
記住我




Several abstracts covered novel diagnostic applications of PET imaging in breast cancer patients. [18F]FDG PET can be limited for detection of small metastases, lymph node metastases, and in patients with particular tumour types or receptor expression, for example, in patients with lobular or with low-grade oestrogen receptor-positive breast cancer. Other PET tracers than [18F]FDG have been proposed to overcome these limitations and to broaden the applicability of diagnostic PET imaging in patients with different clinical presentations of breast cancer.
For example, Knip et al. analysed patients with stage II/III or locoregional recurrent oestrogen receptor-positive breast cancer in a prospective multicentre clinical trial to compare the influence of histological subtype and tumour grade on [18F]FDG and oestrogen receptor-targeting [18F]FES PET. A total of 41 patients with 43 tumours were included, and suspect lesions were verified by pathology or conventional imaging. The authors showed that [18F]FES-PET is more accurate in lobular and grade-1 ductal tumours, whereas for grade 2 and grade 3 ductal tumours, [18F]FDG-PET and [18F]FES-PET performed equally well. The results indicate that both histological subtype and tumour grade can influence the selection of the optimal PET tracer and that a selection based on tumour biology may be necessary to increase the clinical value of PET imaging in heterogeneous diseases, such as breast cancer.
A different approach is the usage of pan-cancer tracers like radiolabelled fibroblast activation protein inhibitors (FAPIs) which may be more specific than [18F]FDG and can be applied in different tumour biologies. Guo et al. investigated the diagnostic accuracy of [68 Ga]Ga-FAPI-46 PET-CT in patients with primary and metastatic breast cancer in comparison with breast ultrasound and [18F]FDG PET-CT. They included 30 patients without further subclassification for hormone receptor status who underwent PET-CT for diagnosis of suspected breast lesions at initial staging or for detection of recurrence. SUVmax, tumour-to-background ratio, lesion detection rate, and TNM classification were evaluated. [68 Ga]Ga-FAPI PET-CT showed higher tracer uptake and tumour-to-background ratios than [18F]FDG PET-CT in different anatomical categories. Moreover, it detected more lesions than [18F]FDG PET-CT and breast ultrasound. This can lead to upstaging in TNM classification and potentially lead to a change in management in a relevant fraction of patients.
However, breast cancer was not the only tumour type which was investigated by FAP-targeted imaging. Chen et al. compared the diagnostic performances of [68 Ga]Ga-FAPI PET-CT and [18F]FDG PET-CT in diagnosing lymphomas also aiming to characterise the influences of FAP and glycolytic markers on tracer uptake by involved lesions. A total of 186 participants underwent dual-tracer imaging, and [18F]FDG was characterised by a higher staging accuracy (98.4%) than [68 Ga]Ga-FAPI (86.0%). Moreover, 52 FAPI + /FDG − lesions and 2939 FAPI − /FDG + lesions were observed. GLUT1 and hexokinase-2 were overexpressed in both lymphoma cells and the tumour microenvironment, while FAP was only expressed in stromal cells. Similarly, Watanabe et al. carried out a head-to-head comparison of [68 Ga]Ga-FAPI PET-CT, [18F]FDG PET-CT, and contrast-enhanced CT in 241 patients with various solid tumours. Scans were reviewed by one blinded central reader. Clinical use and accuracy indicators were calculated by means of histopathological validation from 629 lesions. Per-patient, per-region, and per-lesion detection rates were significantly higher in [68 Ga]Ga-FAPI PET-CT compared to [18F]FDG PET-CT for total, primary, abdominopelvic, liver, and other metastases (p < 0.05). Sub-analysis also showed that [68 Ga]Ga-FAPI PET-CT outperforms [18F]FDG PET-CT in terms of accuracy indicators. [68 Ga]Ga-FAPI PET-CT was also the subject of the study from Lanzafame et al. who focused their attention on various bone and soft-tissue type sarcomas. They analysed the scans of 200 patients and showed higher maximum SUV values particularly for soft-tissue type sarcomas and myxoid liposarcomas using [68 Ga]Ga-FAPI compared to [18F]FDG (Fig. 1). Overall [68 Ga]Ga-FAPI PET-CT showed higher clinical performance scores compared to [18F]FDG PET-CT. Correlation between [68 Ga]Ga-FAPI uptake and histopathologic FAP expression showed a moderate positive trend. With a SUVmax > 10 cut-off for all regions, FAP-directed radioligand therapy eligibility was found for about half of the patients.
