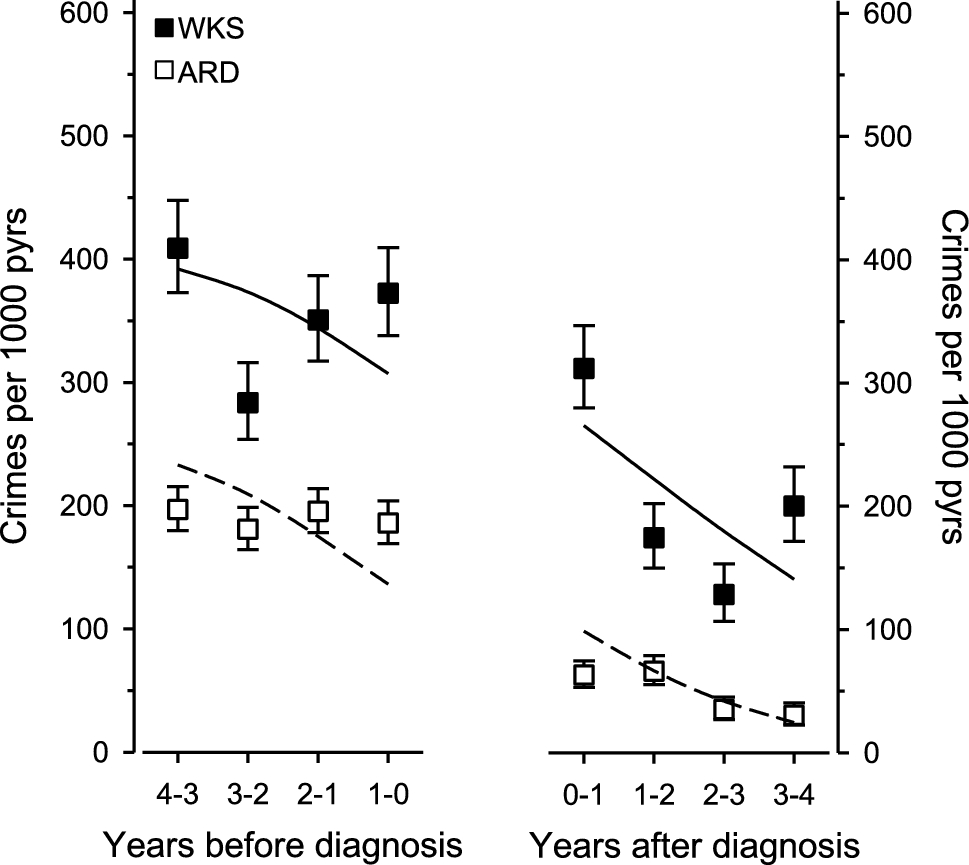
This is the first systematic study to examine criminal behavior in patients with alcohol-related neurocognitive disorders, and, as such, our results present an important point of reference. We found that WKS patients were 3.9 times and ARD patients 2.6 times more likely to commit crimes in the 4 years before diagnosis than the same-aged general population of the same sex. However, crime rates declined linearly in the 4 years surrounding diagnosis, with a noticeable drop after diagnosis. Multiple offending was common, with approximately 62% of WKS patients and 55% of ARD patients who had engaged in criminal activities before diagnosis having committed more than one crime, and some individuals having a record of dozens of offenses. The main types of crimes were property and traffic crimes, followed by violent crimes. Criminal behavior did not affect mortality adjusted by age, sex, and year of diagnosis.
Patients with WKS or ARD are known to have a history of significant alcohol consumption [29, 30], a high likelihood of comorbid alcohol dependence [31], and a tendency to continue to use alcohol even after diagnosis [32]. Alcohol use is strongly correlated with crime, particularly violent crimes [13] involving male offenders and male victims [33]. In Finland, 64% of male and 60% of female homicide offenders suffered from alcohol or drug abuse, and the majority committed the homicide while drunk [34]. Similarly, 72% of assault crimes were committed under the influence of alcohol when the victim was male (vs. 50% when the victim was female) [34]. Alcohol is known to elicit aggression and reduce behavioral control, probably via multiple pharmacological, cognitive, psychological, and social mechanisms [35, 36]. Alcohol has stimulative and anxiolytic properties, and it disrupts executive cognitive functions, which are central in behavioral self-regulation [36, 37]. While there has been limited research on the pre-diagnosis life circumstances of individuals with alcohol-related neurocognitive disorders, they often exhibit various socioeconomic factors that could contribute to criminal behavior, including unemployment, single marital status, and a family history of alcohol abuse [30].
Criminal behavior is particularly prevalent in neurocognitive disorders that affect the frontotemporal or frontal-subcortical circuits such as frontotemporal dementia, semantic variant of primary progressive aphasia, and Huntington’s disease [11, 12]. This is consistent with frontal lobe dysfunction being associated with aggressive and antisocial behavior. Correspondingly, alcohol neurotoxicity mainly affects the frontal lobes; persons with alcohol use disorders show decreased metabolic activity in the frontal lobes as well as frontal cortical atrophy [38].
While WKS and ARD are typically perceived as disorders affecting memory, their neuropsychological profiles also show impairment in executive control [39, 40]. The cognitive effects of alcohol may manifest as neuropsychiatric symptoms, which are highly prevalent in persons with alcohol-related neurocognitive disorders. Of institutionalized patients with WKS or other alcohol-related cognitive disorders, 96% manifested at least one neuropsychiatric symptom, most commonly irritability/lability, agitation/aggression, and disinhibition [41]. These neuropsychiatric symptoms, coupled with the typically younger age of individuals with WKS, may account for the higher likelihood of criminal behavior observed in WKS patients, both before and after diagnosis, in comparison to ARD patients.
