
記住我
 Bajer, Ryou, C. Thompson, and Drastich: Novel upper gastrointestinal bleeding sensor capsule: a first human feasibility and safety trial
Novel upper gastrointestinal bleeding sensor capsule: a first human feasibility and safety trial
Abstract
Background/Aims
Bajer, Ryou, C. Thompson, and Drastich: Novel upper gastrointestinal bleeding sensor capsule: a first human feasibility and safety trial
Novel upper gastrointestinal bleeding sensor capsule: a first human feasibility and safety trial
Abstract
Background/Aims
Upper gastrointestinal bleeding (UGIB) is the most common GI condition requiring hospitalization. The present study aimed to evaluate the safety and feasibility of using the PillSense system (EnteraSense Ltd.), a novel diagnostic tool designed for the rapid in vivo detection of UGIB, in human volunteers.
MethodsIn the present study, 10 volunteers swallowed a PillSense capsule, followed by 2 servings of an autologous blood preparation. Participants were monitored for capsule passage, overall tolerability of the procedure, and adverse events.
ResultsThe procedure was completed per the protocol established in the present study in 9/10 cases. In 9 of the subjects, after capsule ingestion, the device indicated the absence of blood with sensor output values of 1. After the ingestion of the first blood mixture, the sensor outputs of all devices increased to a range from 2.8 to 4, indicating that each sensor capsule detected blood. The sensor output remained within that range after the ingestion of the second mixture; however, in one case, the baseline capsule signal was positive, because of a preexisting condition. The passage of the capsule was verified in all patients, and no adverse events were reported.
ConclusionsThe first trial of the PillSense system in human subjects demonstrated the feasibility, safety, and tolerability of utilizing this product as a novel, noninvasive, and easy-to-use triage tool for the diagnosis of patients suspected of having UGIB.
INTRODUCTION Upper gastrointestinal bleeding (UGIB) is one of the most common GI conditions resulting in hospital admissions worldwide. Despite advances in medical techniques, UGIB is still a common cause of morbidity and mortality in patients, as well as a substantial burden for healthcare systems, especially human resources and costs.1,2 Although UGIB can result from both variceal and non-variceal etiologies, a decreasing incidence of UGIB is presumed be due to advances in GI endoscopy, the eradication of Helicobacter pylori, and the widespread use of proton pump inhibitors.2 The diagnosis and treatment of UGIB should be based on individual patient needs, in combination with the resources available and level of expertise of the staff where the patient is receiving medical services. Proper risk stratification is an essential first step in the management of UGIB, and at present, the only available triage tools rely on scoring systems based on common clinical parameters.3,4 Most international guidelines agree on utilizing the Glasgow-Blatchford score (GBS), as opposed to other scales, such as the Rockall score or AIMS65, to evaluate GI bleeding; however, the routine use of the GBS in clinical practice remains questionable.5-10 Endoscopic video capsules have been studied as a triage tool for the diagnosis of UGIB, albeit with ambiguous results on cost effectiveness.11-13 The development of innovative, non invasive triage tools would facilitate the effective risk-stratification of patients with suspected UGIB, minimizing unnecessary hospital admissions and/or urgent endoscopies.11 In the present study, we aimed to evaluate the feasibility and safety results of the first human trial of the PillSense system (EnteraSense Ltd.), a novel, easy-to-use diagnostic device designed for the rapid and accurate detection of UGIB. METHODS Study design and participantsThe present prospective, non-randomized, open-label exploratory clinical study was conducted at a single tertiary care center (Institute for Clinical and Experimental Medicine). All participants provided written informed consent.
Healthy volunteers aged 18 to 60 years were eligible for inclusion in the present study. The exclusion criteria were as follows: circulatory or hemodynamic instability; relevant psychological issues; magnetic resonance imaging scheduled in the near future; current relevant GI-related conditions (e.g., stomach bezoar, known stenosis, or suspected tumors); and a personal history of various GI symptoms and diseases (e.g., dysphagia, esophageal motility disorders, including achalasia, severe esophagitis, Crohn disease, diverticulitis, bowel obstruction, and/or severe constipation). All participants were asked to fast for at least 8 hours prior to the examination.