Fig. 1
In patients with sarcoma, [68 Ga]Ga-FAPI PET has a higher tumour uptake and detection rate and equal accuracy when compared with [18F]FDG PET. FAP expression can be also used to candidate patients for radioligand therapy (courtesy of Helena Lanzafame et al.). A modified version of the figure appears in the final publication resulting from the presented study [2]
Besides FAPI PET, PSMA-targeted PET imaging and radioligand-based theranostics in patients with prostate cancer are and have been a major topic in all major nuclear medicine conferences over the recent years and already deserve to be regarded as a great classic. Certainly, EANM’23 should not be missed in this trend, and exciting and groundbreaking results on PSMA theranostics were presented. Hofman et al. showed the 54-month follow-up of the proPSMA trial, in which the authors found baseline [68 Ga]Ga-PSMA-11 PET-CT to be prognostic for treatment failure in men with intermediate-to-high risk prostate cancer. A total of 251 patients (ISUP grade groups 3–5, PSA ≥ 20 ng/ml or clinical stage ≥ T3, M0 disease and a median follow-up of 41.0 months) were included. Patients were treated with curative-intent surgery or radiotherapy with or without androgen deprivation, and treatment failure was defined by biochemical failure, initiation of salvage therapy, or development of distant metastatic disease. In the analysis, regional nodal status assessed by [68 Ga]Ga-PSMA-11 PET-CT was prognostic for medium-term oncologic outcomes (for freedom from treatment failure: HR 2.1, p = 0.01), outperforming conventional imaging in which nodal status was not prognostic.
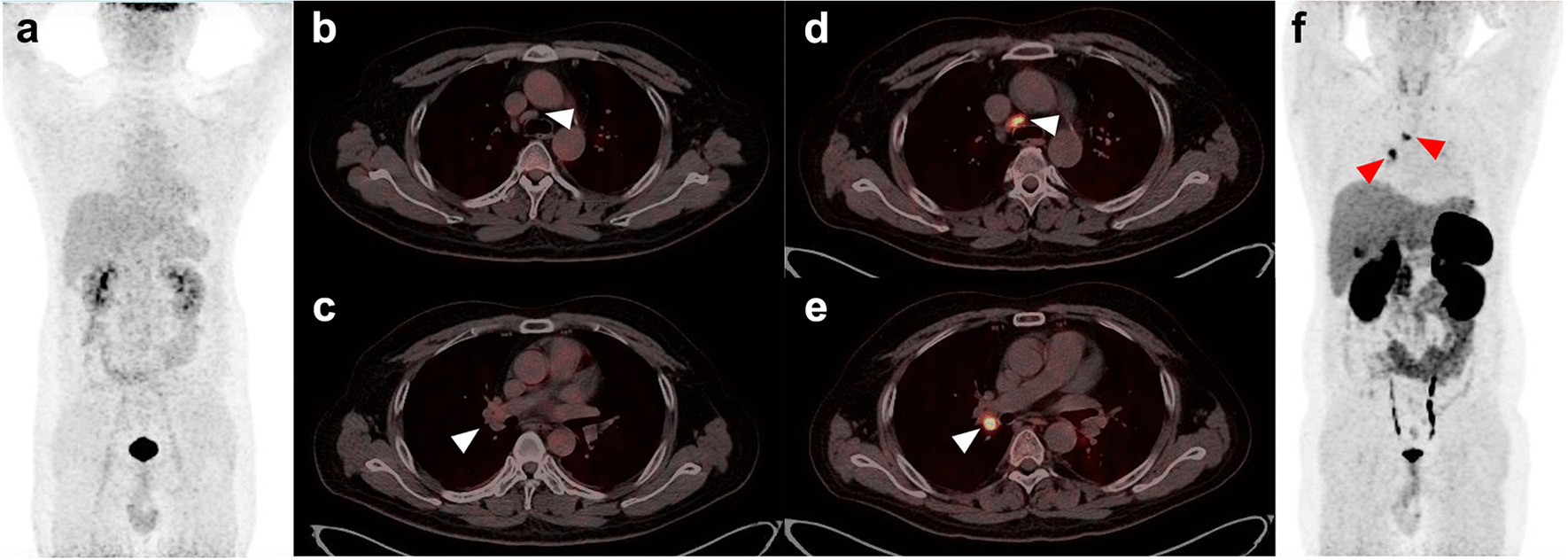
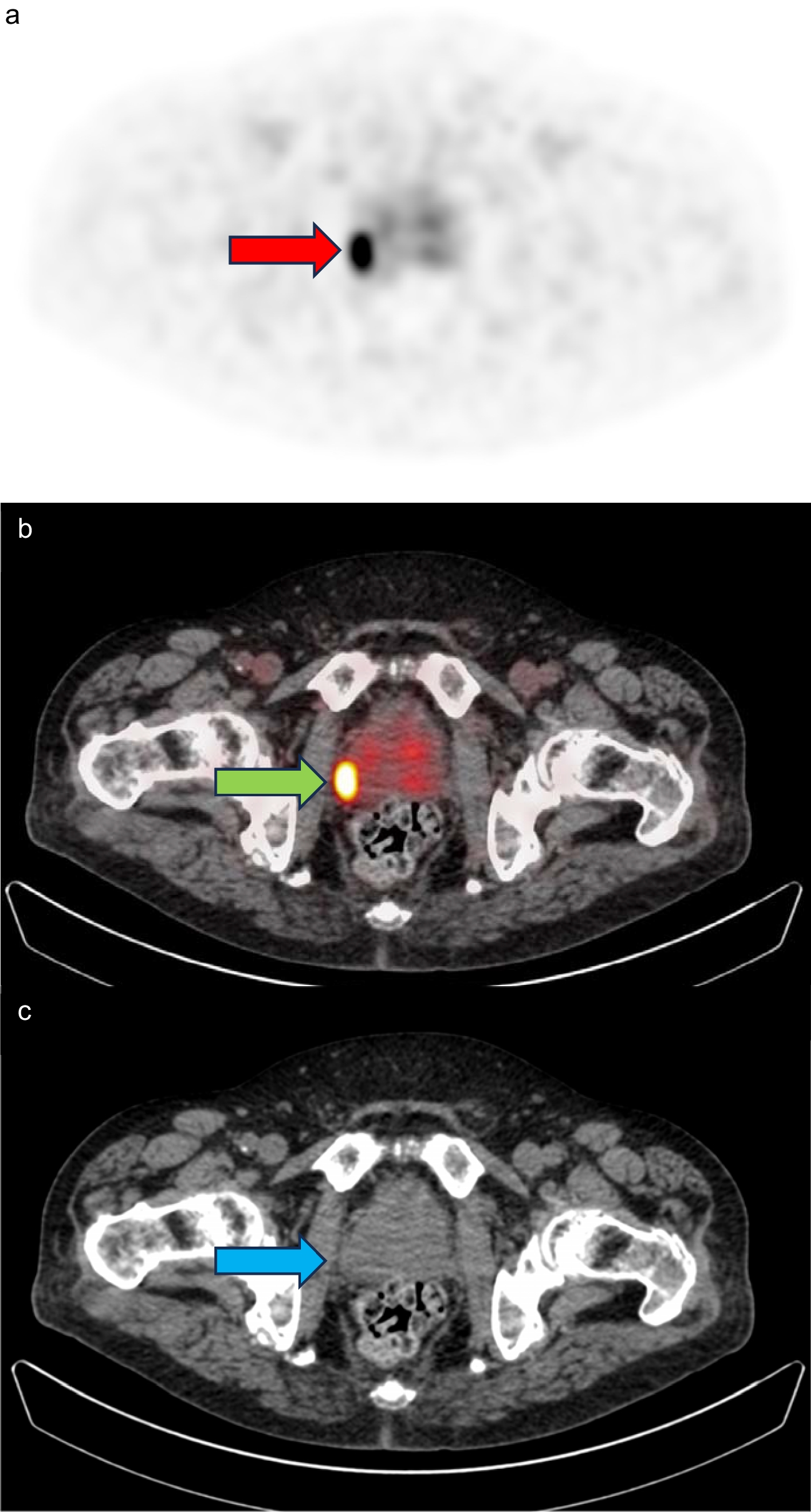
