
記住我
In the current study, patients with mild to moderate AD, and healthy controls (HC) were recruited from the Memory Clinic at Copenhagen University Hospital – Rigshospitalet and the Memory Clinic at Zealand University Hospital, Roskilde. Patients with AD met the NIA-AA criteria for probable AD with amnestic presentation [36] with the diagnosis being determined based on a consensus conference. The consensus conference included information from structural imaging and, in most instances, [18F]FDG positron emission tomography (PET). Some patients underwent lumbar puncture (nAD=18) with evaluation of amyloid-β42, phosphorylated tau, and total tau while some underwent a [11C] Pittsburgh compound-B-PET scan (nAD=2) or both (nAD=3) as part of the clinical work-up.
In patients with AD, the inclusion criteria included (1) a mini-mental state examination (MMSE) [37] score of 16–28, (2) age between 50 and 90 years, (3) native Danish speaker, (4) at least 7 years of education, (5) hearing and vision sufficient for neuropsychological examination, (6) no alcohol or drug abuse within the last two years, (7) no contraindications for MRI, (8) an MRI or CT scan that supported the diagnosis of AD, (9) the general health conditions of the patient allowed participation in the study (as judged by the principal investigator), and (10) living with a caregiver who was able to assist the patient with the home EEG recordings.
The following exclusion criteria were applied: (1) epilepsy prior to the diagnosis of AD, (2) focal pathology (except AD related atrophy) in the hippocampus, i.e. hippocampal sclerosis, (3) living with a relative with serious illness or impaired activities of daily living since the participant may need help to participate in the study, (4) living in a nursing home, (5) psychiatric (except mild depression) or neurological conditions that affects the brain except AD, (6) currently treated with anti-epileptic medication, tricyclic antidepressants or antipsychotics, (7) daily or almost daily administration of medication with known anticholinergic or adrenergic effect, which may affect cognitive abilities or EEG, (8) large cerebral infarctions or more than four lacunar infarctions on MRI, (9) suffering from facial tics/facial hyperkinetic disorders or (10) daily use of hearing aids.
The HC were recruited from a pool of participants in other studies who had expressed interest in participating in new studies. The inclusion criteria were (1) normal cognition (as judged by the principal investigator), (2) a general health compatible with participation in the study as well as criteria 2–7 as applied in patients with AD. The following exclusion criteria were applied: (1) diagnosed with epilepsy, (2) focal pathology in the brain (except mild hippocampal atrophy) as well as exclusion criteria 5–10 as applied in patients with AD but without AD.
The study was approved by the Capital Region Ethics Committee (H-17,035,751), and by the Danish Medicines Agency (2,017,112,288), and registered at the Data Protection Agency (P-2021-866). All participants gave written and oral informed consent before participating in the study. The study is registered at clinicaltrials.gov (NCT04436341).
