INTRODUCTION
Amputation was a mainnstay treatment of soft tissue sarcomas in the extremities; however, owing to the improvements in adjuvant therapy and surgical techniques, limb-sparing surgery is now used as an alternative to amputation.1,2 To preserve the affected limb, the reconstruction of the defect after tumor resection is necessary. Surgical resection of sarcomas often results in large surgical wounds and skin defects.3,4 In such cases, postoperative wound healing takes longer, thereby prolonging hospital length of stay.
WOC nurses are certified by the Japanese Nurse Association. They are professional nurses who have completed their training for specific medical procedures in wound management. To become a WOC nurse, the applicant must be a licensed nurse practicing in Japan, have at least 5 years of experience, and have undergone training at an educational institution established by the Japanese Nurses Association. Traditionally, WOC nurses are responsible for management of pressure injuries, including debridement of necrotic tissue and delivery of negative pressure wound therapy (NPWT). In addition, some WOC nurses have completed specified act training, defined as training to perform specific interventions that can be performed under comprehensive instruction from a physician. Specifically, 38 interventions relative to WOC nursing are currently recognized as specified acts. Following training and certification in performance of these specified acts, nurses can respond promptly to their judgment without having to wait for a physician's order.
While WOC nurses practicing in Japan traditionally manage pressure injuries and ostomies in hospitalized and homebound patients, they are not mainly responsible for postoperative wound management.5–7 Nevertheless, WOC nurses are responsible for managing skin defects after sarcoma excision at our institution. Therefore, the purpose of this study was to determine the outcomes of the WOC nurse management of postoperative skin defects following wide surgical resection of sarcomas.
METHODS
We conducted a retrospective case-control study. Specifically, the medical records of patients who underwent wide resection for soft tissue sarcoma, followed by 2-stage split-thickness skin grafting, in our university hospital in Kagoshima, Japan. Patients cared for between December 2015 and April 2021 were identified retrospectively and included in our study; in contrast, cases for which wound healing could not be confirmed were excluded. We categorized cases into 2 groups; one cohort comprised patients managed by WOC nurses during their postoperative recovery, and the second group comprised patients not managed by a WOC nurse. Cases from January 2015 to December 2018 were assigned to the nonintervention group because they were cared for before the introduction of WOC nurse and the orthopedic management collaborative program, whereas patients managed from January 2019 to March 2021 were assigned to the intervention group since they were cared for after the introduction of the collaborative program. Research procedures were reviewed and approved by the Ethics Committee on Epidemiological Studies, Kagoshima University Graduate School of Medical and Dental Sciences, on June 29, 2021 (approval no. 2170070); an opt-out policy was employed, enabling patients to decline review of their medical records.
Outcome Measures
The following data were extracted from medical records by an orthopedic surgeon: age at surgery, sex, pathological diagnosis, tumor location, tumor depth, maximum tumor diameter, surgical time, and maximum skin defect diameter, use/nonuse of muscle flap, length of hospital stay, and duration of wound healing from surgery. The day of wound healing was defined as fully epithelialization of the skin graft when wound treatment was deemed no longer necessary.
Study Procedures
In our department, we usually cover deep organs such as bones and joints with a pedicled musculocutaneous flap at the resection and perform a 2-stage split-thickness skin graft after confirming a negative margin. Tissue defects were found to be subcutaneous in all cases.
Intervention Group
Patients assigned to the intervention group received care from a WOC nurse who was responsible for wound treatment immediately after surgical resection and through subsequent 2-stage skin grafting. Wound care was delivered daily and included wound cleansing, application of topical treatments such as alprostadil alfadex, isodine sugar paste, or silver sulfadiazine ointment, depending on the wound condition. In addition, the WOC nurse and the orthopedic surgeon routinely discussed progress toward healing and initiated NPWT when indicated using 1 of 2 available devices (V.A.C.; 3M, Minneapolis, Minnesota, or RENASYS, Smith & Nephew, Watford, United Kingdom). When NPWT was initiated, the orthopedic surgeon and the WOC nurse initiated treatment; subsequently, the WOC nurse independently performed NPWT dressing changes once or twice weekly as indicated. The maximum duration of treatment with NPWT was 28 days.
