Study design
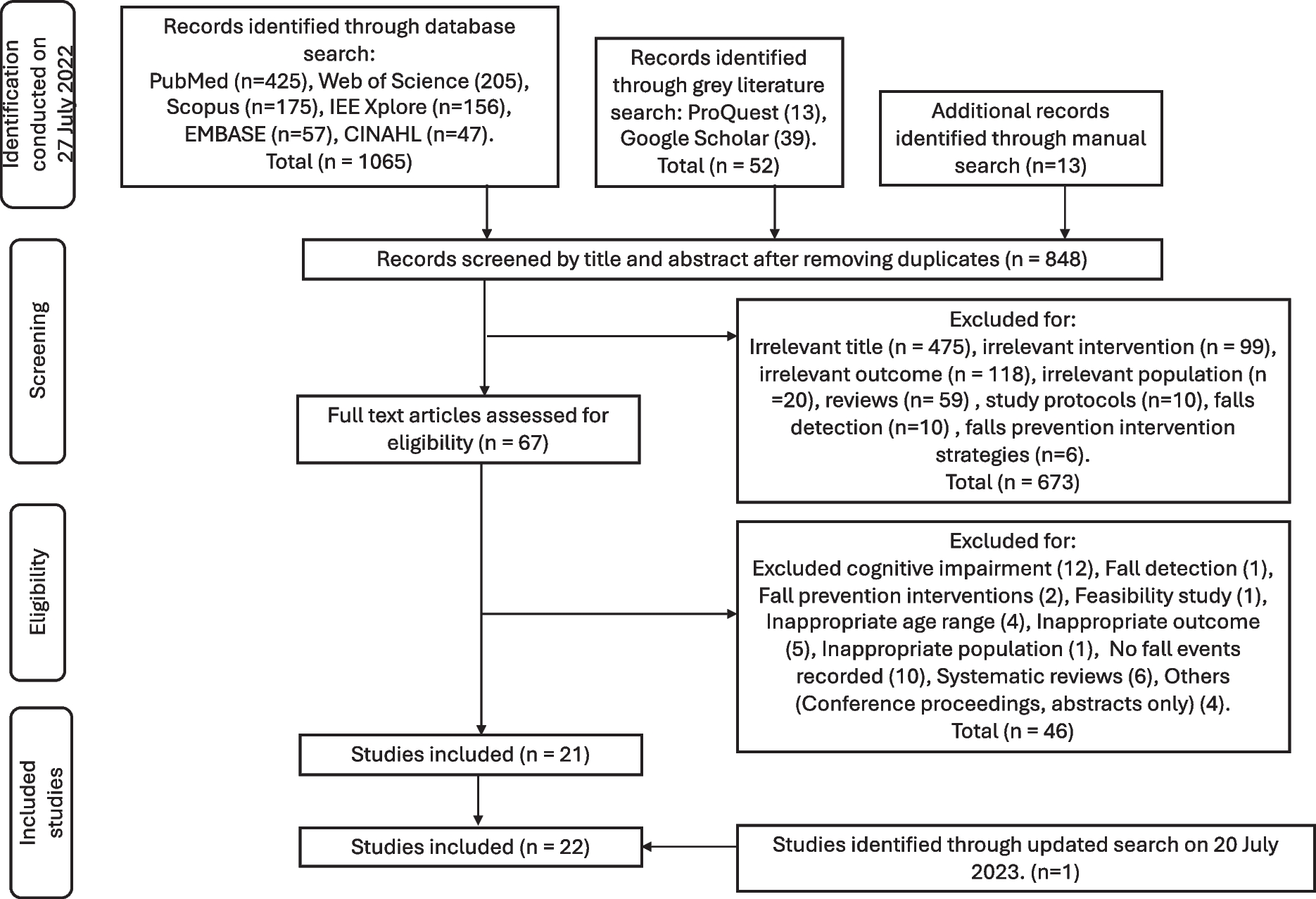
REStORing health of acutely unwell adulTs (RESORT) is an observational, longitudinal, and prospective cohort of geriatric rehabilitation inpatients admitted to the Royal Park Campus of the Royal Melbourne Hospital (Melbourne, Australia). More details on this cohort are presented in prior publications [12, 15, 16]. Briefly, after acute hospitalization, patients who required comprehensive care to restore functional capacity were transferred to geriatric rehabilitation wards. A Comprehensive Geriatric Assessment (CGA) was used to assess physical, psychological, functional, nutrition, and sociological domains within 48 h of rehabilitation admission. Written informed consent was obtained from inpatients or nominated proxies. Patients were excluded if they were unable to provide informed consents, without a legal proxy to consent, or undergoing palliative care at admission. Inpatients from the RESORT cohort without bilateral lower extremity paralysis were eligible for inclusion in the Ending PyJama (PJ) Paralysis campaign [11], and no further restrictions on ambulation status were present. As part of this campaign, a random sample of inpatients from two out of four geriatric rehabilitation wards wore an inertial sensor (ActivPal4, PAL Technologies Ltd, Glasgow, Scotland, UK) to measure instrumented SB and PA from October 22, 2019, to March 29, 2020. There were 145 patients who wore the ActivPal4. This study was approved by the Melbourne Health Human Research Ethics Committee (HREC/17/MH/103) with all ethical guidelines adhered to in accordance with the Declaration of Helsinki [17].
