
記住我
Based on a priori sample size calculation done in G*Power 3.1, we needed to include 52 participants in order to find an interaction effect with medium effect size using a repeated measures ANOVA test with alpha 0.05 and power 0.80. Taking into account the possibility of drop-outs, seventy older adults were included in the study. Participants were eligible for the study if they: (1) were 60 years and older; (2) were not currently on psychopharmacological medication or had used these types of drugs in the last five years; (3) voluntarily participated in the study; (4) were fluent in Lithuanian language; (5) were not regularly participating in any exercise program during the previous six months.
Exclusion criteria were: (1) musculoskeletal disorders, especially of the lower extremity hindering participation in the exercise group; (2) neurological disorders such as previous brain injuries, stroke, multiple sclerosis, epilepsy, or neurodegenerative diseases, or a Montreal Cognitive Assessment (MoCA) score below 16/30 indicating possible undiagnosed dementia [22]; (3) psychiatric disorders such as depression or alcohol or drug abuse in the last five years; (4) diabetes mellitus; (5) deep vein thrombosis; (6) oncologic diseases or history of chemotherapy use; or participants that were not allowed or able to undergo magnetic resonance imaging (MRI) based on the exclusion checklist provided by the Department of Radiology, Lithuanian University of Health Science. MR data collected in the study are not presented in this article. For MRI results, see Vints et al., 2022, 2023 [23, 24]; Sheoran et al., 2023 [25]; Valatkeviciene et al., 2023 [26]; and Levin et al., 2023 [27].
Participants were recruited and continuously enrolled between July 2020 and July 2021 via presentations in local community organizations and contacting candidates from a list of patients provided by general practitioners. Interested individuals were invited to Saules Family Medical Centre, where the study's goals, objectives, and methodology were explained in detail. Participants gave written consent prior to study enrolment. The protocol was approved by the Kaunas Regional Biomedical Research Ethics Committee (No. BE-10–7). All participants signed an informed consent form prior to their inclusion in the study.
Study designWe conducted a single-blinded, two-arm randomized controlled trial with a 12 weeks intervention with lower body resistance exercises at the Institute of Sports Science and Innovation, Lithuanian Sports University. Randomization was performed using a stratified 8-blocked randomization process, stratifying by MoCA score (below 26/30 and 26–30/30), so that each block contained two participants with low MoCA score (i.e., MoCA < 26) and two participants with high MoCA score (i.e., MoCA ≥ 26) allocated to the control group, and two participants with low MoCA score and two participants with high MoCA score allocated to the experimental group. The random allocation was accomplished in an Excel spreadsheet using a random number generator set to indicate either 1 or 2 for the exercise or control group. If two participants from the same group were in a block (N) of four participants with the same cognitive status, a third participant with the same cognitive status and allocated to the same group was assigned to block N + 1. The final block of eight participants included only participants at high risk of MCI, and seven were assigned to the control group. We took this decision to correct for the higher number of drop-outs in the control group participants with high risk of MCI at the beginning of the project. The reason for the difference in number of drop-outs most likely existed because participants allocated to the control group were less motivated to return for follow-up assessments. Assessors of the outcome measurements were blinded for the allocation of the participants to the experimental or control group. The participants were not blind to their group allocation.