When the orthopedic surgeon determined sufficient granulation tissue was present in the wound bed, the wound was closed with a split-thickness skin graft. We fixed the grafts with tie-over fixation and continued postoperative wound care including regular cleansing and application of topical therapies as indicated. The patient learned wound self-care techniques from the WOC nurse in preparation for hospital discharge, often before the wound closed completely. While patients were discharged with open wounds managed by topical interventions, they remained in the hospital during NPWT. Outpatient follow-up after discharge was provided by the orthopedic surgeon.
In the nonintervention group, the orthopedic surgeon performed daily wound care and directed topical wound management strategies. The WOC nurse was not directly involved in any aspect of the patient's postoperative wound management.
Data Analysis
Statistical analyses were completed using JMP software version 16.1.0 (SAS Institute Inc, Cary, North Carolina). Group differences were analyzed using the χ2 test for independence and Wilcoxon tests as indicated. P values less than .05 were deemed statistically significant.
RESULTS
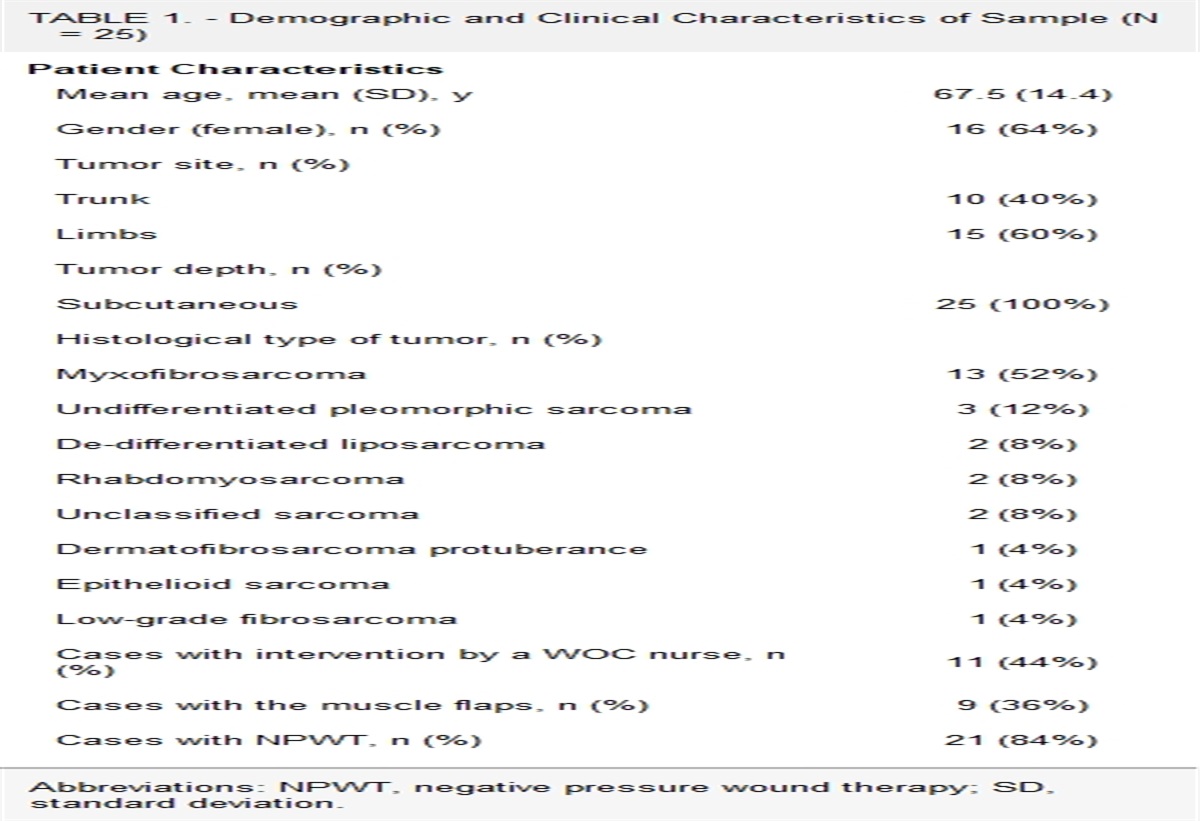
Medical records of 25 patients were reviewed; 11 (44%) were in the intervention group, and 14 (56%) were in the nonintervention group. Demographic and clinical data of patients are summarized in Table 1. Their mean age was 67.5 years (SD = 14.4), and 16 were female. Tumors occurred in the body trunk in 10 (40%) patients and in the limbs in 15 (60%) patients; all tumors were subcutaneous. The histopathological types of tumors were as follows: myxofibrosarcoma (n = 13 patients, 20%); undifferentiated pleomorphic sarcoma (n = 3, 12%); de-differentiated liposarcoma (n = 2, 8%); rhabdomyosarcoma (n = 2, 8%); unclassified sarcoma (n = 2, 8%); dermatofibrosarcoma protuberance (n = 1, 4%); epithelioid sarcoma (n = 1, 4%); and low-grade fibrosarcoma (n = 1, 4%). Nine of 25 patients (36%) underwent reconstruction with muscle flaps after tumor resection. Postoperative wound treatment with NPWT was performed for 21 patients (84%), which included 9 of 11 patients (82%) in the intervention group and 12 of 14 patients (86%) in the nonintervention group.
