
記住我
All measurements were performed on a dual-head Symbia Intevo 6 SPECT/CT system (Siemens Healthineers) with 3/8 inch NaI(Tl) crystals. The rectangular field of view (FOV) was 53.3 cm x 38.7 cm. Data was acquired using a low-energy high-resolution (LEHR) collimator (hole length: 24.05 mm, septal thickness: 0.16 mm, hole diameter: 1.11 mm) for 99mTc and a medium-energy low-penetration (MELP) collimator (hole length: 40.64 mm, septal thickness: 1.14 mm, hole diameter: 2.94 mm) for 166Ho and 99mTc to investigate the influence of the collimator. Dual-energy windows were used for both isotopes. For 99mTc, the photopeak window was centered at 140 keV (15% width) with an adjacent lower scatter window at 119 keV (17.6% width). The 166Ho photopeak window was set to 81 keV (15% width). An additional scatter window at 118 keV (12% width) was used to correct for down-scattered high-energy photons. Activity for the phantom experiments was measured using a dose calibrator (ISOMED 2010, NuviaTech Healthcare).
Sensitivity and count rate performanceThe sensitivity was measured using a point source placed in the center of the FOV without attenuation and scatter with activities of 146 MBq and 222 MBq for 99mTc and 166Ho, respectively. Planar images were acquired for 5 min on a 256 × 256 matrix. The source-detector distance was set to 10 cm.
The effects of dead time and the resulting deviations of count rate linearity were analyzed depending on the activity at scan time. A custom-made phantom with a body-shaped cross section (diameter 30 cm, width 8 cm), including parts of the ribs and spine with bone-equivalent tissue (Fig. 1a), was used to simulate patient attenuation and scattering conditions. An activity-filled vial was placed in a hole at the center of the phantom. Activities ranging from 190 MBq to 2835 MBq and 154 MBq to 6780 MBq were measured for 99mTc and 166Ho, respectively. Planar images were acquired as mentioned above. Anterior and posterior detector-phantom center distances were set to 22 cm and 17 cm, respectively, similar to patient settings. For data analysis, the counts in the photopeak window were plotted against the activity in the phantom. For each isotope and collimator, a data fit was performed according to the paralyzable detector model as follows:
Fig. 1
