Explanation for the choice of comparators
For evaluating the effect of knowing the BDNF -87 methylation status the best way forward is to compare the remission rate and the AE rate in the marker group (treating physicians and patients know the marker status) with a group of patients, who receive TAU (treating physicians and patients not knowing the marker status). In the TAU group, patients and physicians will select subsequent treatments based on national guidelines and the physician’s experience, following the common practices on the ward.
Intervention description
For more details, please see the “Trial design ” section. The BDNF CpG -87 marker stands out as the initial predictive indicator for non-responsiveness to monoaminergic antidepressants, making it unique with no established gold standard or comparator. Within the study protocol, no specific treatment protocol is provided, allowing the marker to be tested under real-world conditions.
Criteria for discontinuing or modifying allocated interventions
Given that there is no study drug intake or intervention involved, aside from the knowledge of the marker status, discontinuation of allocated interventions will not be required during the diagnostic trial.
Strategies to improve adherence to interventions
In the current study, study nurses, physicians, and psychologists will monitor inpatients on a weekly basis until the follow-up period. Consequently, patients will benefit from additional attention and care from the study team to ensure adherence to the study protocol.
Relevant concomitant care permitted or prohibited during the trial
This intervention occurs within a real-world setting, and as such, no concomitant care or interventions are excluded.
Provisions for post-trial care
No provisions for post-trial care are provided, as there is no anticipated risk of harm associated with the patient’s participation in the study. Nonetheless, patients are covered by insurance under an accident insurance policy.
Compensation
Participating patients are not receiving any form of compensation.
Patient and public involvement
Patient participation is a crucial component of the study as it allows the research consortium to address and respond to the needs and concerns of patients regarding the novel biomarker-based treatment approach. By involving patients, prejudices, and misconceptions can be thoroughly discussed and directly addressed during the recruitment process and communication of study findings. In the project’s initial year, the German Depression Foundation (GDF) will conduct a quantitative study to evaluate the beliefs, opinions, knowledge, barriers, and concerns surrounding the use of blood-based biomarkers to guide treatment decisions for depression. This assessment will encompass patients with MDD as well as the general population. The obtained results will serve as a basis for developing informative materials that will be provided to participating patients, as well as for guiding ongoing training for all participating medical doctors, focusing on essential considerations when offering the use of blood-based biomarkers. Through collaboration with the German Alliance Against Depression, the GDF will engage a Patient Advisory Board (PAB) that will be involved in all stages of the proposed study. The PAB’s responsibilities will include, among others, contributing to the design of the quantitative study, shaping information materials, discussing interim study findings, and reviewing public releases based on their expertise and lived experience. By participating in the project’s activities, patients will be enabled to engage in important processes related to their individual health and well-being. Active PAB members will also receive a small monetary allowance for their contribution, and their travel expenses will be reimbursed.
Outcomes Primary outcome
Two co-primary endpoints are used for evaluating the predictive value of BDNF -87 methylation. The 1st co-primary endpoint is the rate of patients achieving remission during therapy, defined as a score of ≤ 10 on the Hamilton Depression Rating Scale (HDRS-24) on day 49 (± 3). The HDRS-24 is commonly used in clinical trials for depression and remission is considered the most relevant outcome for patients. Achieving remission indicates a higher likelihood of full recovery, improved quality of life, and reduced risk of experiencing a chronic-recurrent form of depression. This endpoint focuses on the absence of residual symptoms rather than just a partial response.
The 2nd co-primary endpoint is the rate of AEs. For evaluating AEs an extended version of the DOTES is used on a weekly basis. If a patient has at least one AE with an intensity of three within the time interval of 49 (± 3) days, it is counted for the co-primary endpoint.
Participant timeline
During BL, patients will undergo a short-structured interview using the MINI-DIPS (Mini Diagnostic Interview for Mental Disorders) to screen for mental disorders. The chapter on MDD from the Diagnostic Interview for Mental Disorders (DIPS) will be used to characterize the symptoms of depression further. Demographic information, such as sex, age, education, and employment, will also be recorded.
