Study design
We included 55 depressed patients in a double-blind, multicenter RCT comparing active tPEMF versus sham in a 1:1 ratio. Fifty completed the trial and were included in the current analyses. This study was approved by the Medical Ethical Committee of the University Medical Center Groningen (UMCG), and by the local research office of each participating site. Written informed consent was obtained from each participant. The study was conducted according to the Declaration of Helsinki. The trial was registered at the Dutch Trial Register (http://www.trialregister.nl) under number NTR3702.
Study population
We included patients who met DSM-IV criteria for MDD, currently in a depressive episode, assessed by the Mini-International Neuropsychiatric Interview (MINI) [22]. Inclusion criteria were the presence of at least a moderately severe depression (> 17 on HAMD-17), non-responsiveness to one or more antidepressants given for at least 4 weeks in an adequate dose (i.e. the defined daily dose (DDD) [23]) during the current episode, age between 18 and 80 years, and having a good understanding of spoken and written Dutch.
Patients were excluded if they were Magnetic Resonance Imaging (MRI) incompatible (having metal implants, claustrophobia, refusal to get informed of structural brain abnormalities, and suspected pregnancy). Additional exclusion criteria were presence of MDD with psychotic features, other major psychiatric disorders such as a primary psychotic disorder or an antisocial or borderline personality disorder, a neurological disorder such as dementia or epilepsy, visual or hearing problems that could not be corrected, suicidal thoughts (> 2 on HAMD-17 for suicidal ideation) or a history of a serious suicide attempt, recent (past three months) alcohol or drug abuse or dependence, lactation, inability to comply with treatments and/or assessments, recent change (last 4 weeks) in antidepressant medication or requirement to change antidepressant medication during the course of the study, use of benzodiazepine(s) more than 2 mg lorazepam or equivalent per day within the last 4 weeks or during the course of the study, use of medication indicated for a somatic disease that may have affected mood within the last 4 weeks, excessive use of coffee (> 10 units per day) or alcohol (> 5 units per day), or recent use (within four weeks) of cannabis or any other non-prescribed psychotropic drugs or unwillingness to abstain from these substances during the study. The use of antipsychotics and lithium was allowed.
Treatment
Eligible patients were randomly assigned to either 5 weeks active tPEMF or 5 weeks sham stimulation. Sessions took place on weekdays for 30 min during office hours. All involved were blinded for the treatment condition. Further details regarding randomization and treatment procedure are described elsewhere [7]. Change in depression severity was measured by the HAMD-17 [24] immediately post-treatment. Functional MR scans were made at a maximum of five days pre-treatment and on the same day of the last treatment session. During the scans, participants performed two tasks: the Wall-of-Faces (WoF) task [13] and a Monetary Incentive Delay (MID) task [25].
WoF-Task
During the WoF task, an array of 32 human faces was presented for 3 s followed by an additional reaction period of 1.5 s. Participants had to indicate whether they saw more happy or angry facial expressions –an affective judgment– or whether they saw more male or female faces—a gender judgment-, used as a control condition. In half of the trials, the majority of faces was clear (unambiguous trials) because the array was presented in a 26-6 or 6-26 ratio. In the other half of the trials the ratio of faces was presented in a 16-16 ratio and thus ambiguous. This resulted in two different ambiguous conditions (affect: angry = happy (16-16); gender: male = female (16-16)) and two unambiguous conditions (affect: angry ≠ happy (26-6 or 6-26); gender: male ≠ female (26-6 or 6-26)). In total, there were eight epochs; four in which participants had to perform an affective judgment and four in which they had to perform a gender judgment. During one epoch the ambiguous (four per epoch) and the unambiguous trials (four per epoch) were presented in random order. The four conditions were thus presented sixteen times in total. Stimuli were presented in E-prime version 2.0 (Psychology Software Tools, Sharpsburg, PA). A short practice session was performed prior to scanning.
