
記住我



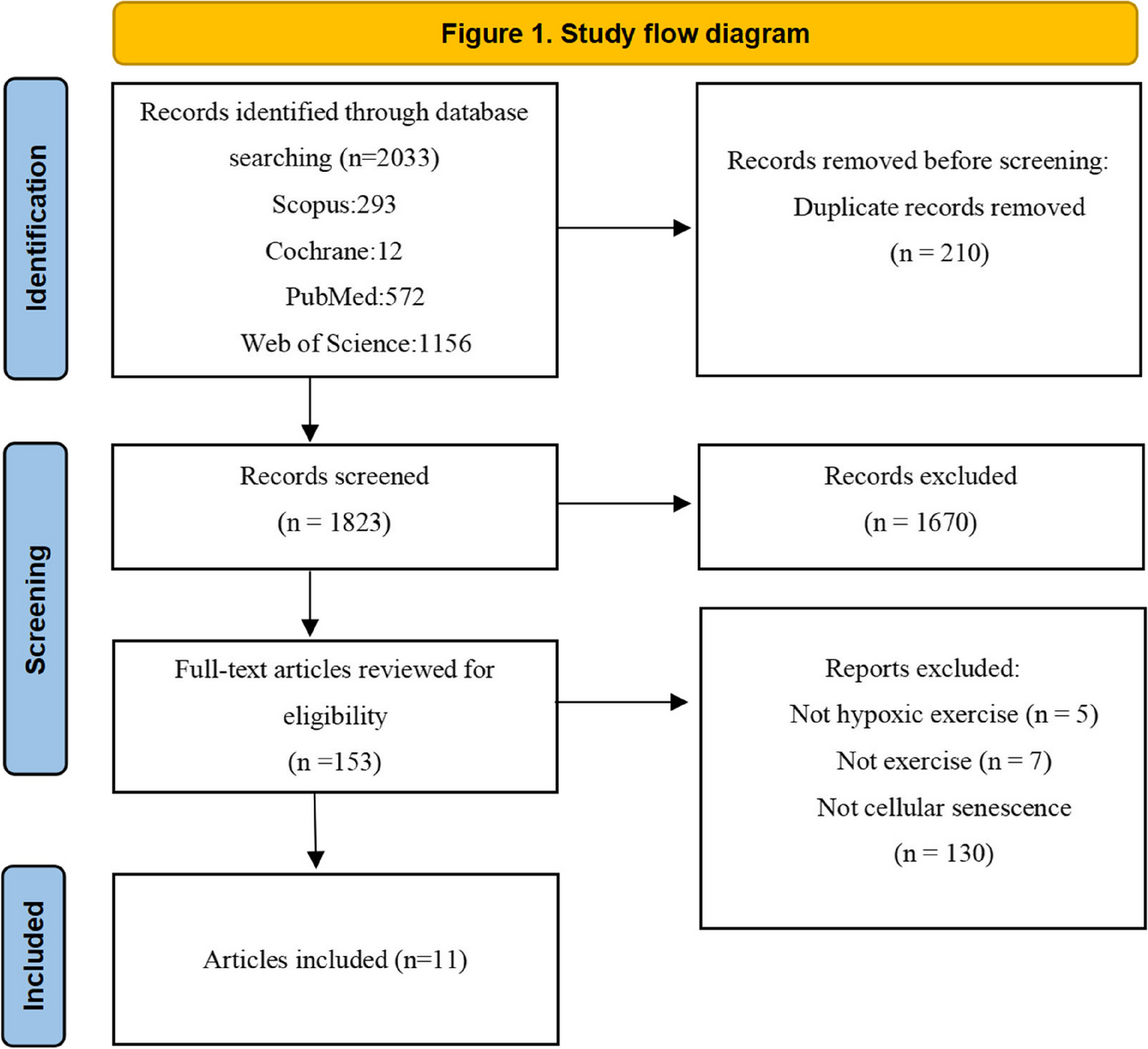




Figure 1 depicts a flow diagram of the study participants. We conducted a population-based 3-year longitudinal study in Japan using data from the Japan Gerontological Evaluation Study (JAGES). The JAGES is an ongoing cohort study exploring social, environmental, and behavioral factors related to the loss of health with regards to functional decline or cognitive impairment among older adults [11, 12]. Self-reported questionnaires were mailed to community-dwelling adults aged ≥ 65 years who were sampled from 28 municipalities, including metropolitan, urban, semi-urban, and rural communities from 14 prefectures in Japan as far as Hokkaido (the northernmost prefecture) and Kyushu (the southernmost region), between October and November 2016 (the 2016 survey) and between November 2019 and January 2020 (the 2019 survey). Both surveys were administered to all eligible residents in the 11 small municipalities and using random sampling in the 17 large municipalities. In the 2016 survey, the questionnaires were mailed to 211,759 people, with 150,878 of them responding (response rate: 71.2%). Likewise, in the 2019 survey, of the 217,874 people approached, 153,801 (70.6%) responded to the questionnaire. Out of the 77,103 respondents who participated in both surveys, 6415 people who had no independence in activities of daily living in the 2016 survey and 143 who had missing information or inconsistencies in sex and age data were excluded from the study.