TABLE 1. -
Demographic and Clinical Characteristics of Sample (N = 25)
Patient Characteristics
Mean age, mean (SD), y
67.5 (14.4)
Gender (female), n (%)
16 (64%)
Tumor site, n (%)
Trunk
10 (40%)
Limbs
15 (60%)
Tumor depth, n (%)
Subcutaneous
25 (100%)
Histological type of tumor, n (%)
Myxofibrosarcoma
13 (52%)
Undifferentiated pleomorphic sarcoma
3 (12%)
De-differentiated liposarcoma
2 (8%)
Rhabdomyosarcoma
2 (8%)
Unclassified sarcoma
2 (8%)
Dermatofibrosarcoma protuberance
1 (4%)
Epithelioid sarcoma
1 (4%)
Low-grade fibrosarcoma
1 (4%)
Cases with intervention by a WOC nurse, n (%)
11 (44%)
Cases with the muscle flaps, n (%)
9 (36%)
Cases with NPWT, n (%)
21 (84%)
Abbreviations: NPWT, negative pressure wound therapy; SD, standard deviation.
We compared demographic and pertinent clinical characteristics in the group; no statistically significant differences were found between the groups in the patient's age, maximum tumor diameter, surgical time, maximum skin defect diameter, and duration of wound healing from resection (Table 2). Analysis indicate that the length of hospital stay in the intervention group was significantly shorter than that in the nonintervention group (intervention group length of stay: 38.3 days, SD = 8.0 vs 47.1 days, SD = 10.2 in the nonintervention group; P = .023).
TABLE 2. -
Comparison of Patient Characteristics and Outcomes Between the WOC Nurse Intervention Group and the Nonintervention Group
Intervention Group (n = 11)
Nonintervention Group (n = 14)
P Value
Age at surgery, mean (SD), y
64.4 (16.5)
69.9 (3.8)
.49
Maximum tumor diameter, mean (SD), mm
47.7 (24.0)
47.0 (21.6)
.94
Surgical time, mean (SD), min
173.8 (110.1)
146.6 (69.3)
.48
Maximum skin defect diameter, mean (SD), mm
131.8 (41.4)
140.7 (14.3)
.74
Cases with the use of a muscle flap, n (%)
5/11 (45%)
4/14 (29%)
.43
Cases with NPWT, n (%)
9/11 (82%)
12/14 (86%)
1.00
Length of hospital stay, mean (SD), d
38.3 (8.0)
47.1 (10.2)
.02
a
Duration of wound healing from resection, mean (SD), d
53.0 (15.5)
69.2 (47.3)
.55
Abbreviations: NPWT, negative pressure wound therapy; SD, standard deviation.
aP < .05; the differences in variables between the WOC nurse intervention group and the nonintervention group were evaluated using the χ2 and Wilcoxon tests.
