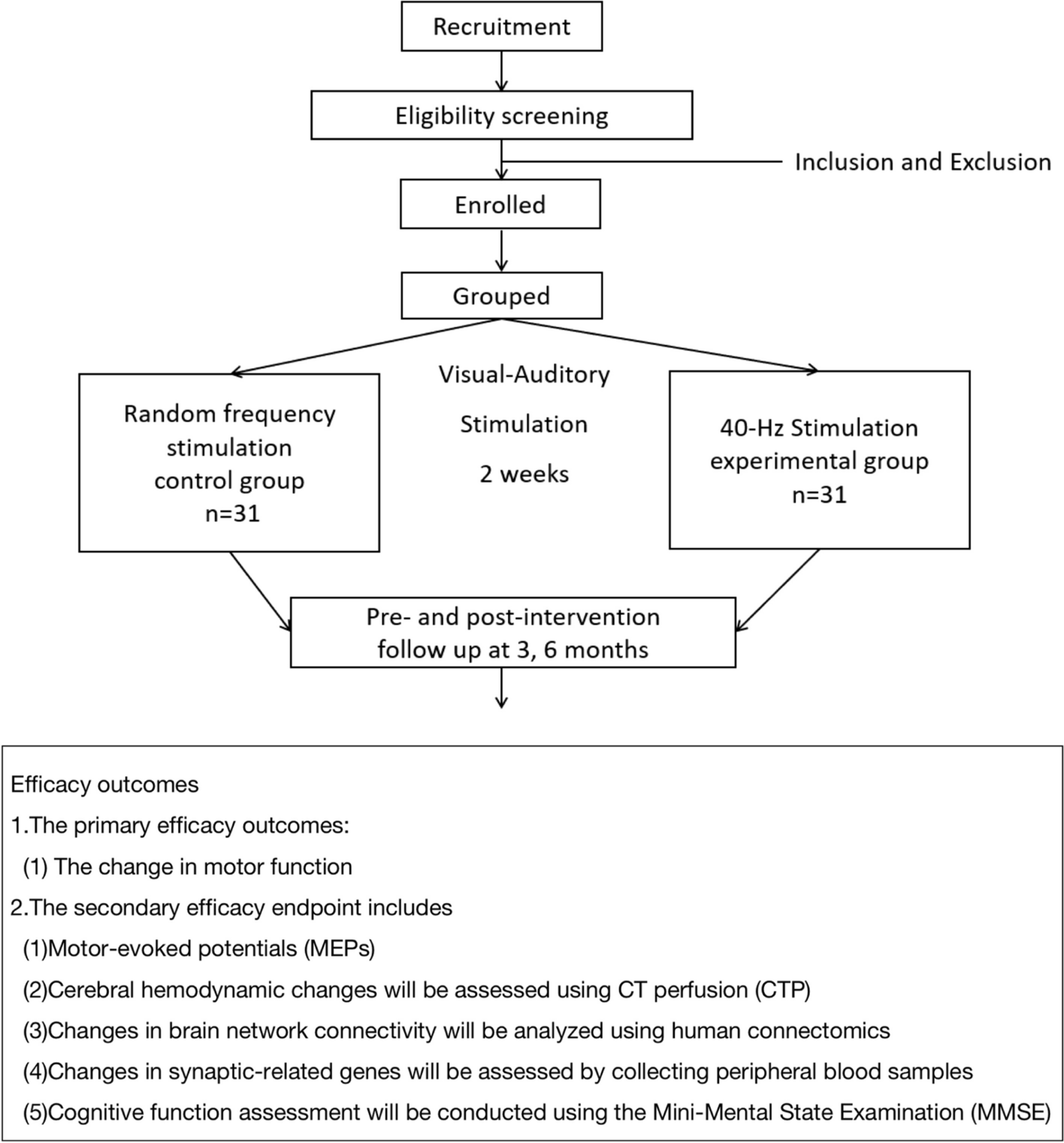



A total of 637 studies were identified from a search of OVID Medline, OVID Embase, and The Cochrane Central Register of Controlled Trials. After the removal of duplicates (n=93) and articles that did not align with the eligibility criteria by title, abstract and full text (n= 537), a sum of 7 articles have been included in this review [23,24,25,26,27,28,29] (Fig. 1).
Fig. 1
PRISMA flowchart of the study selection process
Study characteristicsAll 7 studies in this review were conducted in the United Kingdom and published in English. Studies were published between 20th July 2020 and the 2nd of December 2021. The trial population of each study consisted of adults, however, age limits for recruitment varied between each publication. None of the trials reviewed clarified UK or British citizenship as a pre-requisite for recruitment. One study aimed to only recruit adults aged 30 and above [23]. Two studies recruited all adults aged 18 and above [24, 25]. Two studies focused on recruiting adults aged 50 and above [26, 27] and age limits were applied to the remaining two studies: ages 18 to 84 [28] and ages 18 to 55 [29] respectively. The trial phases also varied, and include phase 1/2 (n=1, 14%) [28], phase 2 (n=4, 57%) [23, 24, 26, 27] phase 3 (n=1, 14%) [28] and phase 4 (n=1, 14%) [25].
Enrolment in these studies took place between 23rd April 2020 and 30th June 2021, with the desired primary outcome of each being the determination of the safety, reactogenicity and immunogenicity of injectable vaccinations against COVID-19. The vaccines investigated in the selected publications are as follows: ChAdOx1 nCoV-19, AstraZeneca; BNT162b2, Pfizer–BioNTech; mRNA-1273, Moderna; NVX-CoV2373, Novavax; Ad26.COV2.S, Janssen; CVnCov, CureVac and VLA2001, Valneva.