Fig. 1
Flow diagram of the study participants. JAGES: Japan Gerontological Evaluation Study; ADL: activities of daily living
For the present study, we used data from 70,545 eligible respondents (33,746 men and 36,799 women). The mean age was 73.1 ± 5.5.
Multidimensional frailty score: Kihon Checklist (KCL)The KCL is a simple self-reported survey developed by the Japanese Ministry of Health, Labour and Welfare to identify older adults at risk of requiring care/support. It consists of 25 questions regarding instrumental (3 questions) and social (4 questions) activities of daily living, physical functions (5 questions), nutritional status (2 questions), oral function (3 questions), cognitive function (3 questions), and depressive mood (5 questions) [13, 14]. With question being worth one point, the total score ranges from 0 to 25, and a higher score indicates greater frailty. The area under the receiver operating characteristics curves for the evaluation of frailty using the KCL was 0.81 for prefrailty and 0.92 for frailty [14]. Another study reported that with higher total scores, the risk of future functional decline and mortality increased proportionately [15].
Participation in different types of group sports and exercisesAt first, participants were asked about their frequency of sports club or group participation; those who participated at least once a year were further asked “what type of sports do you currently do in those clubs or groups (multiple answers possible)?” Possible responses for this question included 1) walking, 2) running and jogging, 3) fitness exercises, 4) weight exercises, 5) hiking, 6) golf, 7) ground golf, 8) gateball, 9) dance, 10) yoga, 11) aerobics, 12) petanque, 13) Tai Chi, 14) swimming, 15) aquatic exercises, 16) table tennis, 17) bowling, 18) bicycling, 19) tennis, and 20) other sports [5]. We also created a dichotomized variable for whether or not they participated in any of these types.
Fitness exercises are low-to-moderate-intensity exercises, such as calisthenics and seated exercises, which mainly focus on health promotion and social interaction. Ground golf, a new kind of golf that simplifies the golf game to promote lifelong sports, is widely popular among older adults in Japan [16]. Gateball, a team sport that originated in Japan, entails competing for points by hitting a ball against a target using a stick [17]. The details of the rules of these sports and how to play them are presented in the respective articles.
CovariatesWe evaluated different variables, which are reportedly associated with sports group participation in older adults, for their potential confounding effect on the association between group participation and frailty [18]. The effect of sex was controlled by conducting a stratified analysis. Data on the following variables were collected: age group (65–69, 70–74, 75–79, 80–84, and ≥ 85 years), marital status (married or unmarried), living alone (no or yes), occupational status (employed, retired, or never employed), number of years of education (≥ 13, 10–12, or < 10 years), alcohol consumption status (none, past, or current), and smoking status (none, past, or current). Self-rated health was measured by a 4-point Likert scale: very good, good, somewhat poor, or poor. Each participant’s annual equivalent income was calculated by dividing the household income by the square root of the number of household members and categorized into three groups: ≥ $40,000; $20,000–$39,999; or < $20,000 per year (1 dollar = 100 yen). Each participant’s disease status was assessed with “yes” or “no” responses and included hypertension, stroke, cardiovascular disease, diabetes mellitus, hyperlipidemia, musculoskeletal disorders, and cancer.
Statistical analysisWe calculated descriptive statistics by sex. Linear regression analyses were performed to examine the association between the type of sports and exercise groups in the 2016 survey and the change in the frailty score from 2016 to 2019 (i.e., values obtained by subtracting the total KCL score in 2016 from that in 2019). The calculated change in score was approximately normally distributed and met one of the assumptions for the application of linear regression. The homogeneity of variances and linearity were likely to be acceptable in the large sample used in the present study. The unstandardized coefficient (B) with its 95% confidence interval (95% CI) was calculated individually for men and women. We then examined the interaction between each type and sex to investigate whether the association with changes in the frailty score differed according to sex. In these regression analyses, we conducted multivariate adjustment using an inverse probability weighting (IPW) method as the tool to adjust for differences between the two groups (i.e., participation or non-participation in each type of sport and exercise group) [19]. To adjust for the between-group differences in participant characteristics “Covariates” section), we developed propensity scores to estimate the probability that older adults would participate in each type of sport and exercise group by conducting a logistic regression analysis. This ensures a balanced approach and involves weighting each participant in each group by the inverse of the probability that they would participate in the group and weighting each participant who did not participate in the group by the inverse of the probability that they would not participate in the group. Additionally, we imputed incomplete variables using a multivariate normal imputation method. We created 20 imputed datasets using all variables introduced in the current analyses, after which the estimated parameters were combined using Rubin’s combination methods [20, 21]. We used Stata/MP version 17.0 (StataCorp, College Station, Texas, USA) for all statistical analyses, with the statistical significance set at P < 0.05.
留言 (0)