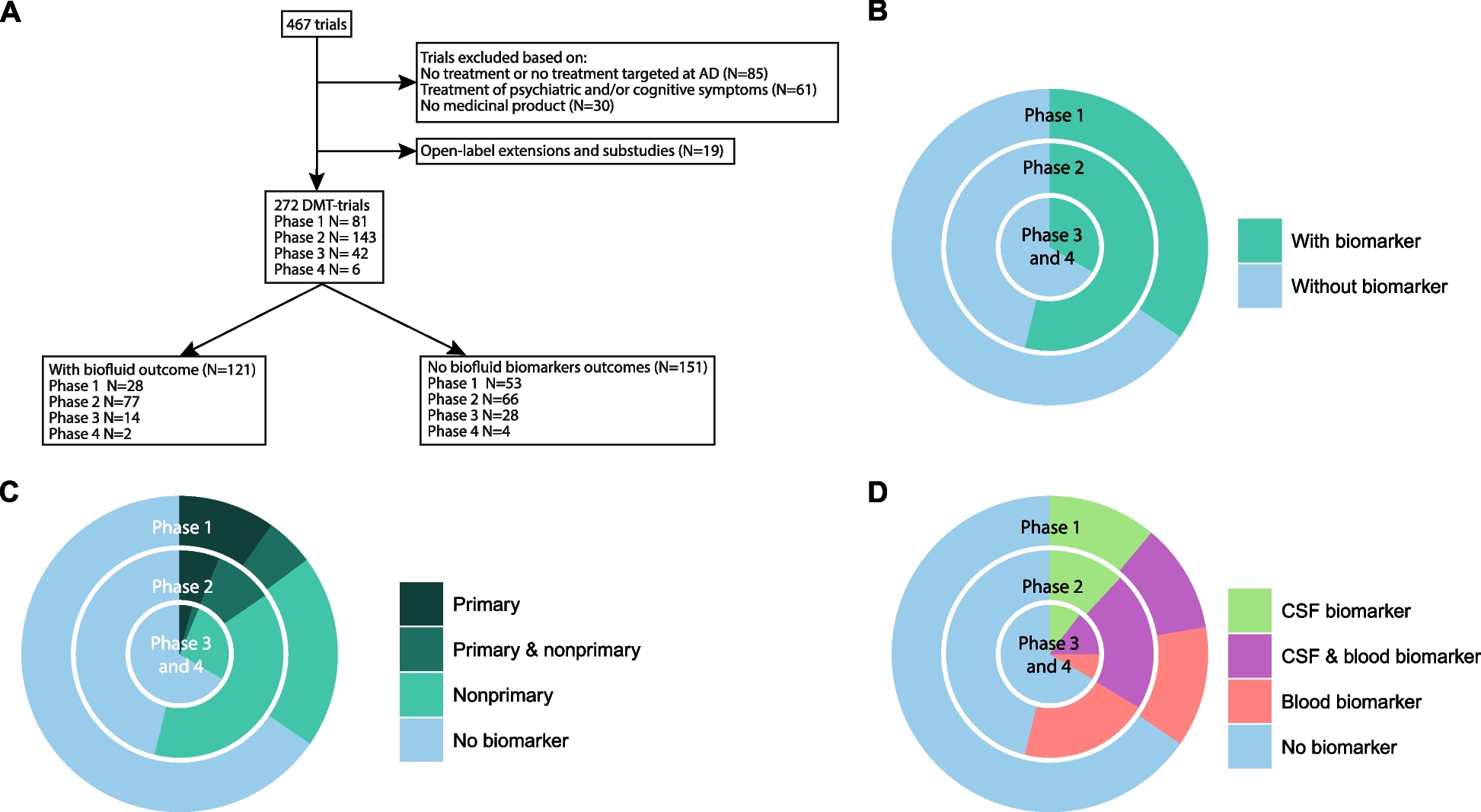
Study designIn this cross-sectional study, a total of four visits were planned for patients with AD, and HC, see Fig. 1.
Fig. 1
Study design. The patients with AD underwent the same procedures as HC except that no questionnaires were administered for the HC in visit 3
At visit 1, informed consent was obtained followed by assessment of medical history, a physical and neurological examination, the Mini-Mental State Examination (MMSE) (for assessment of global cognitive function) and an imprint of the ears using Otoform A Soft X (Dreve, Germany), a soft ear impression silicone. Subsequently, the patient underwent the following: visit 2) MRI scan (either before or after the ear-EEG recording), visit 3) standard EEG recording together with ear-EEG, Functional Assessment Questionnaire IADL (FAQ IADL) [38] (to assess everyday function), and the neuropsychiatric inventory (NPI) [39] (to assess behavioral and psychological symptoms).
Ear-EEG recording and reviewThe participants underwent up to two days of out-patient ear-EEG recording. A full description of the ear-EEG equipment and pre-processing can be found in the supplementary material.
