
記住我








Measurement of patellar height is important in evaluating patello-femoral (PF) instability and PF joint pain (1, 2). The measured patellar height becomes an important indicator when establishing a treatment plan for PF joint pain and instability (3). In general, patellar height is evaluated using lateral radiographs and sagittal plane imaging, which classifies the measurement as normal, patella alta, or patella baja (4). Multiple indices have been defined to measure the height of the patella.
The methods that utilize indirect assessment, such as the Insall–Salvati (IS), Koshino–Sugimoto (KS), Blackburne–Peel (BP), modified Insall–Salvati (MIS), and Caton–Deschamps (CD) have been used (5–8). However, most of these methods rely on bone landmarks, which may not be applicable to pediatric patients whose ossification is not complete (9, 10). The widely used imaging modalities for measuring patellar height include lateral radiographs, computed tomography (CT), and magnetic resonance imaging (MRI). The reliability of patellar tendon measurement on MRI is improved compared to radiographs because it can more clearly display patellar tendon, and PF cartilage (10, 11).
In pediatric patients, data on modalities other than lateral radiographs is limited, and it is often reported in combination with adult data (12, 13). Moreover, there is a focus on the IS method when measuring patellar height in pediatric patients (12, 13). Park et al. compared MRI and lateral radiographs to evaluate the most suitable method among the IS, BP, and KS techniques for measuring patellar height in pediatric patients (10). However, conducting MRI to measure patellar height in all pediatric patients is challenging (9). MRI is less cost-effective compared to radiographs and may require sedation for pediatric patients (9, 13). Recently, Kwak et al. used lateral radiographs to demonstrate differences in the reliability, variability, and applicability of patellar height measurement methods according to age groups in pediatric patients (9). According to their findings, age group and sex influence the choice of methods for patellar height measurement in pediatric patients (9). However, currently, there is no gold standard measurement method for measuring patellar height in pediatric patients.
Therefore, the aim of this study was to determine the inter-observer reliability and intra-observer reliability of various patellar height measurement methods in pediatric patients. In addition, the imaging inter-modality reliability was compared in pediatric patients to assess universal acceptance. This study also assessed which measurement methods were most applicable for different age groups. We hypothesized that different measurement methods and modalities should be used for patellar height measurement in pediatric patients based on age groups.
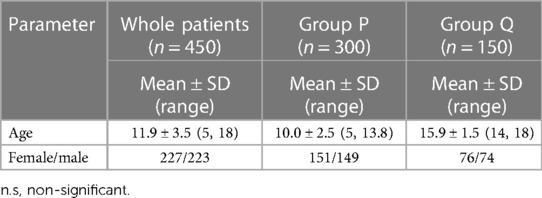
Material & methods PatientsThis study was approved by the hospital's institutional review board. The pediatric patients were retrospectively selected from the record of radiology department. The pediatric patients aged 5–18 years and both lateral knee radiographs and MRI were included. To evaluate patellar height in pediatric population, at first we recruited all the knee MRIs matched with lateral knee radiographs. We identified 580 pediatric patients between January 2012 and September 2022. Then we excluded patients with obvious knee deformities. The exclusion criteria were overall knee disorders as congenital deformities and tumorous condition and trauma as ligament injuries, fractures, previous knee surgeries based on the retrospective review of radiologic studies (10). We also excluded radiographs that deviated excessively from the true lateral view by more than 30° of flexion or rotation (9). After applying the exclusion criteria, a total of 450 pediatric patients (450 knees; 227 males and 223 females) were included in this study. The patients were divided into two groups: Group P (age: 5–13 years) and Group Q (age: 14–18 years) (Table 1) (14, 15).
Table 1. Comparison of the age and gender ratio between Korean pediatric normal and injury.
Image acquisitionPatella height ratios were measured using lateral knee radiographs with a knee flexion of 30°. Radiographs were obtained using a GE Definium 8000 instrument. MRI scans were obtained using a 3.0-Tesla MRI scanner (Philips Medical Systems, Amsterdam, Netherlands). Imaging was performed as previously described (9).