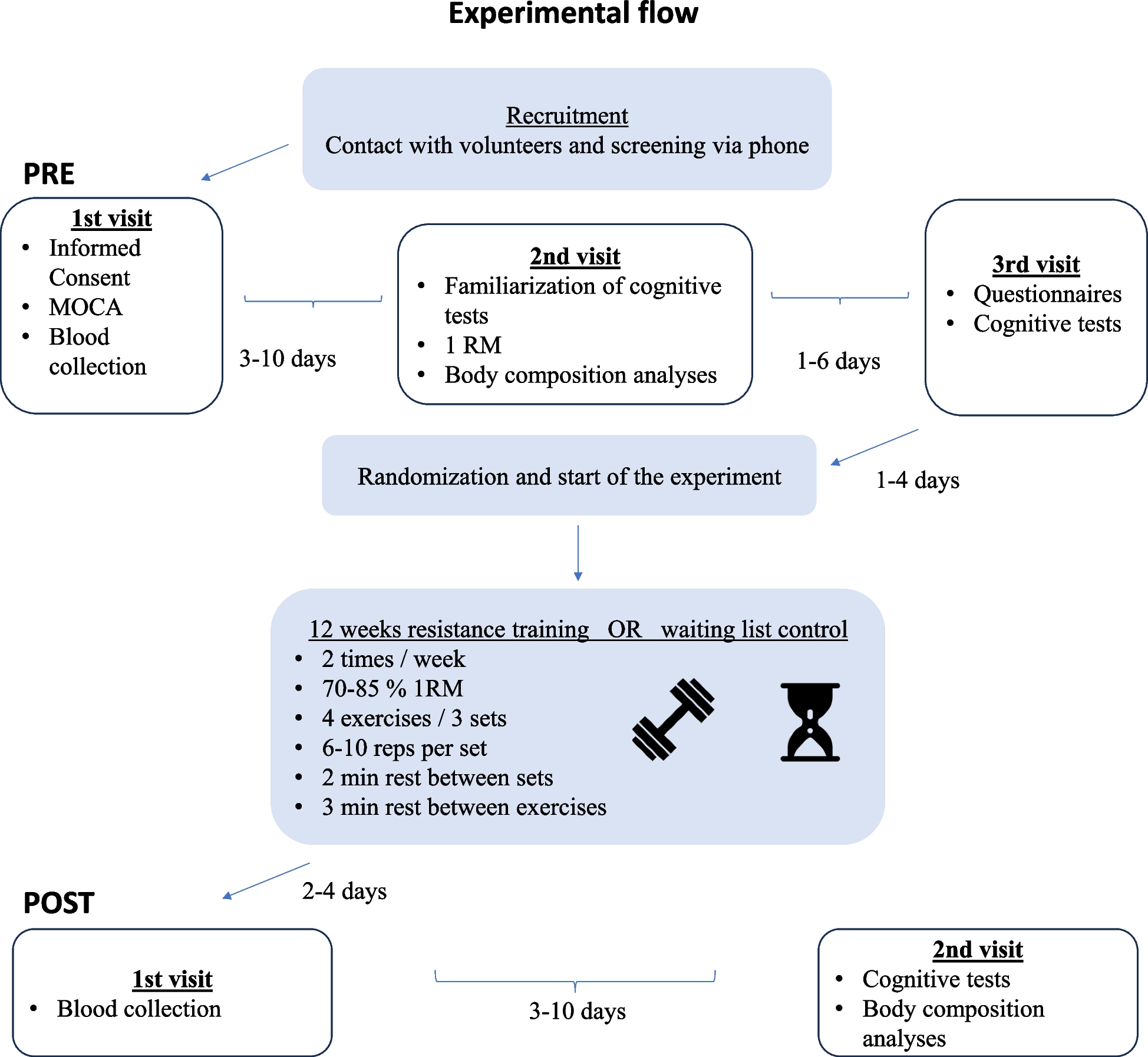
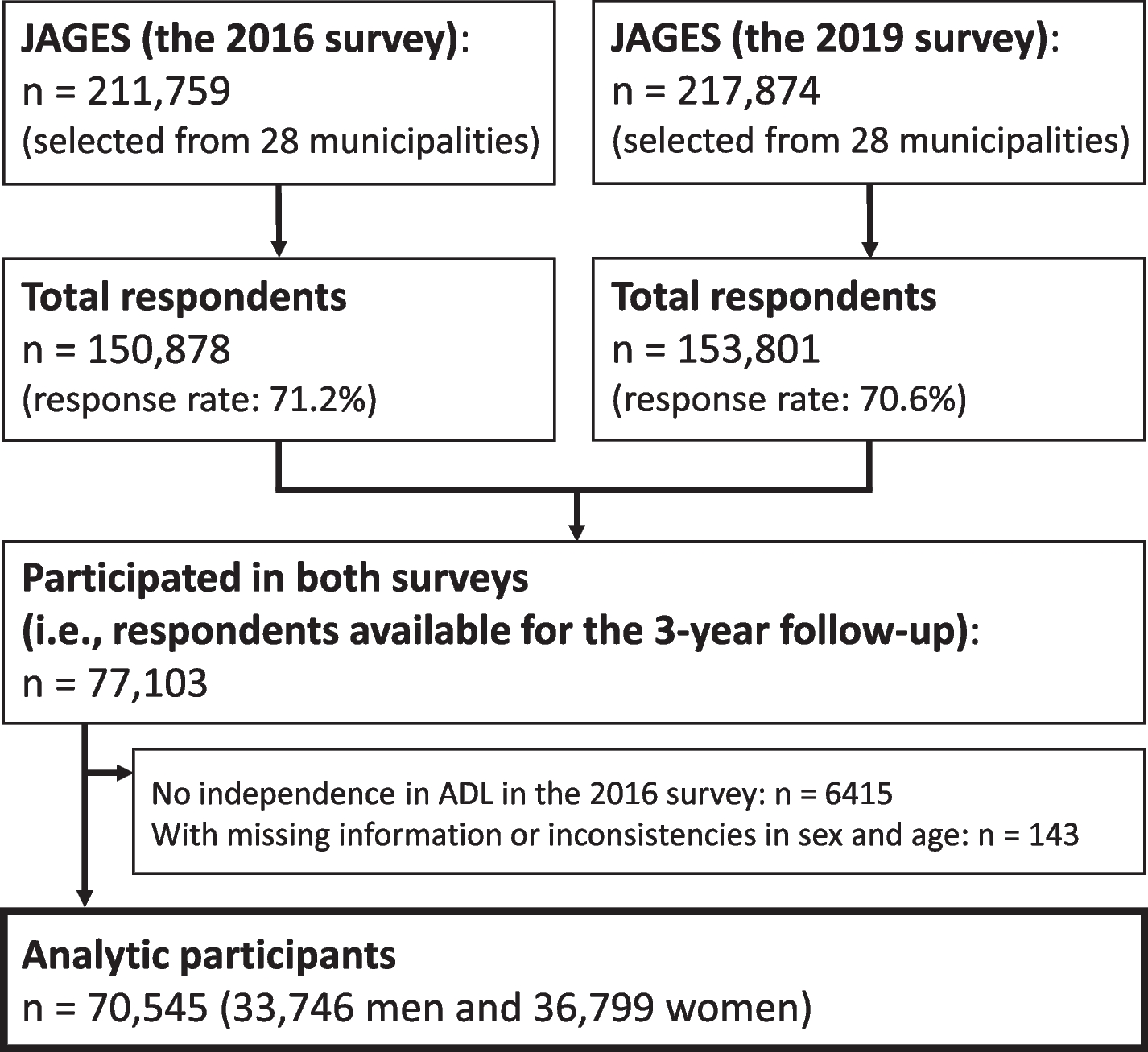
The experimental group underwent 12 weeks of resistance exercise training, while the control group underwent no intervention. Participants from both groups were instructed to continue their daily life routines as usual. Following a cognitive screening with the MoCA test in the Saules Family Medical Center in Kaunas, Lithuania, participants were invited twice on separate days for additional testing at the Lithuanian Sports University in Kaunas, Lithuania. For each participant, the same test conditions were provided at the same time of day (8 am to 11 am) before and after the 12 weeks period. All participants were instructed to avoid unusual physical activity, alcohol, and caffeine intake the day before testing and to sleep at least 7 h. They were asked to have breakfast at least 1–2 h before the experiment. During the first testing day, participants reported their demographic and medical characteristics (see Sect. " Demographic and medical characteristics"). All assessments (see Sect. " Physical activity assessment"-" Blood sampling") were performed before and after the 12 weeks intervention or control condition. See detailed description of the study procedure in Fig. 1 and participant flow diagram in Fig. 2.
Fig. 1
Experimental flow chart. Abbreviations: MOCA, Montreal Cognitive Assessment; RM, repetition maximum
Fig. 2
Participant flow diagram. Please note that some participants enrolled in this project were excluded or dropped-out because of MRI scanning, while no MRI results are presented in this paper. Abbreviations: MCI, Mild cognitive impairment; MRI: Magnetic resonance imaging
Demographic and medical characteristicsAll participants completed a questionnaire battery that assessed their demographic and medical characteristics, such as age, sex, educational level, and smoking status. Educational levels were categorized as primary, secondary, or higher education.