MID-task
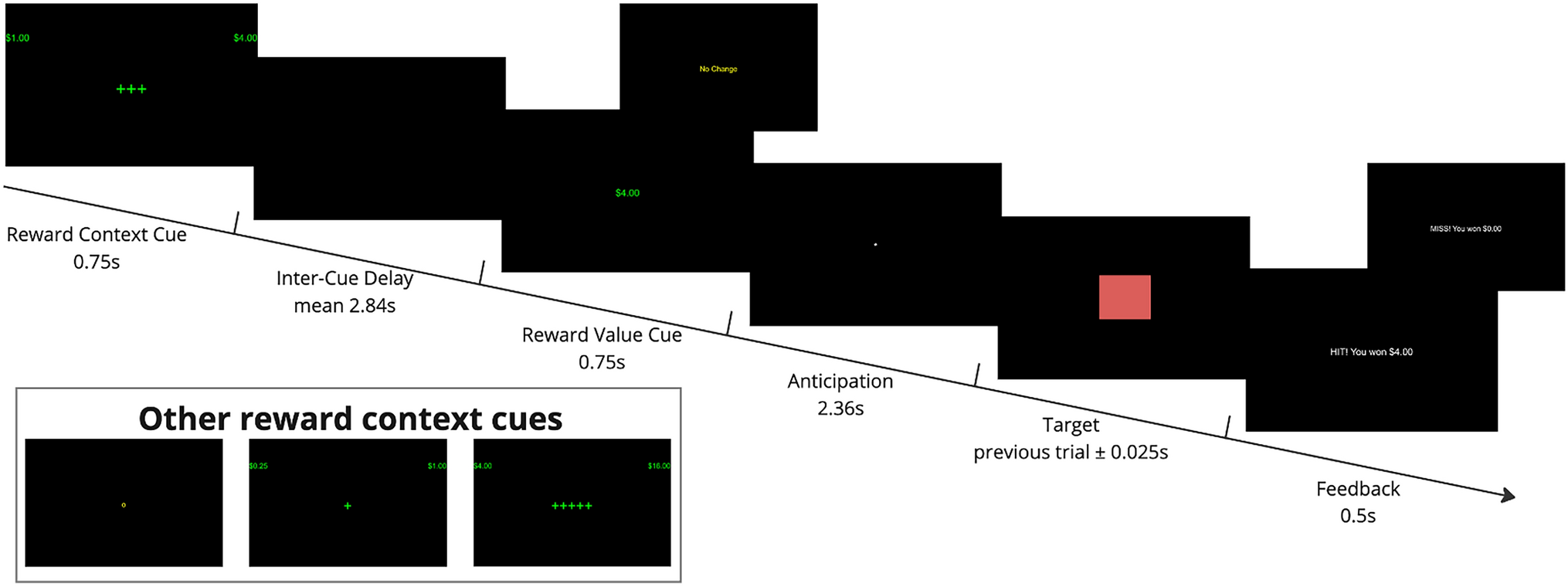
The Monetary Incentive Delay task was adapted from [25]. This event-related task consisted of 20 reward trials (monetary gain), 20 neutral trials (no gain no loss), and twelve loss trials (monetary loss). The total reward obtained during scanning was added to the financial compensation for participation; the total amount was fixed so participants unknowingly always gained € 10,-. During a trial, participants saw a cue for 1.5 s for one of the potential outcomes: reward (+ €), neutral (= €), or loss (-€), which was followed by a blue squared target presented for 0.5 s. Participants were instructed to press a button in response to the cue as fast as possible to maximize their outcome. Feedback (1.5 s) concerning the outcome was given directly after the cue. The inter-stimulus-interval (ISI) varied between trials (ISI-1 between cue of the possible outcome and target: 3.5 s–9.5 s; ISI-2 between target and outcome: 2.5–8.5 s) to prevent expectancy effects, as did the duration of trial-separating fixation cross (3.0–7.0 s). Participants completed four blocks of thirteen trials comprising all conditions, interspersed with 10 s resting periods. The pseudo-randomized order of trials and ISIs was determined with optimized experimental design to maximize efficiency [26, 27] Reward success rates were set at 80% to prevent habituation. Outcome for the neutral and loss trials was set at 100%, so that in the neutral trials participants never received a reward and in the loss trials participants always lost money. Stimuli were presented in E-prime version 2.0 (Psychology Software Tools, Sharpsburg, PA). A short practice session was performed prior to scanning.