These data are another example of the clinical high value of PSMA-targeted PET-imaging in different stages of prostate cancer. However, the symphony of theranostic PET tracers for this disease does not end with PSMA. A different opportunity, for example, for patients without PSMA expression, is the use of gastrin-releasing peptide receptor (GRPR)-targeting molecular imaging. Duan et al. presented the final results from a prospective phase II/III imaging trial in which they investigated PET-MRI using the GRPR-antagonist [68 Ga]Ga-RM2 in patients with biochemical recurrence of prostate cancer [3]. One hundred patients with rising PSA levels after prostatectomy or radiotherapy and non-contributory conventional imaging (negative CT, MRI, and/or bone scan) were included and the diagnostic performance of [68 Ga]Ga-RM2 PET-MRI was compared to that of MRI alone. They found a better diagnostic performance of [68 Ga]Ga-RM2 PET-MRI with significantly higher detection rates, sensitivity, and accuracy, indicating the highly promising characteristics of GRPR-targeted PET-MRI. Figure 2 shows detection rates of [68 Ga]Ga-RM2 PET/MRI in comparison to MRI alone for different serum PSA level groups and image examples of a patient with a subcentimeter, non-specific lymph node, which was ruled negative on MRI, but positive on [68 Ga]Ga-RM2 PET-MRI and subsequently revealed to be a lymph node metastasis.
Fig. 2
Top: The detection rates of [68 Ga]Ga-RM2 PET-MRI were greater than MRI across all PSA ranges; the figure was reprinted with permission from the final publication resulting from the presented study [3]. Bottom: Image example of a 65-year-old man with biochemically recurrent prostate cancer. PSA at the time of PET-MRI was 7.9 ng/mL. 68 Ga-RM2 PET-MRI (axial PET (A); axial fused PET-MRI (B); maximum intensity projection [MIP] (D), respectively) shows a positive lymph node interaortocaval (red arrows). MRI (axial MRI (C)) shows a subcentimeter, non-specific lymph node, which was ruled negative. Subsequent lymph dissection revealed lymph node metastasis compatible with prostate cancer (courtesy of Duan et al.) [2, 3]
留言 (0)