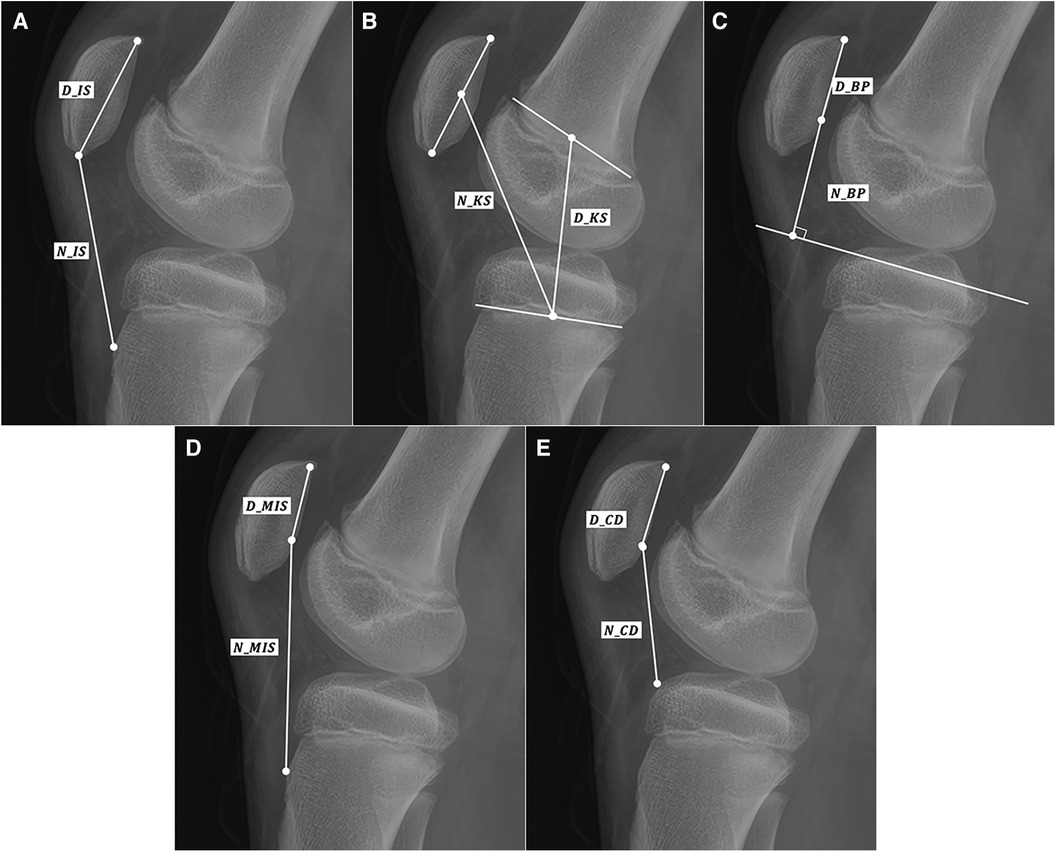
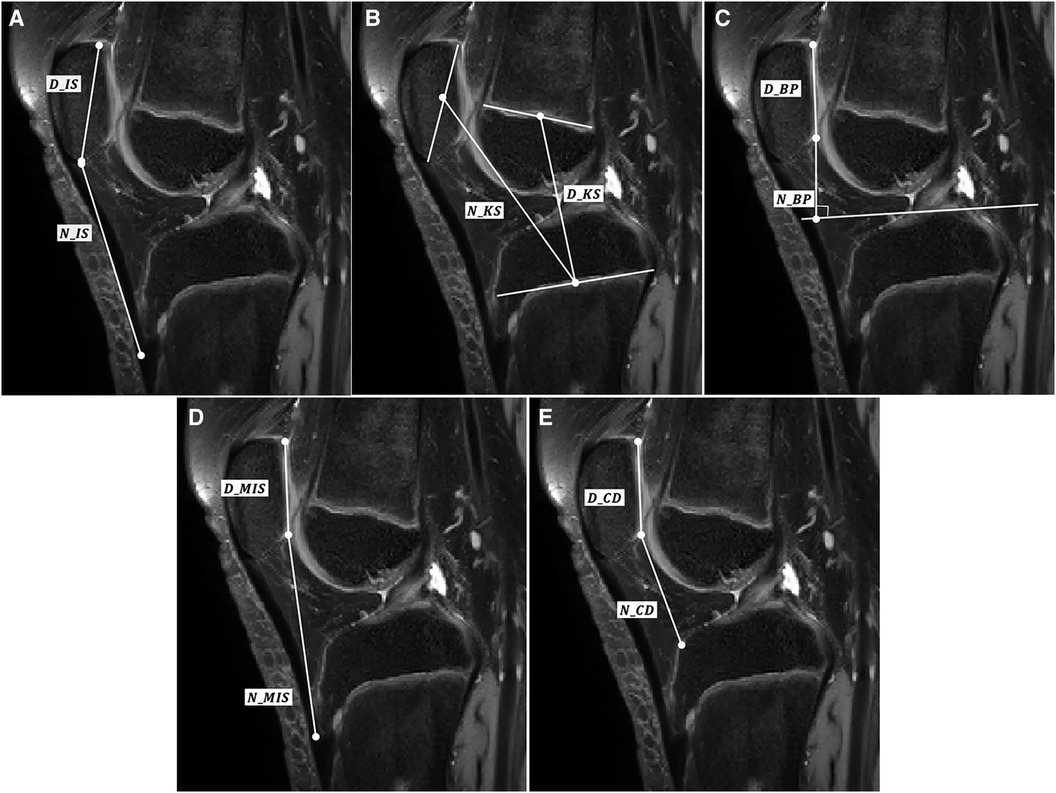
MeasurementsThe patellar height ratios were measured using five methods. Five methods were IS, KS, BP, MIS, CD. The measurement was performed using the Mimics version 17.0 software (Materialise, Leuven, Belgium). Figures 1A, 2A show the IS ratio (N_IS/D_IS) for measuring patellar height on x-RAY and MRI. The IS ratio was calculated as the ratio of N_IS(patella tendon length) to D_IS(patella length). Figures 1B, 2B show the KS ratio (N_KS/D_KS) [7]. The KS ratio was calculated as the ratio of N_KS (the distance between the midpoint of the patella and the midpoint of the proximal tibial physis) to D_KS (the distance between the midpoint of the femoral distal physis and the midpoint of the proximal tibial physis) [17]. Figures 1C, 2C show the BP ratio (N_BP/D_BP). The BP ratio was calculated as the ratio of N_BP (the distance between the inferior edge of patellar articular surface and the tibial plateau line) to D_BP (the length of the patellar articular surface) (5). Figures 1D, 2D show the MIS ratio (N_MIS/D_MIS). The MIS ratio was calculated as the ratio of N_MIS (distance between the inferior edge of the patellar articular surface and the patellar tendon attachment on the tibia) to D_MIS(the length of the patellar articular surface) (6). Figures 1E, 2E show the MIS ratio (N_CD/D_CD). The CD ratio was calculated as the ratio of N_CD (the distance between the inferior edgeof the patellar articular surface and the anterior most point of the tibial plateau) to D_CD (the length of the patellar articular surface) (16). The measurement on MRI was performed on the slice showing the greatest length of the patella. Only in the BP method, tibial plateau line was measured on the slice showing medial plateau.
Figure 1. Schematic representation of (A) IS ratio, (B) KS ratio, (C) BP ratio, (D) MIS ratio, and (E) CD ratio mearued in MRI. (D and N indicate the denominator and numerator, respectively).
Figure 2. Schematic representation of (A) IS ratio, (B) KS ratio, (C) BP ratio, (D) MIS ratio, and (E) CD ratio mearued in lateral knee radiographs.
Each measurement was conducted twice by two raters. The intra-rater reliability, inter-rater reliability and inter-modality reliability were calculated without sampling. Because the patients were pediatric with incomplete ossification, some methods were not applicable. Applicability was defined as the possibility to apply measurement at each age. Applicability of each method was calculated and compared using regression curve and contingency table. The modality-based difference of applicability was also analyzed.