A sharp asymmetric negative potential of 20–200 ms duration was considered an epileptiform discharge (spike/sharp wave) if it was clearly distinct from ongoing background activity and unlikely to be artifactual [40]. Due to the nature of ear-EEG, we could not investigate the spatial distribution of the spikes/sharp wave. All annotations performed by CSM underwent review by a board-certified clinical neurophysiologist (TWK), who made the final ruling. The term epileptiform discharges cover both spikes and sharp waves and assumes an underlying irritative process as seen in epilepsy, even if this cannot be stated with absolute certainty. Both CSM and TWK were blinded to the diagnosis when reviewing the EEGs.
The spike frequency was calculated by dividing the number of spikes by the amount of time (in days) when data from at least one electrode in each ear was being recorded.
The results from the ear-EEG recordings from the patients with AD and HC have been presented elsewhere [30].
MRI acquisitionAll scans were recorded on a 3T Achieva dStream (Philips, Best, The Netherlands) with a 32-channel head receive coil.
Structural image acquisition and analysisA sagittal 3D T1-weighted magnetization prepared rapid acquisition gradient echo (T1-MPRAGE) was recorded with the following acquisition parameters: repetition time (TR) 6.9 ms, echo time (TE) 2.82 ms, flip angle 9, matrix size 256 × 255, 155 slices, voxel size 1.1 × 1.1 × 1.1 mm3, The T1-weighted images were segmented using Freesurfer (version 7.2.0, https://surfer.nmr.mgh.harvard.edu/) and the volumes for each hippocampus and the inferior lateral ventricles were obtained. Both were normalized to the intracranial volume (ICV). The estimated total intracranial volume (eTIV) generated by FreeSurfer was used as an estimate for ICV in this study as has previously been shown [41].
Phase contrast mappingThe mean global cerebral blood flow (CBF) was obtained using velocity sensitive phase contrast mapping (PCM) MRI [42, 43]. Blood velocity contrast maps were acquired by a turbo field echo sequence. Measurements were acquired from an imaging plane perpendicular to the carotid arteries and one perpendicular to the basilar artery.
The blood flow in both internal carotids and the basilar artery was calculated by multiplying the mean blood velocity by the cross-sectional area from regions of interest defining each vessel. The global mean CBF was calculated by normalizing the total blood flow from each artery to the total brain weight, which was estimated from the segmentation of the structural MRI images with an assumed brain density of 1.05 g/mL. Calculations were performed using a custom-built script in Python (https://github.com/MarkVestergaard/PCMCalculator).
Arterial spin labeling MRI analysisA pseudo continuous ASL (PCASL) sequence with Look-Locker Echo Planar Imaging was chosen. The labeling plane was placed across the neck 9 cm beneath the center of the imaging slab and the labeling duration was 1650 ms. The acquisition parameters were: 13 slices, TE 10.8 ms, voxel size 3.44 × 3.44 × 6.6 mm3, FoV 220 × 220 × 85 mm3, TR was 300 ms, Look-Locker Flip-Angle 40o, slice acquisition duration 22 ms, SENSE factor 2.3, The post-labeling delays were set at [100, 400, 700, 1000, 1300, 1600, 1900 ms]. Each ASL pair (label and control) took 8 s. In the current study, the region of interest was the hippocampus, which resulted in the acquisition plane being placed parallel to the inferior lateral ventricles. After each ASL scan, a single equilibrium magnetization scan (M0) was acquired with the same parameters as the previously described ASL images except for a 10,000 ms TR.
ASL images were quantified using BASIL in FSL (FMRIB software library, version 6.0.5.1, www.fmrib.ox.ac.uk) with quantification [44] and fitting of the macrovascular compartment [45]. The initial prior of bolus arrival time was adjusted to account for the delayed arrival as seen in our sample, which resulted in a selected arrival time prior of 1.6 s. Lastly, the ASL data were registered to the T1wscan. The ASL quantification was not corrected for differences in hematocrit values.