DISCUSSION
We evaluated patients undergoing wide tissue resection for subcutaneous sarcomas who did or did not receive services of a WOC nurse and found that hospital length of stay was significantly shortened when a WOC nurse participated in postoperative management. We believe patient education from the WOC nurse focusing on self-management of wounds that were not completely healed may have contributed to these hospital stays. Additional benefits of WOC nurse participation included reducing the burden of ongoing wound management by the attending orthopedic surgeon and collaboration between the WOC nurse and the orthopedic surgeon. We further assert that WOC nurse care facilitated a smooth transition to outpatient care, creating a trusting relationship between the patient and the health care team.
In recent years, the usefulness of nurse-led wound management has been reported in Europe and the United States.8–12 Certified wound care nurses (CWCNs) are specialized wound care nurses who, under the guidance of a physician, manage pressure injuries and a variety of chronic wounds.13,14 These specialty practice nurses provide wound assessment, cleansing, debridement, NPWT, treatment planning, topical therapies, recommendations concerning systemic therapies such as wound-related medication recommendations, and ongoing assessment and treatment.13 Through a multidisciplinary approach that includes CWCNs for wound care, various benefits have been reported, such as reduced incidence of pressure injuries and complications during hospitalization, shorter hospital stays, and reduced hospitalization costs.13,14 We have also observed a shift in the focus of wound management from physicians to nurses in other areas of the world, though physicians still play a central role in postoperative wound management in Japan.9
In addition to these considerations, we have observed that Japanese physicians carry a high workload compared with other professionals, creating concerns related to average working hours. Recently, task sharing, which involves dividing tasks among more than 1 health care professional such as a WOC nurse, has become increasingly important to reduce the working hours of the surgeon while maintaining the current output volume.
Table 3 shows the 10 task-shifting/sharing duties proposed by the Japanese Orthopedic Association in 2019.15 The proposal includes shifting postoperative wound treatment tasks from the orthopedic surgeon to the WOC nurse; nevertheless, we acknowledge this practice has not been widely adopted in our country. The rationale for this task-sharing is partially based on knowledge that WOC nurses are skilled health care professionals who possess the knowledge and skills to share postoperative wound management tasks with the orthopedic surgeon. In Japan, WOC nurses are required to perform wound management based on procedure manuals prepared by orthopedic surgeons; we encourage them to demonstrate their full practice scope via collaborating with an orthopedic surgeon when caring for patients undergoing surgical management of subcutaneous sarcomas.
TABLE 3. -
The 10 Task-Shifting/Sharing Duties as Proposed by the Japanese Orthopedic Association in 2019
Task-Shifting/Sharing Items
To Whom?
1. Preparation of medical certificate and hospitalization summaries
Physician's administrative assistants
2. Instructions to patients on admission
Physician's administrative assistants
3. Explanation and acquisition of consent forms for noninvasive examinations
Nurses, therapists, and physician's administrative assistants
4. Explanation and acquisition of consent forms for hospitalization
Physician's administrative assistants
5. Data entry to medical/surgery records
Physician's administrative assistants
6. Assistance during casting
Prosthetist and orthotist
7. Assistance during surgery (providing surgeons with instruments)
Clinical engineers
8. Modifying prescriptions
Pharmacists
9. Initial response to inpatients not requiring specialized invasive treatment at night
General practitioner
10. Perioperative wound treatment
WOC nurses
To the best of our knowledge, this is the first study reporting the benefits of working with certified nurse specialists in orthopedics. We believe collaboration with certified nurse specialists benefits orthopedic surgeons, ward nurses, hospitals, and patients and should be promoted further. Nevertheless, we also acknowledge that the number of WOC nurses, though growing, remains smaller in Japan. We are also aware that a majority of WOC nurses work in resource-rich settings such as university and general hospitals.
Limitations
Limitations of this study include the small number of cases and the fact that it was a retrospective, single-center study; it did not include evaluations from patients or facility staff and did not evaluate cost savings. To the best of our knowledge, the study's strength is that this is the first report on the effectiveness of collaboration with certified nurse specialists in the orthopedic surgery field in Japan.