Statistical analysisDescriptive statistics were calculated. Inter-rater, intra-rater and inter-modality reliability were determined using intraclass correlation coefficients (ICC). Applicability was determined using logistic regression. All statistics were calculated using R 4.2.2.
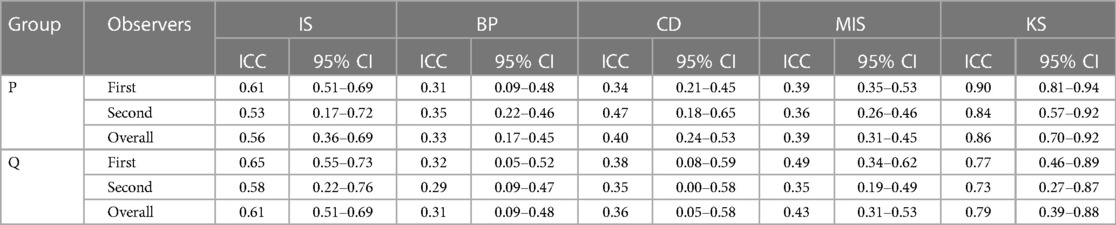
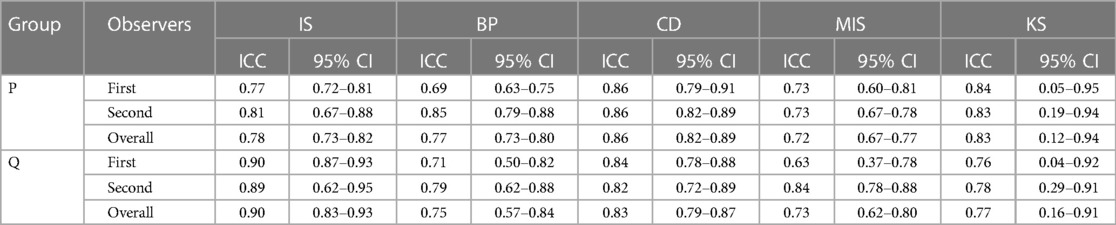
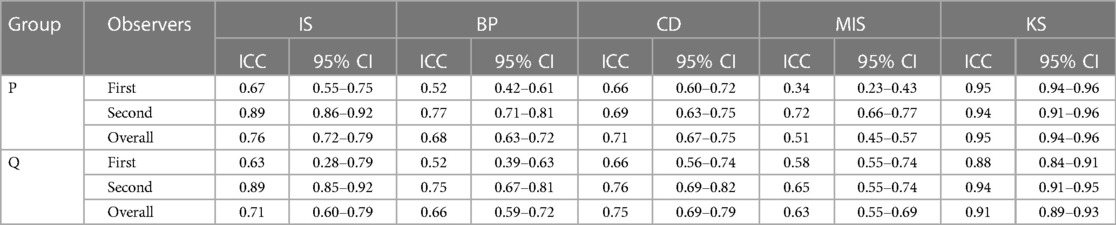
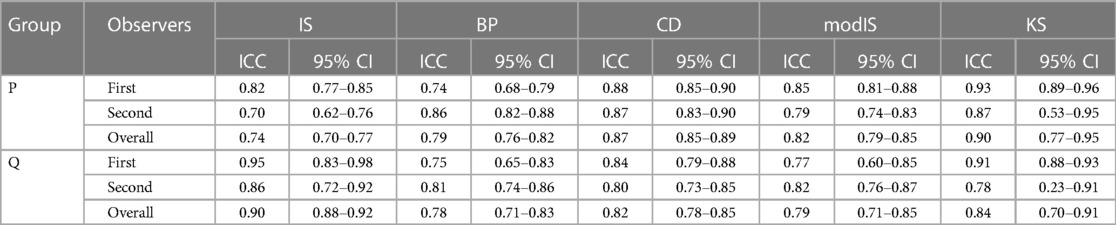
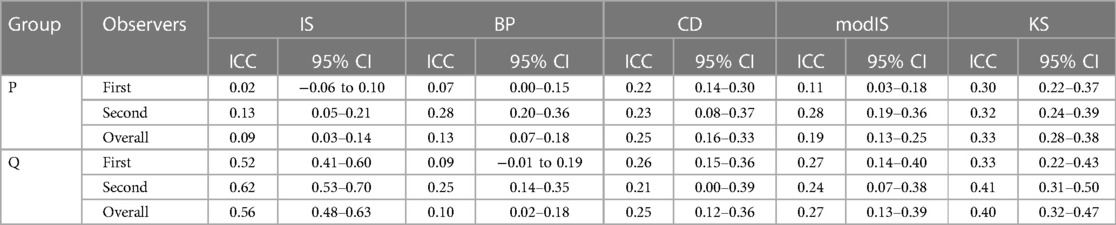
ResultsWhen using MRI, the inter-observer reliability was highest for the KS method (0.86) and lowest for the BP method (0.33) in group P (Table 2). In group Q, the inter-observer reliability was highest for the KS method (0.79) and lowest for the BP method (0.31). The inter-observer reliability for the IS method and MIS method increased with age, while the remaining methods showed a decrease in inter-observer reliability. The KS method showed the highest inter-observer reliability in group P (0.95) and Q (0.91). The MIS method showed the lowest inter-observer reliability in group P (0.51) and Q (0.63). The intra-observer reliability for the CD method and MIS method increased with age, while the remaining methods showed a decrease in intra-observer reliability. When using lateral knee radiography, the inter-observer reliability was highest for the CD method (0.86) in group P, while in group Q, the IS method (0.90) showed the highest inter-observer reliability (Table 3). In terms of intra-observer reliability, the KS method (0.90) showed the highest in Group P, while the IS method (0.84) showed the highest in Group Q (Table 4, 5).
Table 2. Inter-observer reliability of patellar height ratios on MRI.
Table 3. Inter-observer reliability of patellar height ratios on x-RAY.
Table 4. Intra-observer reliability of patellar height ratios on MRI.
Table 5. Intra-observer reliability of patellar height ratios on x-ray.