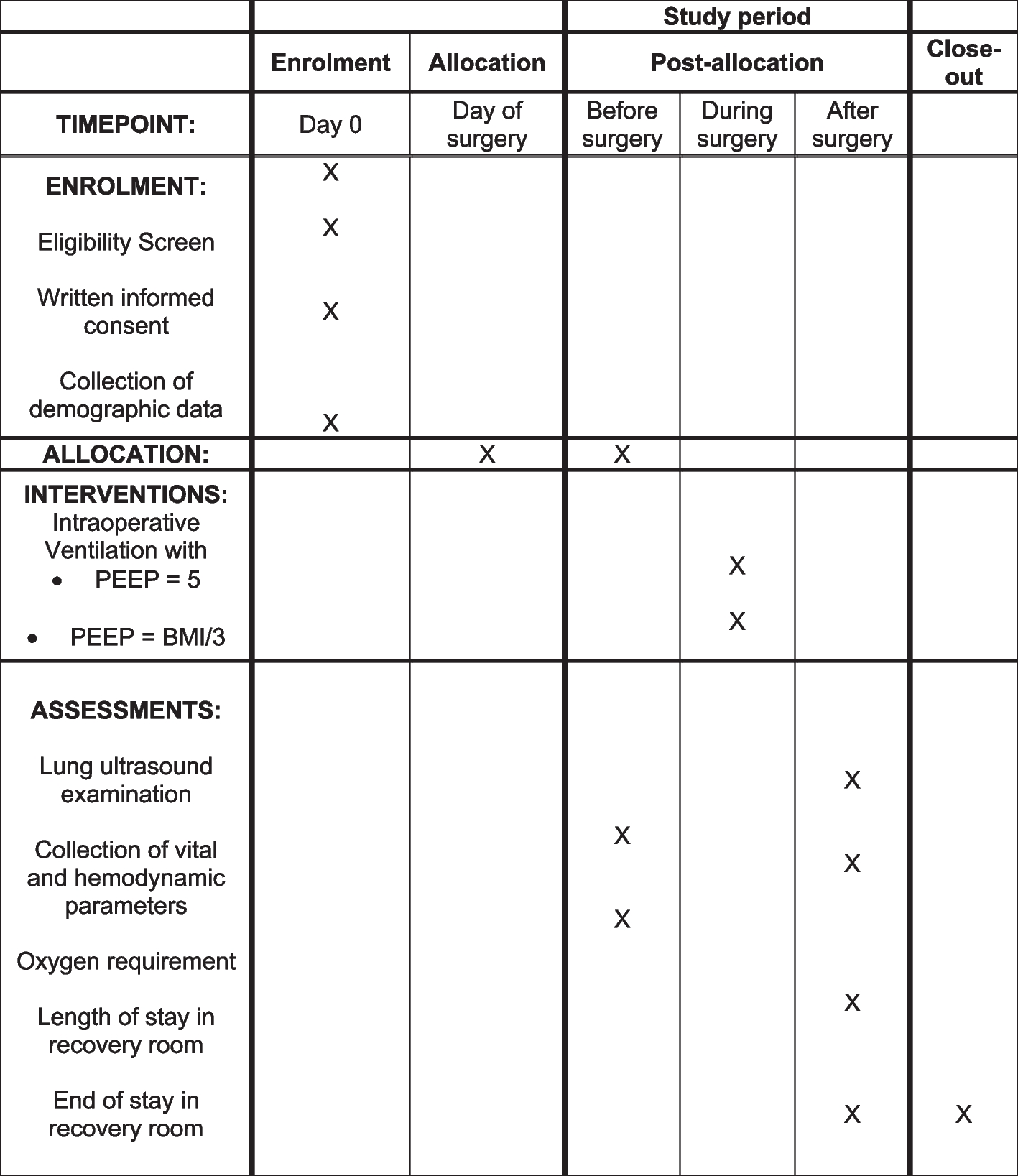
Routine blood work, including inflammation markers, lipid markers, and vitamin status, will be performed at baseline and on day 49 (± 3). Medication intake, symptom severity (assessed using MADRS and HDRS-24), and DOTES will be assessed weekly. The BDI-II will be administered biweekly according to the instructions provided (Table 2).