To quantify rCBF in the hippocampus, we first extracted all the values within the hippocampus ROI segmented with FreeSurfer and then removed the voxels with zero values as these were assumed to be contaminated by CSF. Afterwards, any values more than two standard deviations above the mean were removed since they were assumed most likely to represent arteries. Finally, the median value of CBF was extracted for each hippocampus and normalized to the global mean CBF as measured with PCM and the mean of the two values were computed. Due to the both the structural and functional connectivity between the hippocampus and the precuneus [46], we wanted to investigate if a similar association between spike frequency and rCBF in precuneus was present. Here, the same approach for computing the normalized rCBF in the precuneus was used. No other regions were investigated.
StatisticsThe statistical analyses were performed in RStudio (v1.2.1335). When comparing age, education, MMSE, and the time difference between the ear-EEG recording and MRI scan, we performed t-test between AD and HC. Chi-squared tests was performed for testing for sexual distribution.
When comparing the hippocampus volume, global cerebral blood flow, and rCBF in the hippocampus or precuneus, we performed a t-test between AD and HC. Here, the distribution of the data as well as variance between groups were investigated before performing t-tests.
When comparing the number of spikes or sharp waves/24 hours (spike frequency) between HC, and AD, we calculated the rate ratio using the function rateratio from the epitools toolbox.
Simple linear regression was used to test if spike frequency significantly predicted the normalized mean rCBF in the hippocampus in patients with AD. Since it has been hypothesized that the number of epileptiform discharges increases with AD severity, we performed the same analysis with MMSE as a covariate. In the exploratory analysis, we tested if the spike frequency was associated with the normalized rCBF in the precuneus and whether a similar association between rCBF and spike frequency could be seen in HC.
The R code and output from the subsequent analyses can be found in the supplementary material.
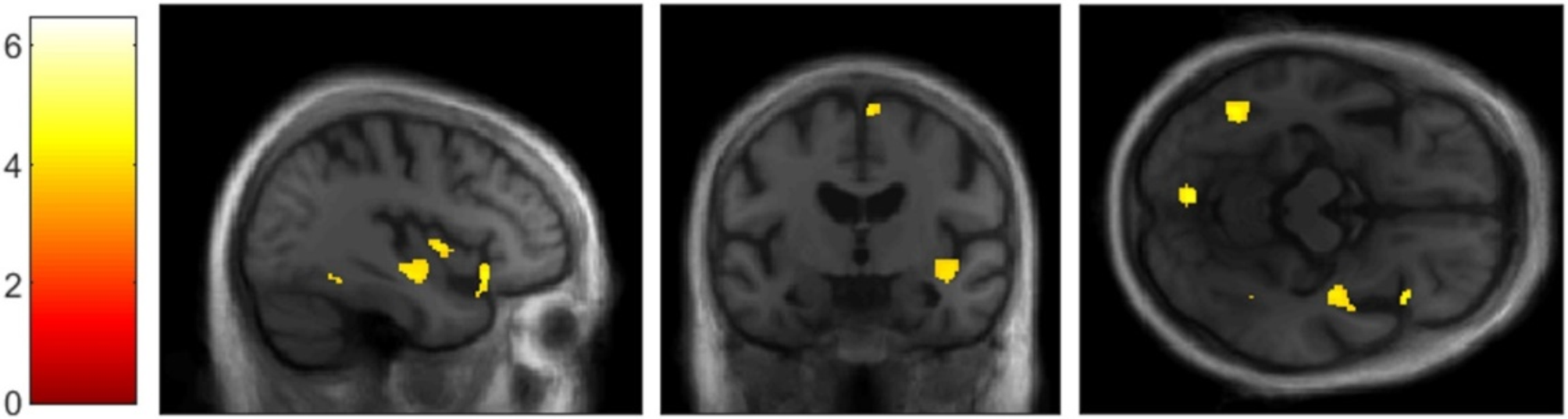
When conducting the voxel-to-voxel analysis to compare normalized rCBF between HC and AD, we performed two-sample unpaired t-tests in randomize from FSL with cluster correction.
留言 (0)