Table 6 presents the ICCs for evaluating the inter-modality reliability of each measurement method. In P group, the KS method showed demonstrated the highest inter-modality reliability, while the IS method showed the lowest inter-modality reliability. However, in group Q, the IS method showed the highest inter-modality reliability. The applicability of the lateral radiograph in group P for the BP, IS, MIS, CD, KS methods were 55.2%, 49.2%, 38.1%, 55.2%, and 99.7%, respectively. In The applicability of the lateral radiograph in group Q for the BP, IS, MIS, CD, KS methods were 100%, 100%, 100%, 100%, and 100%, respectively. The applicability of the MRI in group P for the BP, IS, MIS, CD, KS methods were 56.5%, 99.7%, 56.5%, 56.5%, and 98.7%, respectively. The applicability of the MRI in group Q for the BP, IS, MIS, CD, KS methods were 100%, 100%, 100%, 100%, and 49.7%, respectively.
Table 6. Inter-modality reliability between MRI and x-ray.
DiscussionThe most significant finding of this study was that the inter-observer reliability and intra-observer reliability of patellar height measurement methods varied depending on the age group.
Moreover, the reliability of patellar height measurement methods can differ across age groups depending on the imaging modality used. Therefore, the applicability of patellar height measurement methods vary depending on the age group.
Previously, researchers tried to validate the reliability of methods for measuring patellar height of pediatric population (17, 18). However, in the case of pediatric patients, these methods may not always be applicable due to the incomplete ossification of bony landmarks.
In the past decade, three notable studies have been conducted to determine reliable patella height measurements in pediatric patients (9, 10, 12). Park et al. conducted a study to determine the most suitable method for measuring patellar height in pediatric patients (10). They considered the applicability, concurrent validity, and reliability of different measurement techniques specific to these age groups (10). In terms of applicability, validity, and reliability, the study found that the IS method was superior in patients older than 13 years (10). However, their study has three limitations. Firstly, they conducted the research with a small sample size of only 108 patients. Secondly, they assumed the IS method based on MRI as the gold standard for validity analysis rather than plain radiograph. Lastly, they did not consider the CD method and MIS method in their study.