Criminal behavior is much more common in persons with WKS or ARD than in patients with progressive dementias. In a previous study by our group, the incidence of crimes before diagnosis in men with Alzheimer’s disease was about 50 per 1000 person-years (in women, less than 10 per 1000 person-years) [12]. This rate is several-fold lower than the incidence of crimes shown in our study, which was 354 per 1000 person-years in WKS patients and 190 per 1000 person-years in ARD patients. Considering progressive dementias, even the patient group with the most criminal behavior, men with frontotemporal dementia, had a lower incidence of criminal offending than did the patients in our study [12]. Age-related factors may contribute to the higher incidence of criminal behavior observed in WKS and ARD patients, as the decline in criminal activity with age is a well-documented phenomenon. Alcohol-related neurocognitive disorders primarily affect younger age groups [42], in contrast to progressive dementias such as Alzheimer's disease.
Our results show that persons with WKS or ARD tend to commit more violent crimes than persons with progressive dementias. Violent crimes were rare in patients with Alzheimer’s disease (0.7 per 1000 person-years) or even frontotemporal dementia (4.0 per 1000 person-years) [12]. This finding is in line with previous studies; of seven dementia patients in a forensic hospital, the four patients with ARD were incarcerated for violent crimes, such as murder or assault, while the two patients with Alzheimer’s disease were incarcerated for non-violent crimes (larceny). The patients with ARD had also committed between 1 and 6 earlier crimes, whereas other dementia patients had committed none [22].
Our findings demonstrate a linear decrease in criminal activity during the 4 years surrounding the diagnosis of an alcohol-related neurocognitive disorder. Especially in ARD patients, crime rates experienced a substantial reduction following the diagnosis of an alcohol-related neurocognitive disorder. Comparing the rates before and after diagnosis, we observed a remarkable decrease to approximately one-third of pre-diagnosis levels. One possible explanation is that WKS and ARD patients may experience a progressive decline in their functional and cognitive abilities, reaching a point where they are no longer able to engage in criminal behavior. Alternatively, the act of receiving a diagnosis may signify entry into the health care system, leading to improved access to health and social care, including substance abuse treatment. Our results imply that intervention and support following diagnosis may have an impact on reducing the likelihood of engaging in criminal behavior. In Finland, a diagnosis of moderate to severe dementia or alcohol use disorder can result in revocation of driving and gun licenses, which may contribute to a decrease in traffic-related and violent offenses. Incarceration is unlikely to explain the decline in criminal activity since imprisonment sentences in Finland are reserved for serious offenses and tend to be relatively short.
Criminal behavior, particularly frequent offending, is associated with multiple psychosocial problems and premature death [27]. Even though the patients in our study had elevated mortality compared with the general population, our results did not indicate a difference in the adjusted mortality between patients with and without criminal behavior. This observation may be attributed to the fact that the elevated mortality in this patient group is primarily driven by chronic alcoholism and its related health issues, with criminality representing just one aspect of the many complex problems they confront.
Strengths and limitations
The main strength of our study was its register-based design, which allowed us to effectively investigate patients with alcohol-related neurocognitive disorders, a population that is typically challenging to engage in clinical research. Through the utilization of Finland’s extensive nationwide electronic register databases, we successfully linked information from both health care and police registers, enhancing the comprehensiveness of our study. The high quality and reliability of Finnish health care registers, widely used in research and health monitoring and planning, further strengthened the validity of our findings. To compile a comprehensive dataset on criminal activity, we used the police register, which captures all suspected criminal offenses reported to the police, as opposed to relying solely on court data, which would only cover convictions. The use of the police register ensures the reliability of our crime-related information, due to strict legislative oversight of law enforcement and Finland’s standing as one of the least corrupt nations globally. By acquiring data on crimes directly from the police register rather than relying on self-reports, we mitigated the potential biases associated with reporting or recall. This approach provided a more objective perspective on criminal activities, although it should be acknowledged that some crimes may go unreported to the police.
The register-based design of our study, while advantageous in many aspects, also poses limitations. The health care register used here (FHDR) lacks detailed patient information such as clinical or autopsy data on individual patients. Neither were we able to obtain data on socioeconomic factors or risk factors like alcohol or tobacco use. While associations can be identified from register-based observational data, the ability to fully understand underlying mechanisms and establish causality is inherently limited in this type of study design.
Diagnoses of WKS or ARD were made during routine clinical practice, introducing the possibility of underdiagnosis and misdiagnosis. In general, dementia diagnoses recorded in Finnish health care registers are considered highly accurate [43]. However, a clear discrepancy exists between the prevalence of alcohol-related neurocognitive disorders from autopsy studies and the rates of clinically diagnosed WKS or ARD, indicating these disorders are significantly underdiagnosed [44,45,46]. While this could be due to the individuals being less inclined to seek medical attention, other contributing factors may include the lack of clinicians’ expertise in this field or the absence of well-established diagnostic criteria; as a result, many suspected cases might go undocumented [46].
Another limitation of our study stems from the fact that our dataset lacked information on the alcohol use disorder diagnoses of our study participants. As a result, it remains unclear whether crime rates associated with alcohol-related neurocognitive disorders are higher than those in alcohol use disorders without substantial cognitive impairment (which would imply a compounding effect of alcohol use and cognitive impairment), or if they are comparable or even lower (suggesting, perhaps, that cognitive impairment or some other factor may reduce criminal behavior). While the nationwide design of this study probably represents accurately the Finnish population, there are limitations in generalizing criminal studies to other countries or societies, as legal frameworks, justice systems, and other influencing factors vary across jurisdictions.

留言 (0)