Given the evidence-based SIOP-RTSG guidelines advocating against invasive procedures to determine histology at diagnosis in the majority of children with renal tumors, imaging plays an increasingly important role in the non-invasive discrimination of pediatric renal tumors [8, 25, 34]. This retrospective multicenter study illustrates the MRI characteristics of congenital mesoblastic nephroma in an international cohort, focusing on its different subtypes and identifying potentially specific MRI characteristics of this rare neonatal pediatric renal tumor. Although we know congenital mesoblastic nephroma accounts for the majority of prenatal and neonatal renal tumors, and outcome is excellent with reported outcome rates of 95–100%, early recognition and discrimination from more malignant pediatric renal tumors is important, especially in children >3 months of age [1, 3, 11, 15,16,17, 29]. T2W isointensity particularly, appears to be potentially discriminating in the differentiation of congenital mesoblastic nephroma from the often T2W hyperintense Wilms tumor. Nonetheless, while the classic type congenital mesoblastic nephroma often appears homogeneous on imaging, the cellular and mixed type show more overlapping imaging MRI characteristics with malignant pediatric renal tumors in the same age range, such as Wilms tumor, rhabdoid tumor of the kidney, and clear cell sarcoma of the kidney [2, 3, 6, 8, 11, 21, 31, 37, 44].
Above the age of 3 months, a combination of certain clinical, radiological, and biochemical criteria are usually used to decide if a diagnostic cutting needle biopsy is indicated [26, 27]. In general, some studies have indicated the incidence of congenital mesoblastic nephroma is higher in males than females, whereas we only saw a slight predominance of male patients in our study (57.7%) [33, 45,46,47]. Metastases are described in approximately 2% of patients with the cellular type, which is in line with only one suspected metastatic case in this study [11, 13, 15, 18, 21, 35, 37]. Although its malignant potential remains a topic of debate, the rarity of metastases may be a discriminating factor between congenital mesoblastic nephroma and malignant renal tumors, especially in case of the classic type [5, 6, 8, 11, 14, 48]. Nonetheless, a total nephrectomy is the indicated treatment for all subtypes, especially given the increased likelihood of local recurrence in approximately 5% of the patients after a partial nephrectomy due to positive margins [11, 13, 15, 18].
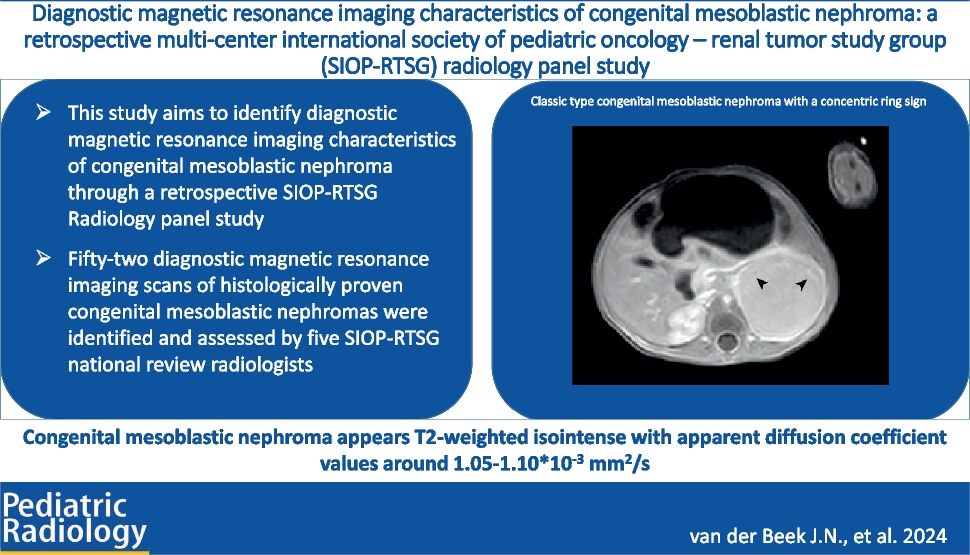
We found that the classic type congenital mesoblastic nephroma often appears as a solid, well-defined, and homogeneous tumor, showing isointensity compared to the renal parenchyma on T2W imaging. The homogeneous appearance is predominantly caused by a lack of hemorrhage, necrotic, and/or cystic changes, which is in line with previous studies [23, 28, 34]. The concentric ring sign, also known as “double layer sign,” was present in more than half of our classic type cases. This recognizable ring pattern, appearing hypoechoic on the abdominal ultrasound, in contrast to the isoechoic tumor tissue, has been predominantly mentioned in the context of the classic variant, and is hypothesized to be caused by compressed kidney tissue and dilated blood vessels [49,50,51]. Nevertheless, it does not appear to be specific to classic type congenital mesoblastic nephroma, as we also reported the characteristic in cellular and mixed cases in this study, in line with Daniel et al. [3, 52].
