
記住我
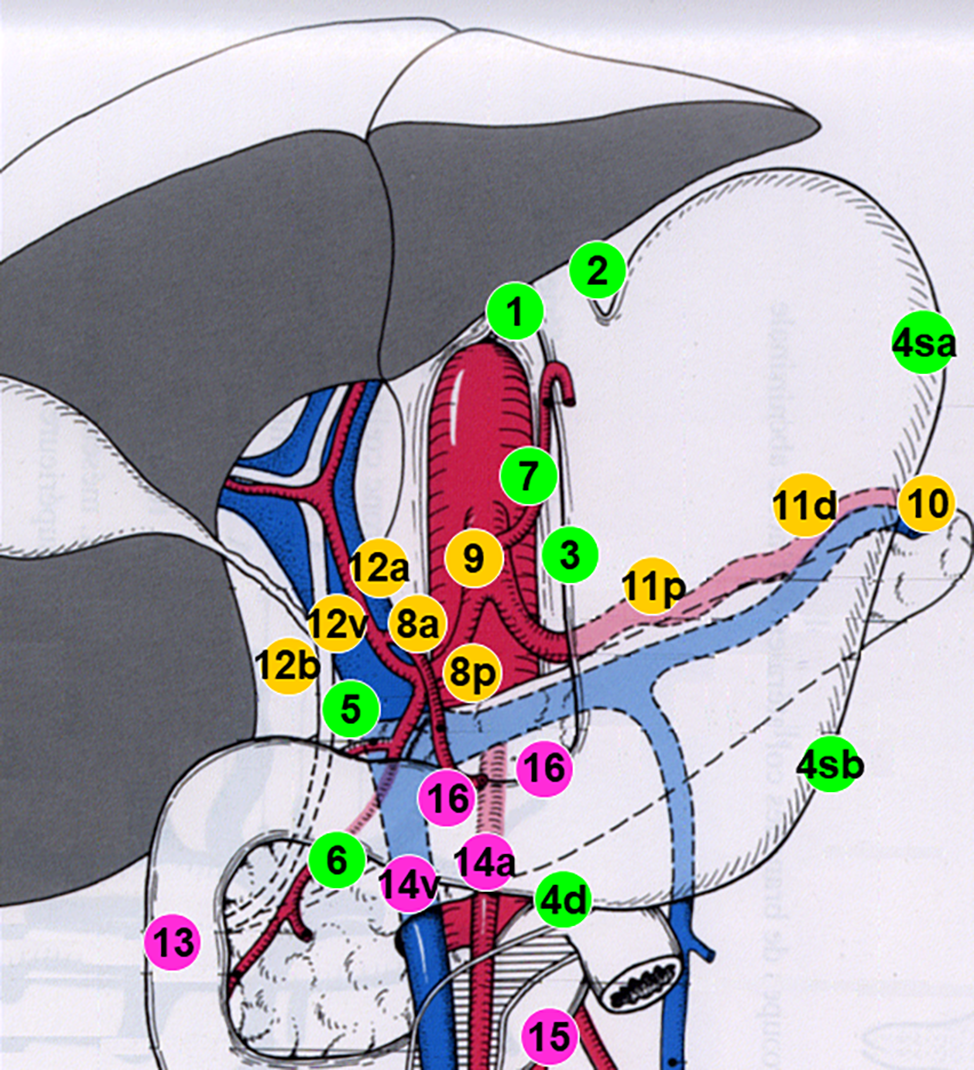





Patients who underwent surgery for breast cancer between 1997 and 2021 were retrospectively studied. Patients were divided into three groups: 1-those who had undergone breast-conserving surgery (BCS) (245 patients, 71.3%), 2-those who had undergone mini-LDF after breast-conserving surgery (38 patients, 11.02%), and 3- those who underwent reconstruction with implants after subcutaneous mastectomy(M + I) (61 patients, 17.68%). The same senior surgeon performed all breast-conserving surgeries, mini-LDFs, and subcutaneous mastectomies, and reconstruction with implants was performed by a total of 3 breast specified plastic surgeons. The patients were called for a follow-up examination, and their photos were taken at the same distance with the same camera (Sony Alpha A6000) and in the same light. The photographs taken were shown to an independent breast surgeon and a plastic surgeon who was not included in the surgeries, and they were asked to evaluate and rate them according to the Japanese Breast Cancer Society Cosmetic Evaluation Scale (JBCS cosmetic evaluation scale) (Table 1). The same images were transferred to the computer and scored using BCCT.core version 3.0 software. After manually placing anatomical landmarks in the program, they are automatically evaluated for asymmetry, color, and scar condition and classified into four groups: excellent, good, fair, and poor [11] (Fig. 1).