(a) Custom-made phantom with a body-shaped cross section, including parts of the ribs and spine with bone-equivalent tissue used for count rate performance measurements. (b) NEMA image quality phantom wrapped in cooling gel packs to mimic the attenuation and scattering conditions of an obese patient. The NEMA image quality phantom was used for quantitative evaluation of image quality and investigation of the influence of patient obesity. (c) CT image of the NEMA image quality phantom. Transverse slice at the level of the spheres. Background ROIs (blue) and lung insert ROI (red)
$$C\left( A \right) = \alpha \cdot A \cdot }$$
(1)
where C is the measured count rate, A is the activity at scan time, α describes the linear detector performance and τ is the detector dead time. It was specified that the curve passes through the axis origin. In addition, energy spectra were measured and analyzed.
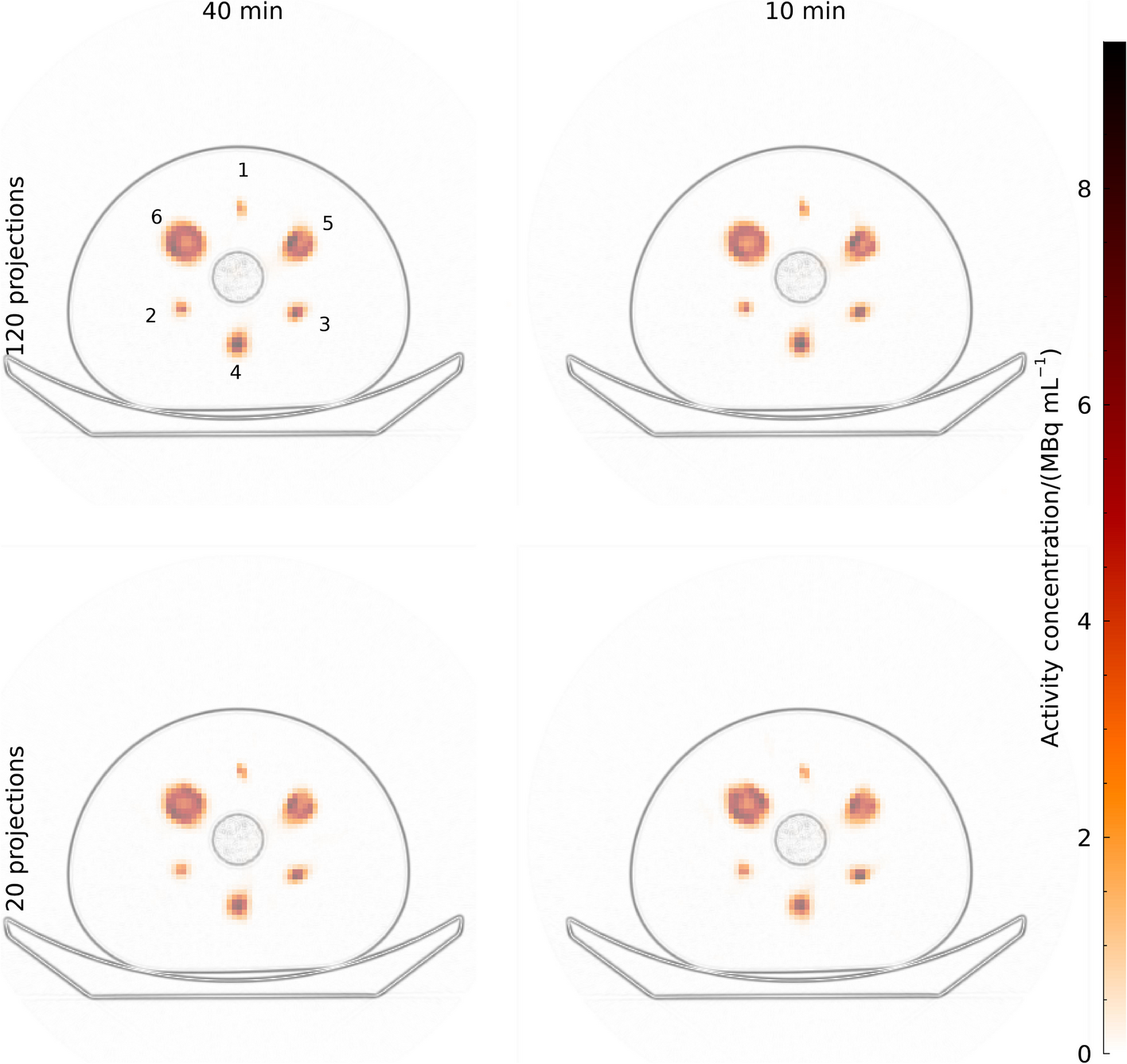
Quantitative evaluation of image qualityPhantom setupsThe torso-shaped NEMA image quality (IQ) phantom, containing a fillable background compartment, six fillable coplanar spheres (inner diameter = 10, 13, 17, 22, 28, and 37 mm), and a cylindrical lung insert, was used to evaluate the image quality and spatial resolution. It was filled with three different sphere-to-background activity concentration ratios to resemble clinical setups. To mimic high extrahepatic abdominal deposition, which is characterized by small activity spots with no background activity, the phantom was measured with activity in the six spheres only. Spheres and the background compartment were filled to mimic the activity distribution in the liver with different activity accumulation in the tumor and parenchymal tissue. A sphere-to-background activity concentration ratio of 4:1 was used to mimic liver metastases with moderate uptake, and a sphere-to-background ratio of 8:1 to mimic lesions of hepatocellular carcinoma (HCC) with higher activity uptake relative to the parenchyma. The activity concentrations in the spheres and background were chosen to be similar to those in clinical practice, assuming a patient with a liver volume of 2000 ml containing 150 MBq of 99mTc or 250 MBq of 166Ho, which are standard activity values for pre-treatment SIRT diagnostics. A tumor fraction of 10% (200 ml) and a homogeneous activity distribution in tumors and liver parenchyma were assumed. The actual activity concentrations at the time of imaging are shown in Table 2. The phantom was also measured after being wrapped in cooling gel packs (Fig. 1b) to mimic the attenuation and scattering conditions of an obese patient. The cooling packs form an additional thickness of approximately 3 cm around the phantom. The attenuation coefficient of the cooling packs was similar to that of water.