MRI acquisition parameters
All fMRI-images were acquired using a 3 Tesla Philips MRI scanner (Best, The Netherlands). Functional images were acquired using T2*-weighted echo planar images sequences. Sequence parameters: single shot EPI; 37 slices; 3.5 mm slice thickness; 0.0 mm gap; 224 × 129.5 × 224 mm (anterior–posterior, foot-head, right-left) field of view; 64 × 61 scan matrix; transverse slice orientation; repetition time 2000 ms; echo time 20 ms; flip angle 70°. In addition, a T1-weighted whole-brain anatomical image was acquired (resolution 1 × 1 × 1 mm).
Statistical analyses of behavioral data
Analyses of behavioral data were performed using IBM SPSS version 24.0 software (IBM, Chicago IL, USA). For the WoF-task we calculated median scores (non-normally distributed) for the response times of the conditions affect ambiguous, affect unambiguous, gender ambiguous, and gender unambiguous. For the MID-task, we calculated median scores for the response time to the target cue for the three conditions (reward, neutral, or loss). Outliers were calculated using the median absolute deviation (MAD) [28]. We used a criterion of 3 + or – the MAD for the different conditions to remove outliers. Differences between the conditions were tested using Wilcoxon rank tests for the median scores. To test for the effect of treatment on behavioral outcome, a linear mixed model with a random intercept was applied with response time score per different condition as dependent variable and treatment group, time (baseline or week 5), and the interaction between time and treatment group as covariates. The level of statistical significance was set at α < 0.05.
MRI data pre-processing
Analyses of MRI data were performed using Statistical Parametric Mapping (SPM12, version number 6470; FIL Wellcome Department of Imaging Neuroscience, London, UK), implemented in MatLab (r2015a). First, PAR files were converted to NIFTI format with an in-house script. Both anatomical and functional images were manually reoriented to the anterior commissure – posterior commissure plane. Further preprocessing consisted of realignment of functional images. Realignment-parameters were visually checked. For all realignment-parameters, their first derivatives and the framewise displacement [29, 30] were calculated to add as covariate in the first-level model later on. Participants were excluded for that particular task if there was progressive movement exceeding 3 mm; in case a single volume would exceed 3 mm, we assumed that scrubbing would compensate for this. Next, coregistration of the functional images to the anatomical image, and spatial normalization to the Montreal Neurological Institute (MNI) space, reslicing the images into a 3 × 3 × 3 mm voxel grid were performed. Coregistration and normalization were visually checked to see if manual correction was necessary, which was not the case. The data was spatially smoothed with an 8 mm full-width at half-maximum Gaussian Kernel.
First level models
For both tasks, a first-level GLM was set up per participant containing two time sessions. Regressors for the different onset times of the conditions were convolved with a canonical hemodynamic response function. Other regressors in the GLM were realignment parameters, their first derivatives, and dummy variables for the volumes showing a framewise displacement of > 0.9 [29, 30].
Wall of faces task
For the WoF-task five different regressors were defined: affective ambiguous and unambiguous, gender ambiguous and unambiguous, and instructions. We calculated the following contrasts on baseline: affect > gender, ambiguous affect > ambiguous gender, affect ambiguity > affect unambiguity. For the interaction over time, we calculated contrasts for: affect > gender (pre > post), ambiguous affect > gender (pre > post), and affect ambiguity > unambiguity (pre > post),
Monetary incentive delay task
For the MID-task six regressors were defined: anticipation of reward, loss, and neutral and consummation of reward, loss, and neutral. We calculated contrasts (at baseline) for anticipation reward > neutral, anticipation loss > neutral, anticipation reward > loss, consumption reward > neutral, consumption loss > neutral, and consumption reward > loss. For the effects over time, we calculated contrasts for anticipation reward > neutral (pre > post), anticipation loss > neutral (pre > post), anticipation reward > loss (pre > post), consumption reward > neutral (pre > post), consumption loss > neutral (pre > post), and consumption reward > loss (pre > post),
Second level
For second-level analyses, a two-sample t-test model was built. We determined task activation using the baseline scans and compared baseline activation between the treatment groups (sham versus active). For the effect over time, we used the respective first-level contrasts to compare the treatment groups. We performed whole-brain correction. The threshold was set at p < 0.05 Family Wise Error (few)-corrected at the cluster level, with an initial voxel-defining threshold of p < 0.001.