Data collection
Age, sex, ethnicity, education, and length of stay in geriatric rehabilitation were retrieved from medical records. A stadiometer was used to assess standing height if the inpatient could stand. Otherwise, knee height was assessed, from which height was calculated [18]. Weight was assessed using a standing scale, seated scale, or a weighted hoist depending on the patient’s ambulation status. Body mass index (BMI) was calculated using body mass (kg) divided by height (m) squared and expressed in kg/m2. The primary reason for hospital admission was categorized into cardiovascular, musculoskeletal, neurological, psychiatry, respiratory, and other reasons. Principal diagnoses, including falls, fractures, and functional decline, were extracted from medical records.
Comorbidity was assessed using the Cumulative Illness Rating Scale (CIRS, range 0–56) with higher scores indicating greater comorbidity burden, which is calculated by dividing the total score with the number of affected physiological systems [19]. The usage of medication was obtained from medical records. Frailty was assessed by the Clinical Frailty Scale (CFS, range 0–9) with higher scores indicating increased frailty and associated risks [20]. Cognitive impairment was defined as a dementia diagnosis reported in medical records, standard Mini-Mental State Examination (sMMSE) score < 24/30 [21], Montreal Cognitive Assessment (MoCA) score < 26/30 [22], and/or Rowland Universal Dementia Assessment Scale (RUDAS) score < 23/30 [23], if further cognitive testing was indicated. The Short Confusion Assessment Method was used to assess the risk of delirium [24]. The Hospital Anxiety and Depression Scale (range 0‒21) was used to assess significant anxiety and depression symptoms with a cut-off score of ≥ 8 [25]. The use of a walking aid and history of falls were self-reported by patients and/or carers. The Functional Ambulation Classification (FAC, range 0‒5) was used for assessing ambulation status with higher scores indicating less support is required (i.e. independent) [26]. Handgrip strength was measured using a handheld dynamometer (JAMAR hand dynamometer; Samsons Preston, Inc.) on both hands three times each, alternating each time [27]. The maximum value (kg) was used for analyses. Inpatients who were unable to perform handgrip strength tests due to medical reasons were ascribed 0.00 m/s or 0.0 kg. The Short Physical Performance Battery (SPPB, range 0–12) was used to assess physical performance with higher scores indicating better performance [28]. The Katz index of activities of daily living (KADL, range 0–6) [29] and the Lawton and Brody scale of instrumental ADL (IADL, range 0–8) [30] were used to measure functional performance with higher scores indicating greater living independency. Malnutrition risk was assessed by the Malnutrition Screening Tool (MST) by which patients with a score ≥ 2 were classified as at risk [31].
Blood biological age prediction
Biological age using blood parameters was predicted using the BloodAge clock, available via the online SenoClock platform (https://www.deeplongevity.com/senoclock) developed by Deep Longevity, Hong Kong (subsidiary of Regent Pacific 00575.HK) [2]. SenoClock-BloodAge is a modular ensemble of 21 deep neural networks (DNNs) trained using over 60,000 samples from common blood biochemistry and cell count tests. A total of 30 clinical frequently measured blood biochemistry and cell count parameters were input in the biological age prediction: albumin, hemoglobin, white blood cells, platelets, hematocrit, red blood cell, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, red cell distribution width, mean platelet volume, neutrophils, lymphocytes, monocytes, eosinophils, basophils, sodium, potassium, chloride, calcium, phosphorous, blood urea nitrogen, creatinine, total protein, total globulin, total bilirubin, alanine transaminase, aspartate transaminase, gamma-GT, and alkaline phosphatase. Blood tests for the abovementioned parameters undertaken close to rehabilitation admission after acute care were included. If one blood parameter was unavailable, the patient was excluded from the analysis.
