Fosfomycin, first discovered in Spain in 1969 [1], is a bactericidal drug that acts by inhibiting a reaction catalysed by enzymes in the first phase of the synthesis of the bacterial cell wall. Due to its action, peptidoglycan (PG) is not formed, leading to the loss of integrity of the PG layer, cell lysis and death. This inhibitory action occurs at an earlier stage than the inhibitory action of beta-lactams or glycopeptides [2]. Employed as a combination partner, fosfomycin has a synergistic effect.
The spectrum of activity of fosfomycin includes activity against both Gram-positive and Gram-negative bacteria (GNB) [3], including multi-drug-resistant (MDR) and extensively-drug-resistant pathogens [4]. Moreover, fosfomycin has shown high tissue penetration into subcutaneous and muscle tissue [5], lung [6], bone tissue [7,8] and cerebrospinal fluid [9]. In-vitro studies have shown that fosfomycin has synergistic activity as a combination partner with several agents [10], including meropenem [11,12], amikacin, colistin [13], ceftazidime/avibactam [14], ceftolozane-tazobactam and aztreonam [15]. It was hypothesized that fosfomycin had a possible role as a combination therapy in in-vivo clinical studies.
Two randomized clinical trials (RCTs) were performed to assess the efficacy of intravenous (IV) fosfomycin as monotherapy for the treatment of urinary tract infections [16,17]. Encouraging data on IV fosfomycin combined with colistin against carbapenem-resistant Acinetobacter baumannii infections [18] have also been reported. Recently, the potential application and safety of IV fosfomycin in the treatment of neonatal sepsis were explored in an RCT involving 120 patients [19].
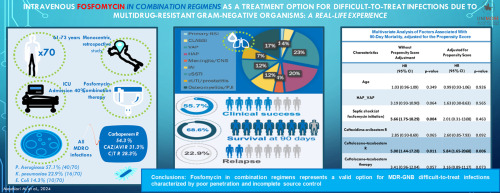
However, the real-world synergy of fosfomycin with ‘first-line’ MDR-GNB has been poorly investigated. Most published experiences come from limited small cohort studies, mainly focusing on bloodstream infections (BSIs) due to carbapenem-resistant Enterobacterales [20] or A. baumannii infections [21], [22], [23]. Furthermore, there are still conflicting results concerning the advantage of combination therapy over monotherapy for Pseudomonas aeruginosa bacteraemia and other complicated infections in critically ill patients [24], [25], [26].
The aim of this study was to evaluate the efficacy of fosfomycin in combination regimens for the treatment of infections caused by MDR-GNB, focusing on difficult-to-treat (DTT) infections due to high resistance profiles (mainly carbapenem resistance) and infection sites with poor penetration, such as lung, bone, intra-abdominal (IAI) and central nervous system (CNS) infections, with incomplete source control.





留言 (0)