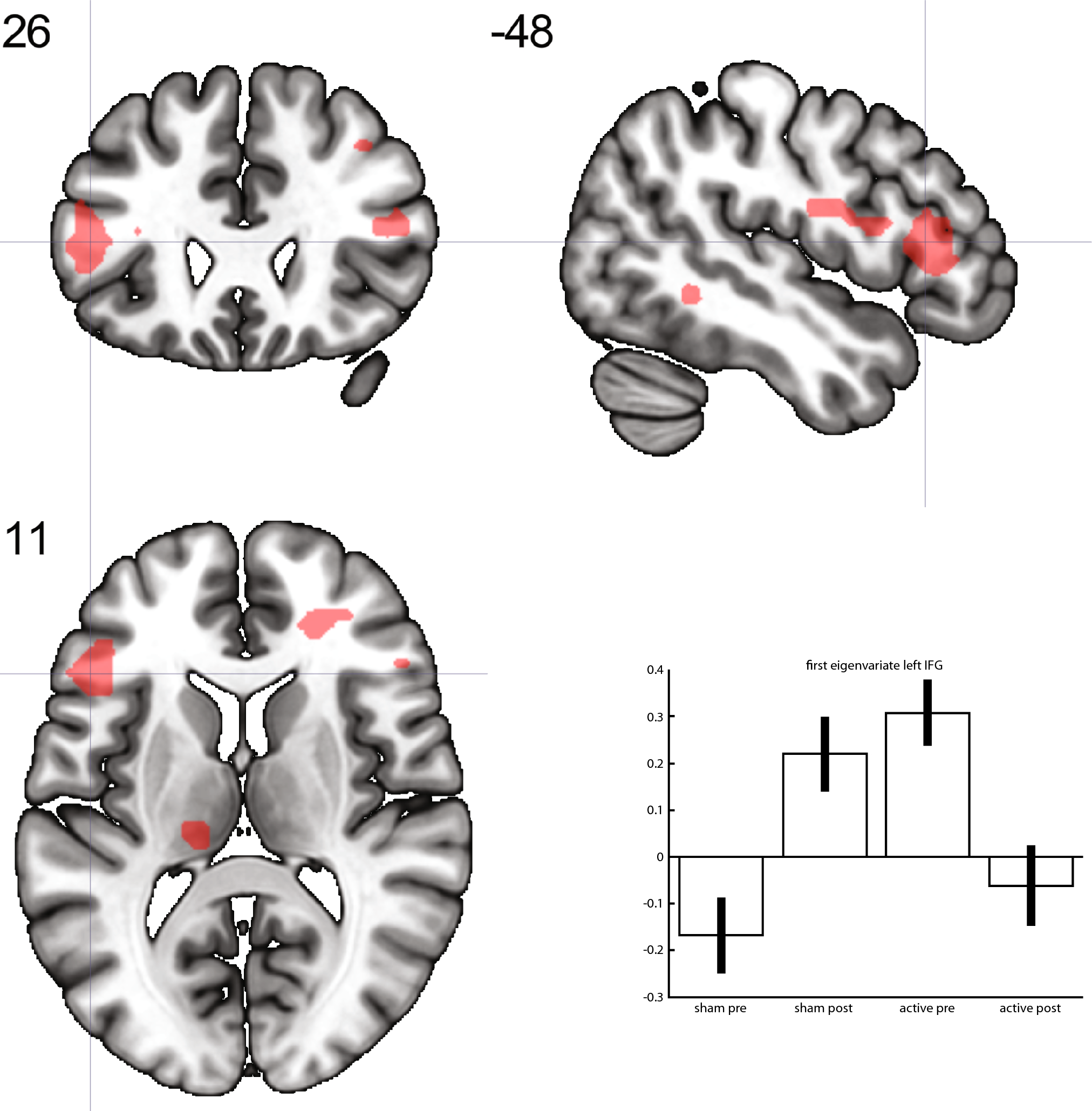
To relate clinical findings to the outcome of the second-level analyses, we extracted the average effect size of the interaction for the Region Of Interest (ROI) defined by the respective clusters. Using regression analyses we explored the correlation between the ROI effect size and changes in HAMD-17-scores.
For visualization purposes, we built a full factorial model containing scans for the two groups and two time moments (pre-treatment, post-treatment for sham and active treatment). We used the significant clusters of the effect over time as a mask to extract the first eigenvariate for each condition and time moment and these were used for plotting bar graphs. No statistics were applied to these values.

留言 (0)