Objective measurement of sedentary behaviour and physical activity
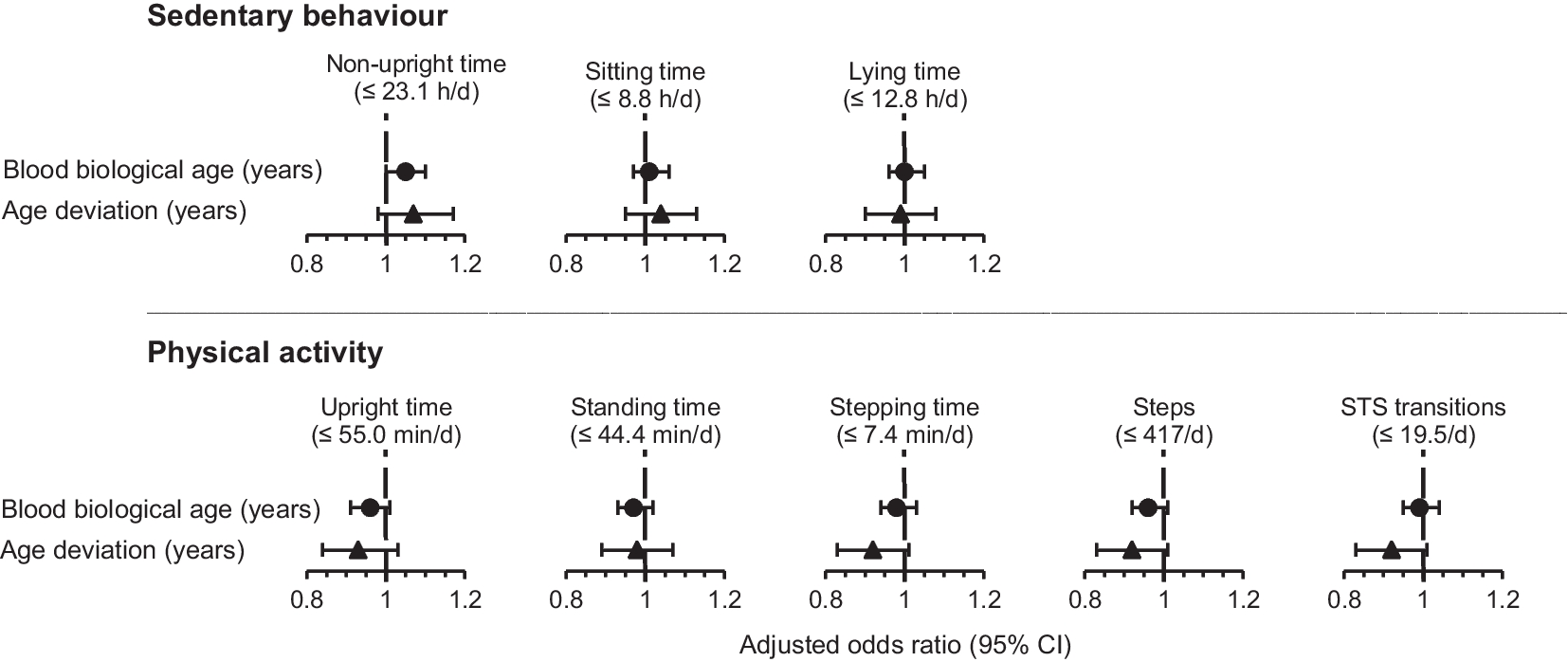
Details on the collection of physical activity data is presented elsewhere [11, 12, 15]. In brief, from day 5 (range 3–7) after rehabilitation admission, patients wore an ActivPAL4 inertial sensor on their right thigh for 7 days, or until hospital discharge, to objectively assess daily SB and PA. The ActivPAL4 consists of a triaxial capacitive accelerometer with a range of ± 4 g that collected data in 15-s epochs at a sampling frequency of 20 Hz and analyzed in 60-s epochs. A valid day of measurements was defined as 20 out of 24 h of wear. Patients were included in the analyses if they reported at least one valid day. The ActivPAL software (Generation 8, PAL Technologies Ltd.) was used to generate eight SB and PA measures, which were averaged over valid days [11, 15]. Daily objectively measured SB patterns were described by the median of the mean time spent non-upright (sum of sitting and lying), mean sitting time, and mean lying time in hours/day. Daily objectively measured PA patterns were described by the median of the mean time spent upright (sum of standing and stepping), mean standing time, and mean stepping time in minutes/day, and the median of the mean number of steps and mean sit-to-stand (STS) transitions per day.
Statistical analyses
Descriptive statistics for continuous variables with a normal distribution were presented as means ± standard deviations (SD) and a non-normal distribution as medians [interquartile ranges, IQR]. Categorical variables were presented as numbers (percentages). Numerical variables were compared using independent sample t-tests (normal distribution) and the Mann–Whitney U tests (skewed distribution), and categorical variables were compared using \(^\)-tests or Fisher’s exact tests (categorical variables).
The independent variables were blood biological age and age deviation, for which age deviation was defined as the difference between blood biological age and chronological age (i.e. blood biological age minus chronological age). A positive difference indicates an individual is biologically older than their chronological age. The dependent variables, the eight SB and PA measures, were dichotomized using the median as a cut-off into groups of patients with low/high SB and low/high PA. The association of blood biological age or age deviation with objectively measured SB and PA measures was investigated using binary logistic regression analyses. Analyses included a crude model and a model adjusted for CIRS. Results are presented as odds ratios (OR) with 95% confidence intervals (CI).
The statistical significance level was set at \(\alpha \mathrm\), and a trend was defined as an \(\alpha\) value of greater than 0.05 and less than 0.10. Analyses were performed using the IBM SPSS Statistics for Macintosh, Version 27.0 (IBM Corp.).








留言 (0)