Recently, Kurowecki et al. conducted a study investigating whether the IS ratio and patella alta, as determined using MRI, are comparable to those determined using lateral knee radiography in pediatric patients (12). Their results showed a strong correlation between the IS ratio and patella alta measured using both MRI and radiographs in children aged 7.5 years and older (12). However, their study has a significant limitation as it was conducted with a very small sample size of only 49 patients. This limited sample size undermines the generalizability and reliability of the conclusions drawn from the study. Kwak et al. recently conducted a study to evaluate the interobserver and intra-observer reliabilities of five patellar height measurement methods (IS, KS, MIS, BP, and CD) in the assessment of lateral knee radiographs in 425 pediatric patients [9]. The study also aimed to determine which measurement methods were most suitable for specific sex and age groups (9). They concluded that different methods for measuring patellar height should be utilized based on the age group and sex of pediatric patients (9). However, their study was limited to lateral knee radiographs. While lateral knee radiographs have cost-effective advantages compared to MRI, it is important to note that MRI offers additional benefits such as the ability to display patellar tendon length and patellofemoral cartilage. Therefore, in measuring patellar height in pediatric patients with incomplete ossification, MRI may be more suitable.
The goal of this study was to determine the most suitable method for measuring patellar height in pediatric patients. We used inter-observer reliability, intra-observer reliability, imaging modality reliability, and applicability. The study investigated the five most commonly used methods for determining patellar height: IS, KS, MIS, BP and CD. Furthermore, the study divided the pediatric patients into only two age groups, which differs from previous studies that examined patellar height measurements (9, 10). By reducing the number of age groups from three to two, orthopedic surgeons can achieve a more efficient and timely diagnosis.
The IS ratio is a frequently used index for evaluating patellar height in adult patients (12). The IS ratio was initially validated using lateral knee radiographs taken at 30° of flexion in adults. The subsequent studies have investigated its application on computed tomography (CT), MRI, and ultrasound in adult patients (19, 20). The IS ratio has shown good reliability in measuring patellar height in pediatric patients compared to other methods (9, 10, 12). In the previous two studies demonstrated that the IS ratio had the highest reliability in pediatric patients aged 13 years and older (9, 10). Another study suggested that it can be used to diagnose patella alta in patients aged 7.5 years and older (12). These findings align with the results of our study.
Our study found that when using lateral knee radiography, the IS method demonstrated the highest inter-observer and intra-observer reliability in pediatric patients aged 14 years and older. In a previous study, which examined the inter-observer reliability of patellar height measurements using lateral knee radiography, it was found that CD had better reliability compared to BP and IS (21). However, in the current study with patients aged 14 and older, the IS method demonstrated the highest intra-observer reliability compared to CD, BP, KS, and MIS. This finding is in contrast to the previous study. This was not only the case for lateral knee radiography but also for CT and MRI. The previous study also suggested that the intra-observer reliability of a measurement method may be related to rater's experience (21), and another study showed similar results (22).
Interestingly, the reliability of the IS method in the Q group when using MRI did not show the same reliability. In the MRI study, both the P and Q groups demonstrated that the KS method exhibited the highest inter-observer and intra-observer reliability. The KS measurement is the only method that does not use the length of the patella to determine its ratio. However, as the slices change, the shape of the patella can also vary, leading to changes in its length. Therefore, methods that utilize the patellar dimensions are more susceptible to the influence of slice selection in MRI. On the other hand, the KS method uses the position of the centroid instead of the length. The centroid position is less affected by changes in slices compared to the length measurement. This is why we believe the KS method demonstrates higher reliability in MRI compared to other methods.
Verhulst et al. also reported that different observers might select different sagittal slices on different occasions, which can result in decreased intra- and inter-observer reliability (21). Our results for imaging inter-modality reliability demonstrated that IS method in the Q group was the highest. Previous studies have also shown that in patients aged 14 and older, the IS method exhibited the highest inter-modality reliability (10, 22). In our study, when using lateral knee radiography, only the KS method demonstrated an applicability of over 99%. This is consistent with previous research findings (9, 10) indicating that the KS method might be a reliable and widely applicable method for measuring patellar height in lateral knee radiography.
