
記住我



Schizophrenia is a chronic disease that impacts all areas of life and affects around 1% of the global population.1 Schizophrenia usually begins in early adulthood. The most common symptoms are an impaired perception of reality, and changes such as hallucinations, delusions, disorganized thinking, emotional withdrawal, stereotyped thinking, anxiety, depression, and active social avoidance.2 As a result, social functioning is negatively affected in many patients, increasing the risk of unemployment, social isolation, and poverty.3
Antipsychotics were first developed in the 1950s and used to treat acute psychotic episodes and as a long-term maintenance treatment to prevent relapses and maximize functioning and quality of life. Today, antipsychotics are prescribed to treat psychotic episodes, prevent relapses, and provide symptom control. First-generation antipsychotics are effective and still widely used, although they are associated with a high incidence of adverse events (AEs), while second-generation antipsychotics are generally better tolerated and are an effective treatment alternative.3
Poor adherence to antipsychotic treatment is common among patients with schizophrenia, causing an increase in the risk of relapse or hospitalization.4 In this situation, after initial control of the acute phase of psychosis, long-acting injectable (LAI) antipsychotics provide stable therapeutic plasma concentrations that can prevent relapse and ensure benefits for patients and their families. By eliminating the need to take daily oral antipsychotic medication, LAI antipsychotics increase adherence rates, reduce treatment discontinuation, and therefore help prevent relapses and hospitalizations; they also avoid gastrointestinal absorption problems and circumvent first-pass hepatic metabolism.5–8
Aripiprazole, an atypical antipsychotic agent that acts as a partial agonist at dopamine D2 receptors, has been proven to be effective and well-tolerated.9,10 Several studies have shown that aripiprazole once monthly 400 mg (AOM400) effectively reduced hospitalization time and improved patient functionality.11–13 Its safety profile was assessed in clinical trials that showed good tolerability and a low incidence of AEs.14 The initial single-injection start regimen consists of a single intramuscular injection with concomitant oral aripiprazole administration for 14 consecutive days to maintain therapeutic drug concentrations.15 The two-injection start (TIS) initiation regimen was recently approved by the European Medicines Agency of the European Union,15 with only a single 20 mg oral dose on the first day alongside 2 intramuscular injections at separate sites. This AOM400-TIS treatment initiation was supported by a pharmacokinetic simulation showing absorption and distribution comparable to AOM400, with similar plasma levels,16 which could potentially be expected to reduce nonadherence to treatment. This treatment initiation strategy for AOM400 has not yet been approved by the US Food and Drug Administration nor is it included in the US prescribing information for AOM400.
There is a need for information on the benefits and effects in real clinical practice of this alternative initiation regimen, given its relatively recent approval. The aim of the SaTISfy study [study of aripiprazole TIS initiation regimen] was to collect psychiatrists’ perceptions to determine the potential benefits of the AOM400-TIS in patients with schizophrenia in Spanish clinical practice. The study also assessed psychiatrists’ perceptions about the safety and tolerability of AOM400-TIS initiation, their degree of satisfaction with this treatment strategy, and the reduction of health care resources associated with using AOM400-TIS, including the potential reduction in hospitalization times. General characteristics of patients with schizophrenia and the management of this disease in Spanish clinical practice were also addressed.
METHODS Study Population and DesignSaTISfy was an ecological study with aggregated data. The data source was the experience of psychiatrists treating patients with schizophrenia in a real clinical setting collected through a survey; no data were extracted from medical charts. Given the retrospective nature of the study, all treatments were administered according to routine clinical practice.
Based on the prevalence of schizophrenia in Spain, an estimated sample size of 250 patients was calculated. As each psychiatrist was asked to give an aggregated answer based on the last 5 patients, the sample size was set at 50 psychiatrists. The participants were selected to ensure a representative sample from acute units of departments of psychiatry in hospitals from different regions of Spain, both rural and urban.
The study was approved by the Ethics Committee of Hospital Clínico San Carlos (Madrid, Spain). All participating psychiatrists provided written consent to participate and for their answers to be used by the sponsor of the study. The participants received a small economic incentive for their participation in the study. Surveys were anonymized to avoid undue influence on participants’ responses.
Survey and Data CollectionThe study coordinators created the survey questions based on their clinical experience and a literature review concerning critical aspects of the management of schizophrenia, treatment with AOM400, and initiation with TIS.