Investigational device: the PillSense system The PillSense system is a noninvasive, easy-to-use system designed for the real-time detection of GI bleeding as liquid blood and/or hematin. The system consists of 2 components, a single-use, swallowable capsule containing an optical sensor that detects blood as it is propelled through the GI tract, and a wireless bedside receiver (Fig. 1). The capsule is pill shaped, 11×27 mm in size, and battery-powered. The external casing is a biocompatible polycarbonate, which ensures the capsule’s smooth and safe passage through the GI tract, while protecting the capsule from the GI tract environment. The capsule begins to gather data as soon as it is immersed in liquid. In brief, the visible light emitted by the capsule passes through the surrounding liquid, and the wavelengths detected by the sensor (Fig. 2) are analyzed using a proprietary algorithm. The resulting sensor output indicates the presence or absence of blood, and the wireless receiver displays a real-time continuous graph of the sensor output with numeric values ranging from 0 to 5. A cut-off value of 1.8 has been determined to indicate the presence (≥1.8) or absence (Fig. 3). Due to the binary output, the device is not currently designed to evaluate the amount or rate of the bleed. Study procedureThe procedure portion of the present study was performed in an examination room in radiology to ensure easy access to fluoroscopy equipment. After completing the necessary documentation, including signing the informed consent form, each participant ingested the capsule as follows: the subject swallowed the capsule with 100 mL of drinking water, after which the presence of the capsule in the patient’s stomach was visually verified using fluoroscopy. After resting on their left side for 5 minutes while the capsule receiver was monitored, the subject drank the first experimental dose of 25 mL drinking water and 25 mL autologous heparinized blood, obtained from the subject’s own peripheral vein. After a 5 minutes rest, the subject drank a second dose of the aforementioned blood mixture. The entire procedure lasted 15 minutes, including the brief fluoroscopic examination.
Endpoints and data analysisThe primary study endpoints were the demonstration of the feasibility and safety of using the PillSense system in humans, and the validation of its effectiveness in detecting UGIB. The secondary endpoints were the successful delivery and transit of the capsule through the GI tract, and the ability of the subjects to tolerate the capsule. Due to the exploratory nature of the present study, no power analysis was performed, and we primarily used descriptive statistics to evaluate the results. The difference between each patient’s baseline value and the value after they ingested the blood-containing mixture was compared using the Wilcoxon signed-rank test.
Ethical statementsThe protocol for the present study was approved by the ethics committee of the Institute for Clinical and Experimental Medicine and Thomayer Hospital (Regulation number: 29213/20), and registered at ClinicalTrials.gov (NCT05631652). Additionally, the present study adhered to the ethical principles of the Declaration of Helsinki and the International Conference on Harmonization Guidelines on Good Clinical Practice, local regulations, and applicable legislation. All of the study participants provided written informed consent.
RESULTS A total of 10 volunteers were recruited for the present study and underwent the aforementioned procedure in February 2021. All of the subjects were able to swallow the capsule without difficulty, and placement in the stomach was verify fluoroscopically in all 10 patients (100.0%). The study procedure was successfully completed per protocol in 9 of the 10 (90.0%) subjects, and in those 9, the receiver display indicated “no blood detected” immediately following the ingestion of the capsule. The sensor output remained steady at approximately 1, although after the first blood-containing mixture was ingested, the “blood detected” notification was displayed in the 9 subjects who completed the entire protocol, with the sensor output increasing almost immediately to values between 2.8 and 4 (mean, 3.5±0.5). The sensor output continued to display “blood detected” following ingestion of the second mixture, and the values remained steady at 2.8 to 4 (mean, 3.5±0.5) (Table 1). The difference in the output values after the ingestion of each dose of the blood mixture was statistically significant, therefore, compared to the baseline (pIn one case (1/10, 10.0%), a positive “blood detected” signal and a sensor value around 3 occurred shortly after the subject swallowed the capsule. Fluoroscopy was used to locate the capsule, which was adjacent to the pylorus. The “blood detected” message remained after the subject ingested the first dose of the blood-containing mixture, and the output remained steady at a value of 3. Fluoroscopy then showed that the capsule had prematurely passed through the pylorus during data acquisition, and the procedure was terminated after the subject ingested the first dose of the blood-containing mixture. The following day, the patient underwent gastroscopy, which revealed several small petechial hemorrhages. In that case, therefore, an asymptomatic preexisting condition was incidentally revealed by the PillSense capsule, as the subject had no known GI-related medical history or anemia.
The passage of the capsule through the entire GI tract was confirmed in all 10 subjects (100%), either by a photograph of the capsule submitted by the study subject or by an abdominal radiograph obtained a week after the procedure. None of the subjects reported any physical or psychological discomfort during the procedure or the subsequent 21-day follow-up period. No device-related, or unrelated, adverse events were observed during the study or follow-up periods.
DISCUSSIONIn the present study, we presented our first human experience with a novel noninvasive sensor capsule designed for the detection of UGIB. The results that we obtained from 10 healthy volunteers demonstrated the feasibility, safety, and ability of the capsule to detect blood in the upper GI tract. Additionally, the capsule was generally well tolerated and passed smoothly through the GI tract, although in one subject, the capsule detected preexisting UGIB. Given the relatively mild findings of subsequent gastroscopy performed on that subject, the device may be expected to perform with high sensitivity in clinical use, as, of note, the signal remained positive even after the capsule passed into the subject’s duodenum. The sensitivity of the capsule for different segments of the upper GI tract will be investigated in future studies.
