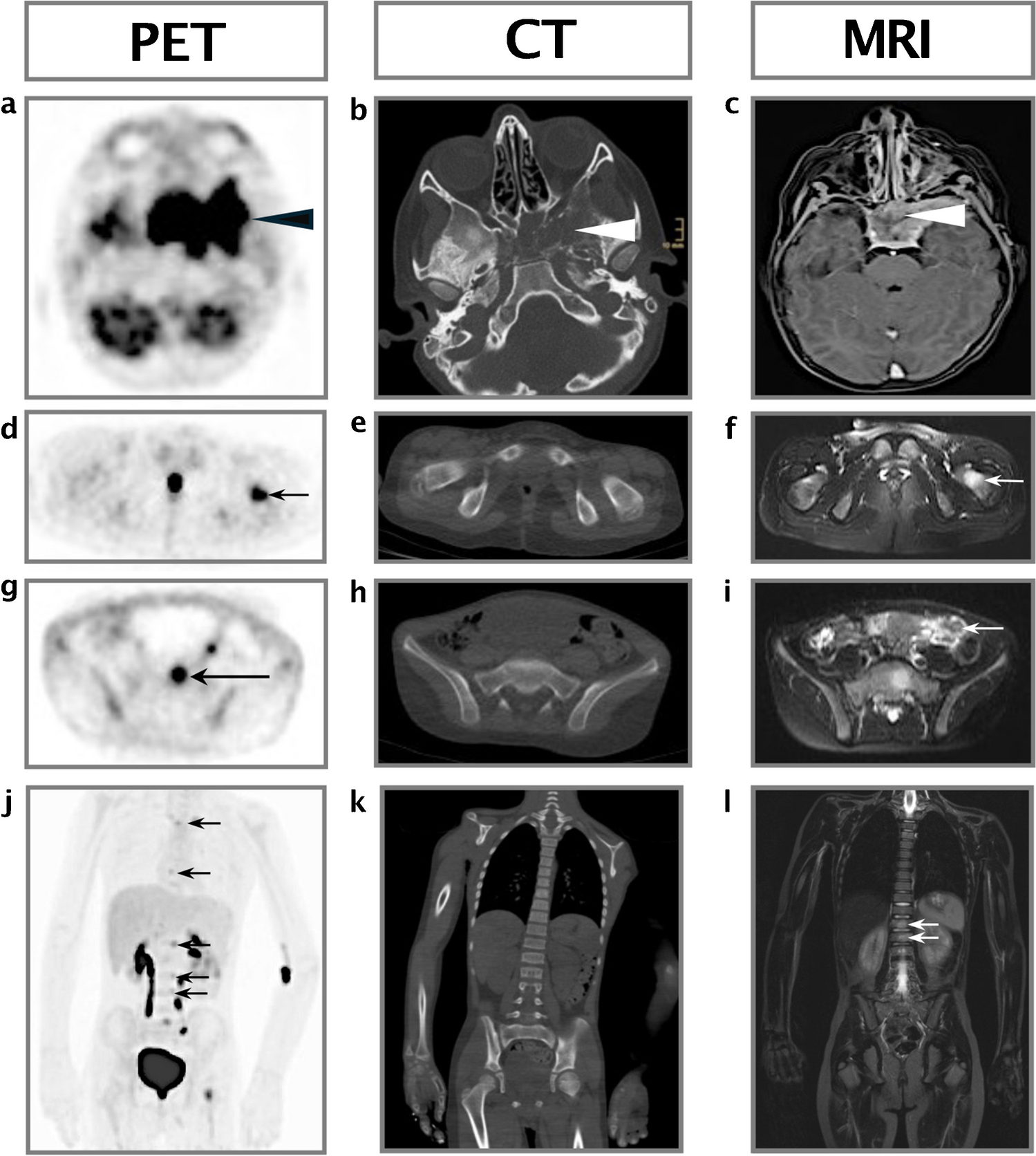
Children with suspected spondylodiscitis should be diagnosed as soon as possible so that appropriate treatment can be promptly commenced. Delay in diagnosis and treatment may cause significant neurological complications [2]. Radiographs are usually normal at onset of the disease and abnormal only 2–3 weeks into the disease [6]. Spinal MRI is the imaging modality of choice [1,2,3], and may show a narrowed disc space and blurring of the adjacent endplate borders. The vertebral bodies and disc are hyperintense on T2-weighted images, may enhance with intravenous contrast, and there may be an associated paravertebral or epidural collection [1, 2]. Fluorodeoxyglucose positron emission tomography is comparable to MRI in detecting spondylodiscitis but exposes the child to significant ionizing radiation [1, 5, 7].
The differential diagnosis may include both benign and malignant tumors (osteoid osteoma, osteoblastoma, neuroblastoma, metastasis), degenerative disorders (Scheuermann kyphosis, Schmorl nodes), and other infections (tuberculosis, brucellosis) [2]. These entities usually affect the vertebral body and spare the intervertebral space. Therefore, when MRI demonstrates direct involvement of the disc, in the appropriate clinical setting, it is pathognomonic for spondylodiscitis.
When clinical, laboratory, and imaging findings are consistent with spondylodiscitis, as in the case described here, empirical antibiotic treatment should be started as soon as possible [5, 6]. Biopsy, whether surgically or image-guided, is usually reserved for patients who do not respond to empirical antibiotic treatment [1, 2, 5].