The KS method is the only technique that utilizes the distance between the distal femoral physis and proximal tibial physis. Unlike other methods, it does not rely on the further ossification of the tibial tuberosity or tibial plateau (9, 10). However, when using MRI, the applicability of the KS method decreases by approximately 50%. The reason distal femoral physis is not well visualized when using MRI is because of the imaging technique itself. MRI utilizes a strong magnetic field and radio waves to generate images, which have a better interaction with soft tissues and fluids. However, bone tissue generates a weaker signal in response to the magnetic field, causing bone structures to appear relatively darker on MRI. In contrast, the IS method, which showed an applicability of approximately 50% when using lateral knee radiography in the P group, increased to 100% when using MRI. The patellar tendon, which was not visible in lateral knee radiography, is clearly visible in MRI. This explains why the applicability of the IS method increased to 100% when using MRI.
Our results demonstrate variations in inter-observer reliability and intra-observer reliability based on age groups. Additionally, there are differences in inter-modality reliability among different age groups. Our findings indicate that the applicability varies among age groups depending on the measurement method and imaging modality. This study has several limitations. First, while our study had a larger sample size of pediatric patients compared to previous studies (9, 10, 12), it is important to acknowledge the limitation in terms of ethnic diversity. This suggests a need for future research to include a more diverse representation of participants in future research. Second, due to the retrospective nature of this study, the degree of knee flexion on lateral knee radiographs may not be consistent with that observed on MRI [9–10]. Third, we used same age threshold between male and female patients in spite of different patella ossification age. Further larger-scale analysis should be conducted based on this consideration.
ConclusionsOur results show that the reliability according to the measurement method and imaging technique differs according to the pediatric knee age group when measuring patellar height. Therefore, in the case of pediatric patients, the application of measurement methods and imaging techniques should be tailored to the patient's age. This has important clinical implications in the assessment of pediatric patellofemoral instability and it unscores the importance of methodological considerations in clinical evaluations.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving humans were approved by the Ethics Committee of Asan Medical Center (IRB No. 2022-1251). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributionsYK: Writing – original draft. SS-P: Writing – original draft. AH: Writing – review & editing. KK: Writing – original draft. YG-K: Writing – original draft, Writing – review & editing. JH-N: Writing – original draft. KT-K: Writing – review & editing.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Mj AL-S, Cameron JC. Functional outcome after tibial tubercle transfer for the painful patella alta. Clin Orthop Relat Res. (2002) 396:152–62. doi: 10.1097/00003086-200203000-00024
Crossref Full Text | Google Scholar
2. Monk AP, Doll HA, Gibbons CL, Ostlere S, Beard DJ, Gill HS, et al. The patho-anatomy of patellofemoral subluxation. J Bone Joint Surg Br. (2011) 93:1341–7. doi: 10.1302/0301-620X.93B10.27205
PubMed Abstract | Crossref Full Text | Google Scholar
3. Van Duijvenbode D, Stavenuiter M, Burger B, Van Dijke C, Spermon J, Hoozemans M. The reliability of four widely used patellar height ratios. Int Orthop. (2016) 40:493–7. doi: 10.1007/s00264-015-2908-2
PubMed Abstract | Crossref Full Text | Google Scholar
4. Mortensen AJ, Ludwig TC, Adams BM, Adeyemi TF, Aoki SK. The Blackburne-Peel index for determining patellar height is affected by tibial slope. Arthrosc Sports Med Rehabil. (2021) 3:e359–65. doi: 10.1016/j.asmr.2020.09.026
PubMed Abstract | Crossref Full Text | Google Scholar
6. Grelsamer RP, Meadows S. The modified Insall-Salvati ratio for assessment of patellar height. Clin Orthop Relat Res. (1992) 282:170–6.