Outcome measuresA sum of 23,994 participants were enrolled to take part in COVID-19 vaccine RCTs at sites across the UK. Of this, ethnicity data was reported for 20,439 (85.2%) participants during either the enrolment or randomisation process. Raw data on participant demographics can be found in Table 1.
Table 1 Breakdown of raw values and the calculated prevalence of Black adults and adult ethnic minorities in the reviewed literaturePrimary outcomeCombining data from all 7 studies reviewed, 0.45% (91 of 20,439) of analysed participants identified as Black (Table 1). A weighted average based on trial size of Black adult participation (0.45%) was also calculated. The highest prevalence included in a single study to be 1.3%, (6 of 463) [26], with the lowest prevalence at 0% (0 of 679) [25] (Table 1).
A standard mean of 0.59% (95% CI: 0.13%, 1.05%) representation for all reviewed publications was calculated across all studies included (Fig. 2). With Black adults making up 2.67% of the UK adult population [15,16,17], a two-tailed, one-sample t-test comparing the mean representation against the 2011 census figure provides evidence (p < 0.001) that Black adults were under-served in UK-based COVID-19 vaccine RCTs.
Fig. 2
Plot with squares depicting the inclusivity (as a percentage) of Black adults across all 7 studies alongside a diamond depicting overall mean (with ends representing 95% CI) in comparison to the proportion they make up within the UK population (as represented by the line at 2.67%). NB: “No. black adults” denotes the number of Black adults enrolled in each study
Secondary outcomeA total of 1244 (6.10%) adults who identified with a minority ethnic group (including Black), provided data for all 7 studies. The corresponding weighted average was 6.08%. The level of ethnic minority representation varied, with the highest prevalence being 25.27% (based on 117 of 463 randomised) [26] and the lowest being 3.68% (25 of 679) [25] (Table 1).
A standard mean of 8.94% (95% CI: 2.07% - 15.80%) adult ethnic minority representation was calculated (Fig. 3). With adult ethnic minorities make up 16.30% of the UK population [17,18,19], a two-tailed, one-sample t-test comparing the mean representation against the 2011 census figure provides evidence (p = 0.039) that the minority ethnic group as a whole was under-served in UK-based COVID-19 vaccine RCTs.
Fig. 3
Plot with squares depicting the inclusivity of black adults and ethnic minorities (as a percentage) across all 7 studies alongside overall mean (with ends representing 95% CI), in comparison to the general population of the UK (as represented by the line at 16.30%)
Inclusion and exclusion criteriaThere was no identifiable exclusion of any ethnic groups when reviewing the inclusion and exclusion criteria of the studies. However, over half (n=4/7, 57%) listed insufficient English language level as grounds for exclusion [23, 26, 27, 29].
Recruitment techniquesThe recruitment methods used across each study remain relatively similar. All 7 studies utilised advertisements on social media as well as in public forums such as radio, newspapers and magazines to raise public awareness of the trial. Each study involved an online component of the recruitment and screening process, including forms to register interest in the trial. A major method for recruitment across all 7 studies - and the only recruitment method for one publication [28] - included email distribution to individuals who have already given consent to be contacted for any clinical trial at any trial sites. This includes databases such as the NHS COVID-19 online vaccine research registry, the Oxford Vaccine Centre databases and the NIHR COVID-19 vaccine volunteer database. Other recruitment techniques included direct mail out via the most recent electoral roll and using local GP practises or Trusts as participant identification centres.
Study locationsTo provide some potential context to our primary and secondary outcome findings we have investigated the site locations of the 7 studies reviewed. In total, 87 sets of data collated from clinical trial sites across the UK contributed to the studies included in our review. Of these, 1 was collected from Northern Ireland, 4 from Wales (0.6% black, 4.4% non-white), 4 from Scotland and 78 from England (Fig. 4 & Supplement Figure 1). The majority of datasets (n=17, 19.5%), reported came from sites located in the South-West of England (0.9% black, 4.6% non-white) with the East of England (2.0% black, 9.2% non-white) having the lowest number of reported datasets (n=2, 2.3%). The remaining datasets reported per region of the UK are as follows: London (n=15, 17.2%; 13.3% black, 40.2% non-white), South-East England (n=13, 15.0%; 1.6% black, 9.3% non-white), North-West England (n=11, 12.6%; 1.4% black, 9.8% non-white), Yorkshire and the Humber (n=7, 8.1%; 1.5% black, 11.2% non-white), East Midlands (n=5, 5.8%; 1.8% black, 10.7% non-white), West Midlands (n=4, 4.6%; 3.3% black, 17.3% non-white ) and North East England (n=3, 3.5%; 0.5% black, 4.7% non-white). Breakdowns of ethnicity by area were obtained from the 2011 census [15] with data for Scotland and Northern Ireland unavailable.
Fig. 4
Number of reported datasets per region. *denotes where location was not able to be mapped
Risk of biasUsing the RoB 2 tool, [22], each study was determined to have a low risk of bias. Whilst three studies did not provide outcome data for nearly all of the participants randomised [23, 27, 28] (determined as over 95%), the provision of an intention-to-treat or modified intention-to-treat analysis was considered sufficient evidence that this did not influence the study outcomes.
留言 (0)