In case reports and small series, the cellular type congenital mesoblastic nephroma is suggested to be more heterogeneous on MRI, due to cystic, hemorrhagic, and/or necrotic components, in general showing a more aggressive growth pattern compared to the classic variant, as well as a larger size [3, 21, 23, 33, 36, 48]. Our study confirmed these findings, again stressing the difficulty to discriminate this variant from the often large, heterogeneous Wilms tumour [6, 11, 13, 21, 28, 48]. Also, this cohort of patients with cellular and mixed type congenital mesoblastic nephroma seemed to be older, indicating an overlap in age with the malignant Wilms and non-Wilms tumors [31, 34]. Nevertheless, Wilms tumors are often described as T2W hyperintense, which might indicate T2W isointensity as slightly discriminative for congenital mesoblastic nephroma in general [21, 22, 24, 53]. Rhabdoid tumors of the kidney are reported to be small, mainly T2W hypointense and often show infiltrative and aggressive features, potentially discriminating them from congenital mesoblastic nephroma as well as from Wilms tumors [44, 54]. Finally, no additional potentially discriminative MRI characteristics were identified for mixed type congenital mesoblastic nephroma, concerning both differentiation from the classic and cellular type and from other renal tumor types.
Whereas solid tumor characteristics and T1W and T2W imaging are predominantly used to identify abnormal and potentially specific characteristics of tumors, DWI and ADC values might contribute through the semi-quantification of cellularity [6, 34, 50]. Nevertheless, very limited studies have reported ADC-values of congenital mesoblastic nephroma, and conclusions are limited to the presence or absence of diffusion restriction in general [6, 48]. We showed ADC values for all subtypes to be approximately the same, with overall means ranging from 1.05 to 1.10×10−3 mm2/s, indicating moderate diffusion restriction in most tumors. ADC values around this range have also been described for clear cell sarcoma of the kidney, as well as stromal type Wilms tumor, whereas in general, more aggressive Wilms tumor subtypes show a higher diffusion restriction [44, 55, 56].
Our study has several limitations, predominantly related to its international setting and retrospective nature. While this could lead to potential information bias and variability, there was excellent interrater agreement among the included radiologists, who are experts in the field of imaging of pediatric renal tumors [44]. Also, the design of this study and related inclusion in different SIOP-RTSG protocols over the past decades affects the extent of national registration and center-specific choice of cross-sectional imaging modalities, which may have led to registration bias, potentially resulting in a disproportionate number of included patients per country, nonetheless also taking into consideration differences in population. Furthermore, in international studies, variability on the level of the patient and the MRI, reflected in the heterogeneity of reported scan parameters, has to be taken into consideration [57]. While this might not influence the reported results, it limits the possibility for statistical analysis in DWI data, given non-comparable ADC maps based on a variety of b-values [58]. Concerning clinical characteristics of the patients, this study was not designed to report on prenatal imaging or outcome, therefore lacking information on prenatal diagnoses and survival of the included patients. Also, despite the international setting of this study, numbers remained low and distribution of subtypes may not be in line with percentages reported by for instance a review by Gooskens et al., who showed a higher percentage of cellular type congenital mesoblastic nephroma (42%) [2]. Finally, statistical analysis of the discriminative value of MRI characteristics in the differentiation of subtypes of congenital mesoblastic nephroma was limited due to these relatively low numbers, while the differentiation from other pediatric renal tumors could not be analyzed based on the design of this predominantly descriptive study.




留言 (0)