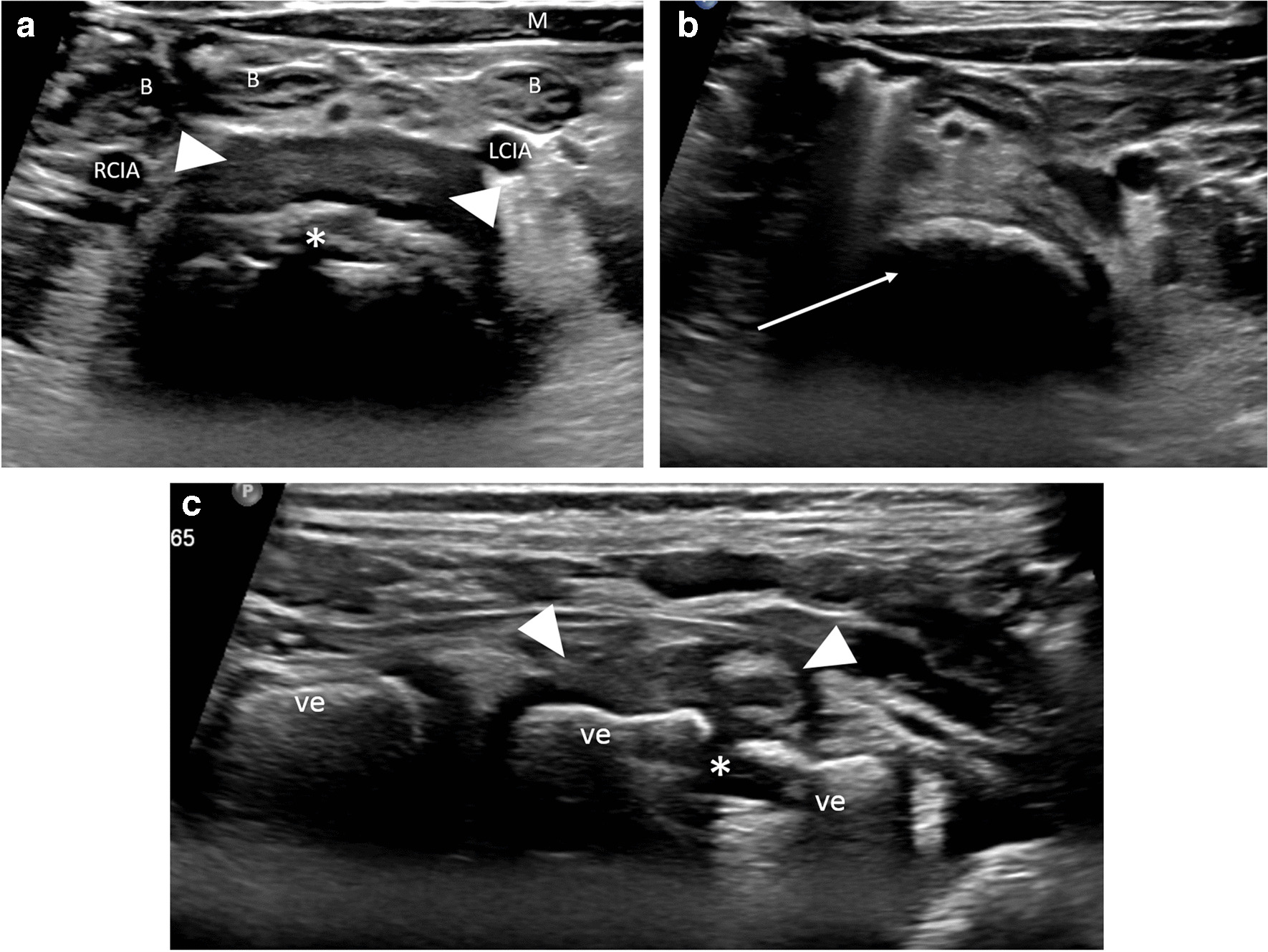
Readily available and without ionizing radiation, ultrasound is an essential tool in the management of articular and skeletal inflammatory and infectious diseases in children [8]. By identifying intra-articular fluid, bony erosion, periosteal reaction, and abscesses, sonography can assist in diagnosing septic arthritis and osteomyelitis. For certain infectious disorders, such as transient hip synovitis, it may be the only imaging modality necessary. Ultrasound is also valuable for guiding joint fluid aspiration and percutaneous biopsies and is commonly used to image the spinal contents in young infants via the posterior approach. In older infants and young children, the ossified posterior elements of the spine pose an acoustic obstacle for vertebral body, disc space and spinal contents ultrasound, and in transabdominal ultrasound, overlying bowel and pelvic organs usually mask the spinal and intraspinal structures. For these reasons, sonography is not routinely employed to diagnose or rule out spondylodiscitis. We have shown, however, that lumbar spondylodiscitis, using the anterior transabdominal approach, can be identified by sonography in young children.
Sonographers and radiologists, in both pediatric and musculoskeletal fields, should be acquainted with the sonographic features of lumbar spondylodiscitis, whether as an incidental or an intentional finding.




留言 (0)