8. Yılmaz B, Ozdemir G, Sirin E, Cicek ED, Anıl BS, Bulbun G. Evaluation of patella alta using MRI measurements in adolescents. Indian J Radiol Imaging. (2017) 27:181–6. doi: 10.4103/ijri.IJRI_222_16
Crossref Full Text | Google Scholar
9. Kwak YH, Park SS, Huser AJ, Lim HW, Baki SWA, Koh YG, et al. Evaluation of age group and sex differences in the measurement of patellar height of pediatric knee in a Korean population. Front Pediatr. (2022) 10:1021147. doi: 10.3389/fped.2022.1021147
PubMed Abstract | Crossref Full Text | Google Scholar
10. Park MS, Chung CY, Lee KM, Lee SH, Choi IH. Which is the best method to determine the patellar height in children and adolescents? Clin Orthop Relat Res. (2010) 468:1344–51. doi: 10.1007/s11999-009-0995-3
PubMed Abstract | Crossref Full Text | Google Scholar
11. Diederichs G, Issever AS, Scheffler S. MR imaging of patellar instability: injury patterns and assessment of risk factors. Radiographics. (2010) 30:961–81. doi: 10.1148/rg.304095755
PubMed Abstract | Crossref Full Text | Google Scholar
12. Kurowecki D, Shergill R, Cunningham KM, Peterson DC, Takrouri HSR, Habib NO, et al. A comparison of sagittal MRI and lateral radiography in determining the Insall-Salvati ratio and diagnosing patella alta in the pediatric knee. Pediatr Radiol. (2022) 52:527–32. doi: 10.1007/s00247-021-05207-4
PubMed Abstract | Crossref Full Text | Google Scholar
13. Sistrom CL, Mckay NL. Costs, charges, and revenues for hospital diagnostic imaging procedures: differences by modality and hospital characteristics. J Am Coll Radiol. (2005) 2:511–9. doi: 10.1016/j.jacr.2004.09.013
PubMed Abstract | Crossref Full Text | Google Scholar
15. Phillips CL, Silver DA, Schranz PJ, Mandalia V. The measurement of patellar height: a review of the methods of imaging. J Bone Joint Surg Br. (2010) 92:1045–53. doi: 10.1302/0301-620X.92B8.23794
PubMed Abstract | Crossref Full Text | Google Scholar
17. Aparicio G, Abril JC, Albiñana J, Rodríguez-Salvanés F. Patellar height ratios in children: an interobserver study of three methods. J Pediatr Orthop B. (1999) 8:29–32.10709594
PubMed Abstract | Google Scholar
18. Shin AY, Loncarich DP, Hennrikus WL, Case SR. A comparison of three methods for measuring patella malalignment in children. J Pediatr Orthop B. (1998) 7:303–6. doi: 10.1097/01202412-199810000-00009
PubMed Abstract | Crossref Full Text | Google Scholar
19. Giovagnorio F, Olive M, Casinelli A, Maggini E, Presicci C, Tominaj C, et al. Comparative US-MRI evaluation of the Insall-Salvati index. Radiol Med. (2017) 122:761–5. doi: 10.1007/s11547-017-0781-3
PubMed Abstract | Crossref Full Text | Google Scholar
20. Lee PP, Chalian M, Carrino JA, Eng J, Chhabra A. Multimodality correlations of patellar height measurement on x-ray, CT, and MRI. Skeletal Radiol. (2012) 41:1309–14. doi: 10.1007/s00256-012-1396-3
PubMed Abstract | Crossref Full Text | Google Scholar
21. Smith TO, Cogan A, Patel S, Shakokani M, Toms AP, Donell ST. The intra- and inter-rater reliability of x-ray radiological measurements for patellar instability. Knee. (2013) 20:133–8. doi: 10.1016/j.knee.2012.05.011
PubMed Abstract | Crossref Full Text | Google Scholar
22. Verhulst FV, Van Sambeeck JDP, Olthuis GS, Van Der Ree J, Koëter S. Patellar height measurements: Insall-Salvati ratio is most reliable method. Knee Surg Sports Traumatol Arthrosc. (2020) 28:869–75. doi: 10.1007/s00167-019-05531-1
留言 (0)