Physical activity assessmentPhysical activity level was assessed using the IPAQ-SF. This self-report questionnaire comprises seven questions and four intensity levels of activity: 1) vigorous-intensity activity such as aerobics, 2) moderate-intensity activity such as leisure cycling, 3) walking, and 4) sitting [28]. Each activity type's frequency (days per week) and duration (minutes per day) in the last seven days are recorded. Each type of activity is characterized by METs (metabolic equivalent of task), and total IPAQ score is estimated by adding up the calculated MET-minutes within each physical activity intensity level (vigorous intensity = 8.0 MET, moderate intensity = 4.0, walking = 3.3 MET). Participants that indicated to burn less than 600 kcal/week are defined as sedentary, 600–3000 kcal/week as moderately physically active, and more than 3000 kcal/week as highly physically active.
Body composition analysisBody weight (in kg), height (in cm), body fat percentage (fat %), and body mass index (BMI, in kg/m2) were measured before and after the intervention. Weight and fat% were estimated using leg-to-leg bio-impedance analysis (BIA, Tanita TBF-300-A).
Maximum voluntary knee extension forceThe maximum voluntary contraction (MVC, in Newton meters) of isometric knee extension torque of the dominant leg was measured with Biodex System 3 dynamometer (Biodex Medical Systems, NY, USA). The highest MVC value out of two trials was recorded.
Neurocognitive assessmentsMoCA testA MoCA examination was conducted by a mental health care professional to evaluate cognitive abilities. This test is considered reliable and consists of 12 items that assess seven cognitive domains, including visuospatial ability and executive functioning, naming, memory, attention, language, abstract reasoning, and orientation. All items contribute to a total score of up to 30 points, with a higher score indicating stronger cognitive functioning. One point is added to the total score if the participant had less than 13 years of education. The participants were classified into different groups based on their MoCA test scores, with a cutoff score of 26 being used for stratification. It is worth noting that a MoCA test score of 25 or lower is generally considered indicative of a high risk of MCI in an otherwise healthy geriatric population [22].
ANAM testSpecific cognitive domains were tested with four selected tests of the ANAM4 (Automated Neuropsychological Assessment Metrics, version 4) test battery. The ANAM4 test system consists of a library of 28 computer-based self-administered tests that assess different aspects of neurocognition including executive functions and attentional processes. Since maintaining attention, inhibitory control, basic computational skills, and working memory are crucial for independent daily living in older adults, we have selected specific subtests to evaluate these functions before and after the intervention. These subtests comprised two-choice reaction time, Go/No-Go, mathematical processing, and memory search tasks. Subjects completed the cognitive tests using a Lithuanian Sports University (LSU) computer running the test suite software in a quiet environment. The software automatically provides the already averaged results of each test. Outcome measure was the response time (in milliseconds, ms). Accuracy measures were used to exclude trials with more than 50% incorrect responses, as this may indicate that the subject did not understand the task. We decided also to delete response times that were faster than the best percentile of young male college students, based on normative values presented in the ANAM4 user manual, considering that this likely indicates that the participants did not adequately perform or understand the task and attained the 50% correct responses by chance [29]. However, none of the participants ‘ results had to be excluded based on this decision. A familiarization session took place 48-72 h before the testing day and on the testing day the participants were allowed one practice trial before the results were being recorded.
2-choice reaction time testWe used this test to assess processing speed and alternating attention. It contains a motor speed component. The 2-choice reaction time test measures choice reaction time by presenting the participant with a "*" or "o" on the screen. The individual is instructed to respond as quickly as possible by pressing the left or right mouse button as soon as the stimulus appears.
Go/No-go testIt is used to assess response inhibition. The participant is presented with two characters, “o” and “x” and needs to respond as quickly as possible to the “x” character each time the stimulus appears. The subject is instructed to do nothing when the character “o” appears (inhibit response).
Memory search testThe results of the memory search test are used as an index of attention, immediate recognition, and verbal working memory. The program uses letters and symbols to assess verbal working memory as symbolic and non-verbal subparts. The user sees a positive memory set of four letters on the screen (e.g., “T B Q U”). Then, individual characters are displayed, and the participant needs to press mouse buttons to indicate if each character is or is not a member of the positive memory set.
Mathematical processing testThe mathematical processing test results are used as an index of concentration, working memory, and computational skills. During the test, the participant needs to solve an arithmetic problem (e.g., “4 + 8–5 = ”). The task involves only three single-digit numbers and two operators. The subject needs to indicate whether the answer is less or higher than five.