CONCLUSION
Collaboration between WOC nurses and orthopedic surgeons has resulted in shorter hospital stays for patients with malignant soft tissue sarcoma and contributed to more efficient use of personnel.
REFERENCES
1. Gilbert NF, Cannon CP, Lin PP, Lewis VO. Soft-tissue sarcoma. J Am Acad Orthop Surg. 2009;17(1):40–47. doi:10.5435/00124635-200901000-00006.
2. Frobert P, Vaucher R, Vaz G, Gouin F, Meeus P, Delay E. The role of reconstructive surgery after soft tissue sarcoma resection. Ann Chir Plast Esthet. 2020;65(5/6):394–422. doi:10.1016/j.anplas.2020.05.009.
3. Geller DS, Hornicek FJ, Mankin HJ, Raskin KA. Soft tissue sarcoma resection volume associated with wound-healing complications. Clin Orthop Relat Res. 2007;459:182–185. doi:10.1097/BLO.0b013e3180514c50.
4. Baldini EH, Lapidus MR, Wang Q, et al. Predictors for major wound complications following preoperative radiotherapy and surgery for soft-tissue sarcoma of the extremities and trunk: importance of tumor proximity to skin surface. Ann Surg Oncol. 2013;20(5):1494–1499. doi:10.1245/s10434-012-2797-1.
5. Tshuchida T. National survey report on developing a wound, ostomy and continence nurse-led outpatient care model. J Jpn WOCM. 2020;24(3):338–348.
6. Sugama J. The effect of wound, ostomy, and continence nurse care on outcomes in patients with wounds: a multicenter prospective cohort survey of structure and process in the activity of the wound, ostomy, and continence nurses. J Jpn WOCM. 2019;23(3):330–343.
7. Nagano M. Effective pressure ulcer measures at hospital as determined from certified wound, ostomy, and continence nurses perception of influence on quality control and the incidence of pressure ulcers. J Jpn WOCM. 2014;18(3):293–304.
8. Dhar A, Needham J, Gibb M, Coyne E. The outcomes and experience of people receiving community-based nurse-led wound care: a systematic review. J Clin Nurs. 2020;29(15/16):2820–2833. doi:10.1111/jocn.15278.
9. Dutton M, Chiarella M, Curtis K. The role of the wound care nurse: an integrative review. Br J Community Nurs. 2014;(suppl):S39–S40, S42-S47. doi:10.12968/bjcn.2014.19.sup3.s39.
10. Bergersen TK, Storheim E, Gundersen S, et al. Improved clinical efficacy with wound support network between hospital and home care service. Adv Skin Wound Care. 2016;29(11):511–517. doi:10.1097/01.ASW.0000499714.97688.4b.
11. Kelechi TJ, Mueller M, Spencer C, Rinard B, Loftis G. The effect of a nurse-directed intervention to reduce pain and improve behavioral and physical outcomes in patients with critically colonized/infected chronic leg ulcers. J Wound Ostomy Continence Nurs. 2014;41(2):111–121. doi:10.1097/WON.0000000000000009.
12. Wellborn J, Moceri JT. The lived experiences of persons with chronic venous insufficiency and lower extremity ulcers. J Wound Ostomy Continence Nurs. 2014;41(2):122–126. doi:10.1097/WON.0000000000000010.
13. Newbern S. Why your facility needs a full-time certified wound care nurse. Nursing. 2018;48(2):66–68. doi:10.1097/01.NURSE.0000529914.98433.76.
14. Boyle DK, Bergquist-Beringer S, Cramer E. Relationship of wound, ostomy, and continence certified nurses and healthcare-acquired conditions in acute care hospitals. J Wound Ostomy Continence Nurs. 2017;44(3):283–292. doi:10.1097/WON.0000000000000327.
15. Mikami Y. Work style reform for orthopaedic surgeons: basic knowledge for April, 2024. Rinsho Seikei Geka. 2021;56:179–185.






留言 (0)