Table 2 Overview of examinations during the BDNF trialSample size
To calculate the required sample size for the study, assumptions regarding the prevalence for biomarker-positive patients, as well as the rates for the co-primary endpoints in both treatment groups, must be established.
1st co-primary endpoint (remission rate)
Based on the studies by Tadic et al. [17] and Lieb et al. [18], the prevalence of biomarker-positive patients and the remission rate (dependent on the biomarker status) were estimated. Due to the different sample sizes of both studies (Tadic et al.: n = 39 and Lieb et al.: n = 146), an overall rate was calculated using weighting. Tadic et al. (unpublished data) reported a biomarker-positive rate of 0.38, while Lieb et al. reported a rate of 0.58, resulting in a weighted rate of 0.54. Furthermore, Lieb et al. observed a remission rate of 0.45 for biomarker-positive patients, and Tadic et al. observed a rate of 0.4, leading to a weighted rate of 0.41. For biomarker-negative patients, Lieb et al. reported a remission rate of 0.09, and Tadic et al. reported a rate of 0.23 resulting in a weighted rate of 0.19. Based on these empirical data, the following assumptions were made for the planned study:
1.
Rate for biomarker-positive patients: 0.5
2.
Remission rate for biomarker-positive patients: 0.4
3.
Remission rate for biomarker-negative patients: 0.2
To test for non-inferiority of the remission rate, an equal remission rate of 0.30 in both treatment groups is assumed for sample size calculation. This is derived from the 50:50 ratio of biomarker-positive and biomarker-negative patients, averaging the rates described in points 2 and 3. A two-sided 5% significance level and a non-inferiority margin of − 0.2 (favoring the TAU group) are employed for sample size calculation. Based on these assumptions, a sample size of 222 patients, allocated equally (1:1 allocation ratio) between the treatment groups, is required to achieve 90% power to reject a remission rate difference (marker − TAU group) of less than − 0.2. Selecting a non-inferiority margin of 20% ensures sufficient precision, as demonstrating a significant reduction in AEs (the second co-primary endpoint) is crucial for establishing treatment success.
2nd co-primary endpoint (AE rate)
In a meta-analysis conducted by [21], which examined the efficacy of SSRIs and the incidence of AEs based on placebo-controlled studies, the median AE rate was 0.8 in the treatment group. In this trial, it is assumed that knowing the marker status will result in a reduced use of antidepressants, leading to fewer AEs during pharmacotherapy. Conservatively, it is assumed that the AE rate will be half in the biomarker-negative group compared to the rate in patients treated with antidepressants (AE rate in antidepressant-treated patients: 0.8, AE rate in patients not treated with antidepressants: 0.4). Therefore, it is assumed that the AE rate in the marker group is 0.6, calculated as the mean of the expected AE rates stated. Since all MDD patients in the TAU group receive antidepressant treatment, an AE rate of 0.8 is assumed. A sample size of 218 achieves 90% power to detect a rate difference of − 0.20 (marker − TAU group) for the assumed AE rates, with a one-sided type I error of 2.5%.
To demonstrate the value of knowing the marker status for both co-primary endpoints with sufficient robustness, the final sample size was determined based on the 1st primary endpoint, which requires a larger sample size (n = 222 vs. n = 218). To compensate for potential treatment effect reduction due to study dropouts, the sample size is increased by 15% to ensure a conservative sample determination (n = 256). Sample size calculation was performed with nQuery 9.3.
Recruitment
Patient recruitment occurs within the larger multicenter cohort study “P4D—Personalized, Predictive, Precise & Preventive Medicine for Major Depression” (for additional information, refer to the German Clinical Trial Register (DRKS) ID: DRKS00032215). Briefly, individuals diagnosed with depression will undergo screening upon admission to a psychiatric ward at any of the five participating university hospitals.




留言 (0)