Table 2 Information on the measurements with the NEMA image quality phantom filled with 99mTc and 166Ho in different phantom setups (spheres without background; sphere-to-background activity concentration ratio 8:1 and 4:1)Planar imaging of the NEMA image quality phantomFor the evaluation of the planar scintigraphic imaging characteristics of 99mTc and 166Ho, planar anterior and posterior images were acquired for each phantom setup with an acquisition time of 5 min and an image matrix of 256 × 256. Additional measurements of 99mTc with the MELP collimator and a reduced acquisition time of 22 s were performed to investigate the influence of the used collimator and the low gamma emission probability of 166Ho compared to 99mTc. The reduced acquisition time was chosen based on the ratio of the gamma emission probabilities of 166Ho to 99mTc. Planar scatter correction was applied for 166Ho. The images were evaluated with regard to the pre-treatment determination of the liver-lung shunt in SIRT, which is usually based on planar scans. A region of interest (ROI) was placed in the phantom simulating the liver and another ROI was placed above the phantom in an area of no activity. The ratio of the counts in the ROI outside the phantom to the sum of the counts in both ROIs was calculated as a measure of apparent lung shunt.
SPECT/CT acquisition and reconstruction parametersAll SPECT data was acquired with 120 projections (60 per head, 20 s per projection) over a non-circular 360° orbit using step-and-shoot mode, followed by a low-dose CT scan (130 kV, 20 mAs, 2.5 mm slice thickness) for attenuation correction. The images were reconstructed to a voxel size of 2.4 × 2.4 × 2.4 mm3 using the 3D OSEM algorithm (Flash 3D; Siemens Healthineers) with 8 iterations and 8 subsets for 99mTc and 16 iterations and 8 subsets for 166Ho according to our clinical routine. Gaussian post-reconstruction filtering of 9 mm was applied. Scatter correction for 99mTc was performed using the dual-energy window method with an adjacent lower scatter window and a scatter fraction k-factor of 0.5. For 166Ho the photopeak was corrected for scatter with the upper scatter window at 118 keV and a k-factor of 1.4, as previously investigated [6]. Additional measurements of 99mTc with the MELP collimator and a reduced scan time of 1.5 s per projection were performed to investigate the influence of the used collimator and the low gamma emission probability of 166Ho compared to 99mTc. The acquisition times were adjusted over time according to the respective half-life to obtain comparable count statistics. To obtain information on statistical variation and reproducibility of the results, measurements of the NEMA IQ phantom at 8:1 contrast and standard phantom setup were performed exemplarily twice. The average and standard deviation of both measurements were used for further analysis.
Influence of count statisticsThe influence of count statistics on SPECT image quality was evaluated by examining the reconstructed images of the NEMA IQ phantom with a sphere-to-background ratio of 8:1 for different acquisition times. SPECT images with projection times of 5 s, 10 s, 15 s, and 20 s for 99mTc and 10 s, 20 s, and 30 s for 166Ho were analyzed.
Image analysisThe SPECT images were evaluated in terms of contrast recovery, image noise, detectability, relative count error in the lung insert, and spatial resolution. The six hot spheres were segmented using 3D isocontours with a 50% background-adapted threshold for each sphere according to [7]. Three cylindrical volumes of interest (VOI) (45 mm diameter, 150 mm length) were defined in the phantom background (Fig. 1c). The lung insert was delineated with a cylindrical centered VOI (30 mm diameter, 130 mm length) similar to the NEMA NU 2-2018 protocol [8].
The contrast recovery coefficient (CRC) was calculated for each of the six hot spheres as follows:
$$CRC = \frac_}}}}_}}}}} - 1}}} \cdot 100\%$$
(2)
where \(}_}\) is the mean number of counts in the sphere VOI, \(}_}\) is the mean number of counts in the background VOIs, and \(R\) is the true sphere-to-background activity concentration ratio. The relative count error in the lung insert (\(\varDelta _})\) was determined as:
$$\Delta }}} = \frac_}}}}}_}}}}} \cdot 100\%$$
(3)
where \(}_}\) is the mean number of counts in the lung insert VOI. To evaluate the image noise, the noise coefficient of variation (\(_\text}\)) was calculated using:
$$C}}} = \frac}}}}}_}}}}} \cdot 100\%$$
(4)
where \(_}\) is the standard deviation of all voxels within the three background VOIs. The contrast-to-noise ratio (CNR) was used to asses object detectability. It was calculated for each sphere as follows:
$$CNR=\frac}_}-}_}}_}}$$
(5)
The tomographic spatial resolution was determined based on the analysis of radial profiles through the homogeneously filled phantom spheres in the reconstructed images according to [9]. The full width at half maximum (FWHM) of the point spread function was assessed using the software Rover (version 3.0.60h, ABX, Germany).
留言 (0)