Pre-endoscopy risk stratification and triage are essential for the management of patients with suspected UGIB, for which the GBS is currently recommended by all major guidelines.8-10 The real-life utilization of the GBS, however, remains questionable.14 Additionally, the GBS does not consider patient age, and as geriatric patients account for approximately 70% of UGIB admissions, risk stratification might be difficult or skewed, because older individuals don’t typically have antecedent symptoms.15,16 This novel noninvasive sensor capsule, therefore, might be particularly useful in the elderly population and frail patients in general. An accurate, ready-to-use tool with a high negative predictive value for UGIB has the potential to substantially reduce unnecessary upper-GI endoscopies and hospital admissions, particularly to the intensive care unit, substantially decreasing costs.1 On the other hand, however, the cost-utility of an endoscopic video capsule for such diagnosis remains unclear.13 Increased access to GI endoscopy is a critical component of the downward trend of UGIB incidence which has occurred in last 2 decades.2 Availability of endoscopy, however, may be limited in certain settings – not only in remote and rural areas, but also as a result of the “weekend effect”.17,18 In such situations, a sensor capsule option might represent an ideal solution, as it is easy to use and can be handled by nurses. Moreover, the device provides both immediate quantitative sensor values and qualitative (present or absent) results. The capsule could be offered as an alternative to patients who are unable to tolerate traditional upper GI endoscopy, which accounts for up to 35% of cases, or to those who initially refuse endoscopy.19 Finally, the pre-endoscopic differentiation of upper- and lower-GI bleeding can be challenging.20 The prompt exclusion of UGIB with a swallowable sensor capsule, therefore, would facilitate decision making in certain situations. The utilization of the PillSense system in determining small bowel (including duodenal) bleeding, however, has to be addressed in future trials, as the test sequence in this study was only 15 minutes, while mean gastric transit time is estimated to be approximately 44 minutes.21In conclusion, the PillSense system was safe, feasible, and well tolerated in the first human trial, and the results of the present study demonstrated the efficacy of capsules in accurately detecting blood in the upper GI tract. Further studies on patients with suspected UGIB will determine the effectiveness of this sensor capsule in real-life patients. As such, the PillSense system has many possible applications in clinical practice, and is an innovative, noninvasive triage tool.
Fig. 1.PillSense system bedside receiver, touch pen, and swallowable single-use capsule.
 Fig. 2.
Fig. 2.
PillSense capsule and details of the gap where the analysis of the wavelengths of visible light passing through the liquid and reaching the sensor occurs.
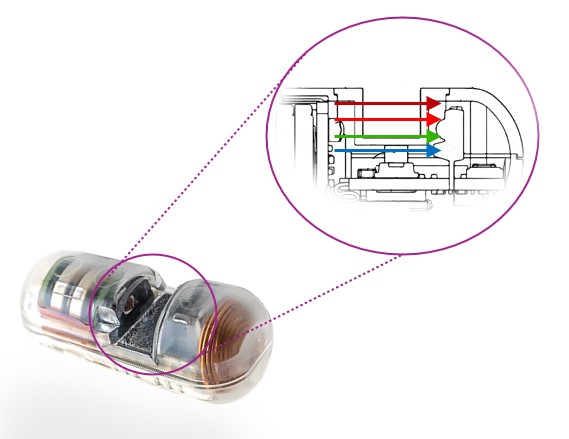 Fig. 3.
Fig. 3.
Real-time data are displayed on the bedside receiver, with an automated interpretation based on a pre-determined cut-off value: ≥1.8, blood detected; <1.8, no blood detected.
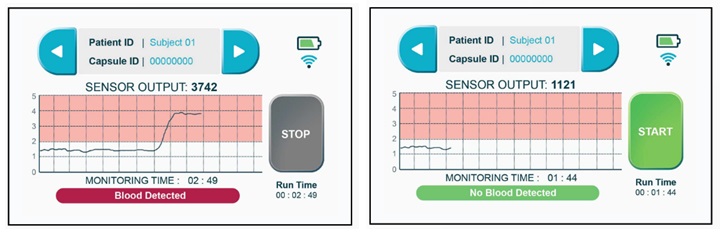
 Table 1.
Table 1.
Summary of data output from the human subjects: sensor values and binary interpretation of the presence or absence of blood as visible on the receiver screen
Before blood ingestion Post drink 1 ingestion (blood=25 mL) Post drink 2 ingestion (blood=25 mL) Sensor value PillSense output Sensor value PillSense output Sensor value PillSense output Subject 1 1 No blood detected 3.5 Blood detected 3.5 Blood detected Subject 2 3 Blood detected 3 Blood detected N/A Subject 3 1 No blood detected 4 Blood detected 4 Blood detected Subject 4 1 No blood detected 4 Blood detected 4 Blood detected Subject 5 1 No blood detected 3.2 Blood detected 3.2 Blood detected Subject 6 1 No blood detected 4 Blood detected 4 Blood detected Subject 7 1 No blood detected 3 Blood detected 3 Blood detected Subject 8 1 No blood detected 3 Blood detected 3 Blood detected Subject 9 1 No blood detected 3.8 Blood detected 3.8 Blood detected Subject 10 1 No blood detected 2.8 Blood detected 2.8 Blood detected REFERENCES 1. Peery AF, Crockett SD, Murphy CC, et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2021. Gastroenterology 2022;162:621–644. Share:
METRICS
Share:
METRICS 
留言 (0)