Blood samplingSerum IL-6, KYN, and IGF-1 concentrations were measured using the ELISA method (ELISA, Biotek, model ELX 800) with spectrophotometry (Spark 10 M, Tecan Group Ltd. Zürich, Switzerland) by an experienced technician. A nurse drew the venous blood samples from the antecubital vein into 5 mL EDTA-K3 vacuum tubes. All blood samples were collected between 9:00 a.m. and 1:00 p.m. The second blood collection was carried out 2 to 4 days after the last exercise session for participants in the experimental group. The tubes were gently inverted 8–10 times immediately after blood collection and kept at room temperature for no more than 30–35 min until centrifugation for 15 min at 4,000 g centrifugal force. Subsequently, serum was aliquoted into 1.5 mL polypropylene tubes. The serum samples were frozen immediately after serum separation and kept at -80 °C in the freezing room of the LSU Institute of Sports Science and Innovation laboratory until further examination.
The IL-6 ELISA kit was purchased from DIAsource ImmunoAssays S.A., Belgium (KAP1216). The lower detection limit is 2 pg/mL. The KYN ELISA kit was purchased from MyBiosource, Inc., USA. The lower detection limit is 45.7 ng/mL. The IGF-1 ELISA kit was purchased from IBL International, GMBH, Germany (MD58011). The lower detection limit is 0.03 ng/mL.
Training interventionRT intervention was conducted over 12 weeks in the Lithuanian Sport University gym in accordance with the National Strength and Conditioning Association (USA) position statement on resistance training for older adults [30]. Two to ten days prior to the exercise intervention, participants were familiarized with the RT procedure and underwent 1-repetition maximum (1RM) testing. Two resistance training sessions were scheduled per week with a minimum of two days apart. Warm-up consisted of 5-min cycling on a cycle ergometer at an intensity (in Watts) approximately equal to the participant’s body weight in kilograms, followed by a few dynamic stretching and activation exercises including lunges, butt kicks, side step lunges, half-squats, and front and side cross swings. The training program comprised four exercises, namely knee extension (1), incline leg press(2), hamstring curls (3), and calf raise (4), using resistance training equipment from Technogym (Italy).
Each exercise was performed for 2–3 sets of 6–10 repetitions, at 70–85% of the baseline 1RM, with a 2-min rest between sets and a 3-min rest between exercises. From week 1 to 3, participants did 8–10 repetitions, starting at 70–75% 1-RM; from week 4 to 9, they worked 6–8 repetitions, starting at 75–80% 1-RM; and from week 10 to 12, they did six repetitions starting at 80–85% 1-RM. After the first session and during each of the three training blocks the weight was adjusted according to the participants’ rate of perceived exertion (RPE) on a 10-point Borg scale. The weight was increased when the older adult indicated a score below seven on ten. The exercise sequence was periodically randomized. Qualified trainers supervised all training sessions.
Statistical analysisIBM SPSS Statistics version 27 (IBM Corp., Armonk, NY) was used to perform all analyses. Data were initially inspected for outliers and normality. Extreme outliers were defined as values lying more than 3 × the interquartile range away from the median and were excluded. Normality was checked graphically using PP-plots and histograms and numerically by a kurtosis and skewness measure between -2 and + 2. If the normality assumptions were not met, data was log transformed. Homoscedasticity was tested with the Levene’s test.
First, independent t-tests and Chi2 tests (or Fisher Exact tests, if the expected count in any of the cells was below 5) were used to assess group differences in baseline variables for continuous and categorical variables respectively. Two-way ANCOVA was used with either post-intervention blood biomarker levels or ANAM test results as a dependent variable. Group (experimental versus control) and cognitive status (low MCI risk versus high MCI risk) were entered as fixed factors, and age and pretest values of the dependent variable as covariates. Body fat % was entered as an additional covariate for analysis with IL-6 or KYN levels. We chose this approach instead of a three-way repeated measures ANOVA, because it was demonstrated that ANCOVA tests taking into account the pretest value of the dependent variable by entering it as a covariate in the model, rather than as a level of the time factor in repeated measures ANOVA, reduce the population error variance and are therefore more powerful and precise [31]. Bivariate correlation R-values were calculated between the pre- to post-intervention changes in blood biomarker levels and ANAM test results for total group and experimental group. Spearman’s rho was chosen, because of the non-normal distribution of some of the outcome measures. Statistical significance was accepted at α = 0.05.
留言 (0)