Table 1 Japanese cosmetic evaluation form used by plastic and general surgeonsFig. 1
Examples of different patient scores obtained by BCCT. Core software
RadiotherapyRT was applied in 37 patients (97.4%) in the mini-LDF group and in 233 patients (94.7%) in the BCS group, whereas RT was applied in 27 patients (44.3%) in the M + I group.
Surgical techniqueBreast-Conserving Surgery (BCS)In patients who underwent breast-conserving surgery, inframammary sulcus or areolar incisions were used depending on the location of the tumor. The mass was excised with a solid margin, the remaining tissue was approximated to create no interstitial space, and a primary suture was performed. An incision was made separately from the axilla for sentinel lymph node biopsy.
Mini-LDFAfter the patient was positioned, the tumor and sentinel lymph node were harvested and sent for intraoperative pathological evaluation. Then, the superior part of the latissimus dorsi muscle was found, separated from the site where it adhered to the humerus, and dissected to the scapula. After the flap was removed, a subcutaneous tunnel was prepared between the site where the tumor had been excised and the muscle, the neurovascular bundle was preserved, the tunnel was traversed, and the cavity defect created there was filled (see the related article for detailed information on surgical technique) [13].
Subcutaneous mastectomy + implantSince it provides easy access to the axilla, subcutaneous mastectomy was performed through a lateral radial incision, implants were placed behind the pectoral muscle, acellular dermal matrix (Tutopatch) was used in 51 patients, an expander was placed in 10 patients, and reconstruction was performed with permanent implants in the remaining 51 patients.
Cosmetic evaluationJapanese Breast Cancer Society (JBCS) Cosmetic Evaluation Scale, developed by Sawai et al. [16] in 2004 and supported by the Japanese Breast Cancer Society, was used to assess cosmetic outcomes. It scores the following eight items and conducts evaluations with the highest total score of 12 points: breast size (0–2 points), breast shape (0–2 points), scar (0–2 points), breast firmness (0–2 points), nipple-areola complex (NAC) size/ shape (0–1 point), NAC color tone (0–1 point), nipple position (0–1 point), and position of the maximum descent point of the breast (0–1 point). In this method, total scores of 11 to 12, 8 to 10, 5 to 7, and 0 to 4 points were defined as "excellent," "good," "fair," and "poor." An "excellent" rating means the treated breast was nearly identical to the untreated breast. A "good" rating means that the treated breast differed slightly from the untreated breast. A "fair" rating means that the treated breast was not seriously distorted but clearly different from the untreated breast, while a "poor" rating means that the treated breast was seriously distorted. Although this scale was easy to use, it was subjective [17].
The objective evaluation was used as an objective tool for cosmesis evaluation. The software analyzed cosmetic outcomes by marking the jugular notch and both nipples and outlining the breasts with lines. The endpoints included the breast retraction assessment, lower breast contour, upward nipple retraction, breast compliance evaluation, breast contour length difference, breast area difference, and breast overlap difference. In addition, the breast image was divided into 12 fractions by 30 degrees each. Color and scar assessments were conducted simultaneously to compare the left and right breasts. The software automatically conducted all the items. Eventually, four staged evaluation results are procured as follows: "excellent," "good," "fair," and "poor." [17].
Statistical analysisThe statistical analysis was performed using the IBM SPSS version 22 program package. The variables were examined through visual methods like histograms and probability plots and analytical methods like Kolmogorov–Smirnov/Shapiro–Wilk's test to assess whether they were normally distributed. Descriptive analyses were presented using medians for non-normally distributed parameters such as age, tumor size, follow-up time, and ordinal variables. The Chi-square test was used to compare proportions in different groups. Since JBCS Cosmetic Evaluation Scale Scores were not normally distributed, Kruskal‒Wallis tests were conducted to compare these parameters. The interrater reliability between the plastic surgeon, breast surgeon, and BCCT. core scores were determined using the intraclass correlation coefficient (ICC). To identify factors associated with poor cosmetic outcomes, the results obtained with the JBCS Cosmetic Evaluation Scale and BCCT. core software were re-grouped as poor and others. Logistic regression (enter) was used for univariate analyses to identify variables associated with poor outcomes for every parameter. For multivariate analyses, possible factors identified with univariate analyses were further entered all together into logistic regression analyses (Backward LR) to determine independent predictors of poor cosmetic outcomes. Model fit was assessed using Hosmer–Lemeshow's goodness of fit statistics. A 5% type-I error level was used to infer statistical significance.
留言 (0)