
記住我



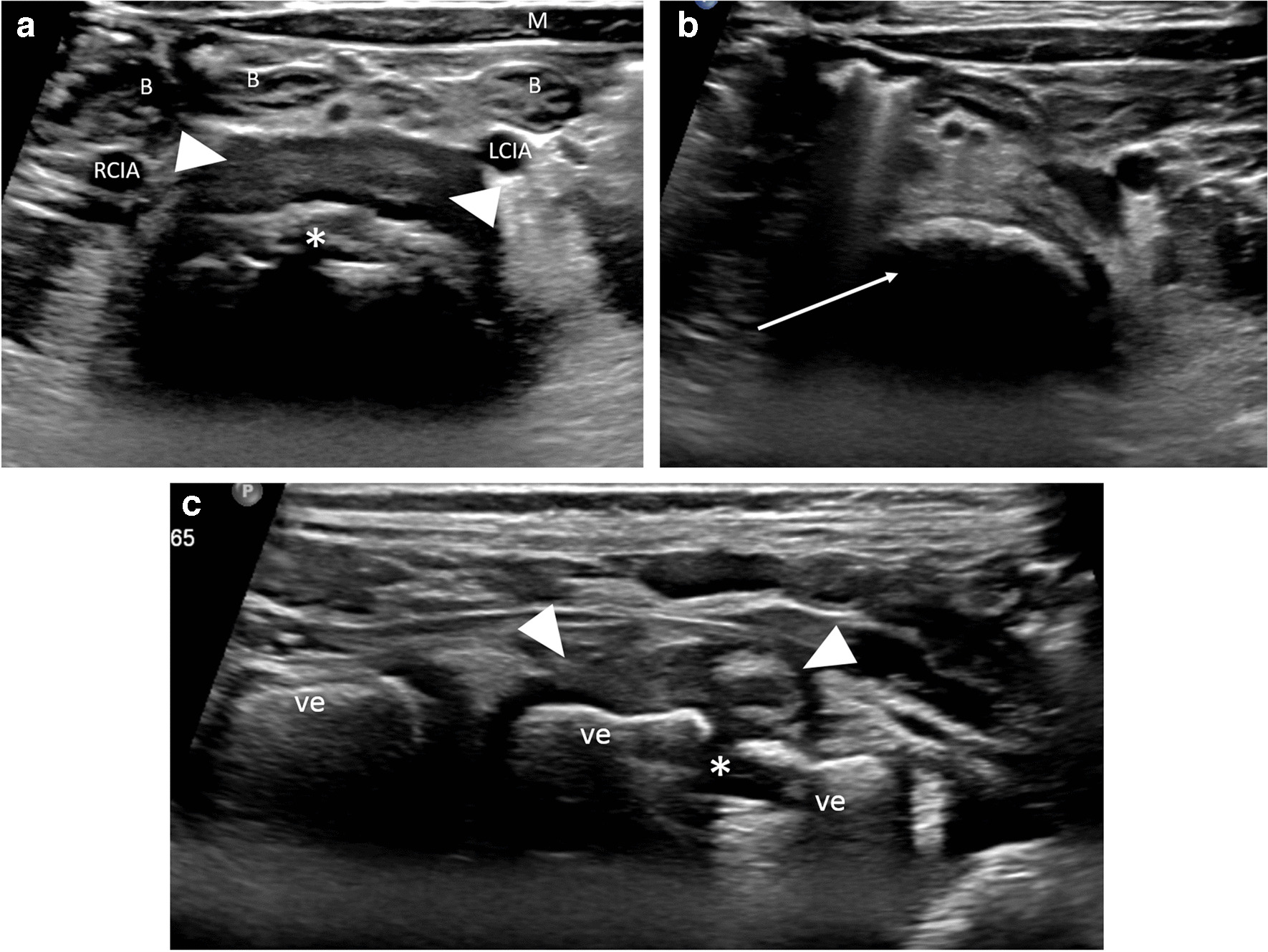
Bowel ultrasound is a useful diagnostic tool in the diagnosis and management of necrotizing enterocolitis (NEC) but can be time-consuming and requires technical expertise, particularly for assessing pneumatosis. Previous literature on sonographic evaluation of NEC has focused on a full bowel ultrasound protocol, but the utility of an abbreviated protocol primarily aimed at identifying high-risk sonographic findings without focused bowel assessment has not been well studied.
ObjectiveThis study aims to describe the diagnostic accuracy of an abbreviated ultrasound protocol for identifying high-risk NEC findings.
Materials and methodsThis is a retrospective, institutional review board-approved study. We identified all abbreviated NEC ultrasounds performed between January 2014 and August 2022 at our institution. Exams were reviewed for the presence of high-risk findings including pneumoperitoneum, fluid collections, and complex free fluid. Clinical outcome was categorized as poor or good depending on if emergent surgical intervention or death related to NEC occurred. The frequency of follow-up NEC ultrasounds was reviewed to determine if new findings affected outcome. Sensitivity, specificity, and positive and negative predictive values were generated to assess the performance of the abbreviated ultrasounds to identify high-risk findings.
ResultsA total of 84 abbreviated abdominal ultrasounds were performed on 73 children. Median age at the time of ultrasound was 41 days (interquartile range (IQR) 53 days) and median gestational age was 35 weeks and 3 days (IQR 80 days), and 44/73 (60%) were male. Thirteen ultrasounds had at least one high-risk finding with nine (69%) resulting in a poor outcome, including seven surgical interventions and four deaths. Two patients had surgical intervention and died as a result of necrotizing enterocolitis. Ultrasounds without high-risk findings were not associated with poor clinical outcomes. Sensitivity, specificity, positive predictive value, and negative predictive value of the abbreviated NEC ultrasound were 100% (95% CI 60–100%), 95% (95% CI 86–98%), 69% (95% CI 39–90%), and 100% (95% CI 94–100%), respectively. Twelve abbreviated ultrasounds were followed by a second NEC ultrasound within 5 days. Five follow-up ultrasounds demonstrated new high- or low-risk findings, but the new findings did not correlate with a change in outcome as predicted by the initial ultrasound.
ConclusionAn abbreviated NEC ultrasound can be of clinical utility in predicting poor outcomes, particularly during non-business hours when resources are limited.
Graphical abstract
留言 (0)