A total of 50 psychiatrists with experience using AOM400-TIS answered an online survey between November 2021 and January 2022. Each participant received an information leaflet that described the study objectives and, after agreeing to participate, each participant received a personalized link to access and complete the online survey anonymously. The online platform remained open until the expected sample size was reached. Once 50 psychiatrists had accessed the online survey, access to the survey was locked and recruitment efforts were stopped. Participants had to answer all questions. The survey contained 41 questions divided into 4 parts: (1) 6 questions on the physician’s experience of treating patients with schizophrenia and the average duration of hospitalization, (2) 14 questions regarding the treatment of the psychiatrist’s last 5 patients with schizophrenia, (3) 8 questions on the last 5 patients treated with AOM400, and (4) 13 questions on the last 5 patients who initiated treatment with the AOM400-TIS regimen and the patients’ average duration of hospitalization. The psychiatrists were instructed to only consider the last 5 patients who fulfilled the requirement for that survey section: for section (2), patients with schizophrenia; for section (3), patients treated with AOM400; and for section (4), patients who initiated treatment with the AOM400-TIS regimen.
Statistical ConsiderationsA descriptive analysis of the data was performed. Absolute and relative frequencies of responses to questions related to the psychiatrists’ experience, together with means and SDs, were calculated. Means and SDs were similarly calculated for questions related to the number of patients (out of the last 5 patients treated by the participants in the study). For multiple-choice questions, the number of respondents is presented with the absolute frequencies, together with the mean percentage and SD attributed to each factor by those respondents; percentages may add up to more than 100%.
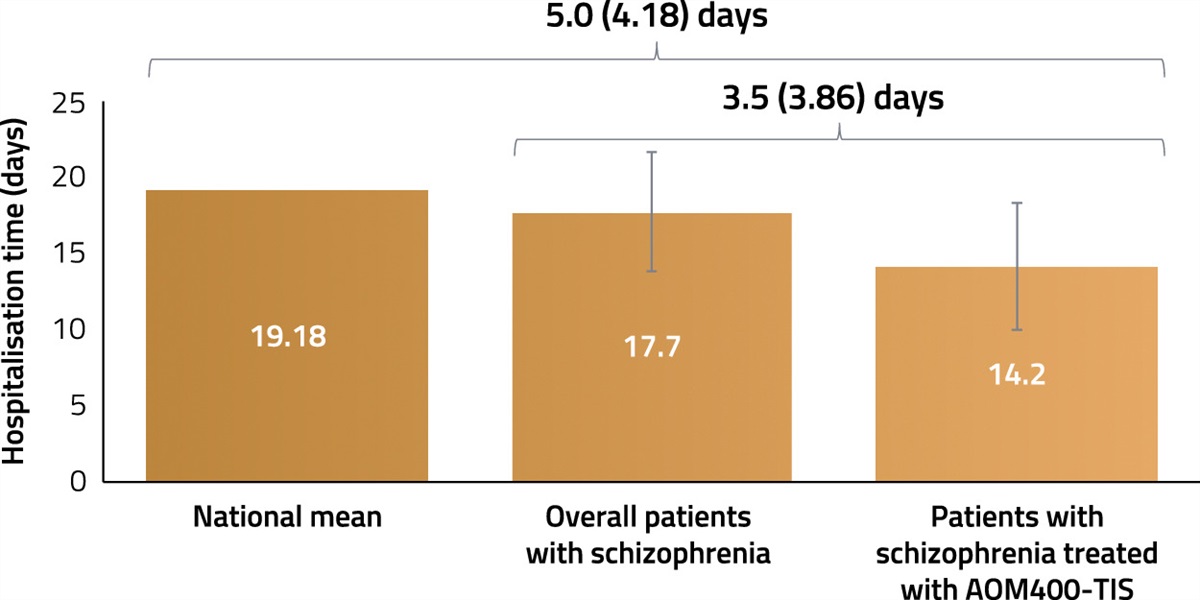
The total population of the study—the 50 participating psychiatrists—was defined as the “full analysis set” (FAS) and was the population considered for analysis unless otherwise stated. Each participant provided aggregated data for the last 5 patients treated. No information from individual patients was collected or analyzed. The mean duration of hospitalization of patients with schizophrenia was analyzed in a subpopulation defined as “full analysis set 2” (FAS2). FAS2 excluded those psychiatrists who reported hospitalization times of 30 days or longer, as these were considered extreme values and could not be compared with data from the national registry which only includes hospitalization times shorter than 30 days for acute units. The FAS2 population included a total of 45 psychiatrists. Therefore, the mean hospitalization time of patients who initiated treatment with AOM400-TIS was compared with the mean hospitalization time of acute patients in psychiatry units in Spain and the mean hospitalization time of patients with schizophrenia in hospitals participating in the study who were hospitalized for fewer than 30 days. According to the literature and available national registry data, the average length of hospitalization in psychiatric units in Spain was estimated to be 19.18 days.17 An average cost of 436€/d (Euros/d) of hospitalization in Spain in 2021 was used to calculate the estimated cost reduction when AOM400-TIS initiation was chosen over other treatments. This cost was estimated using the EPPI-Centre software with 420.90€ used as the reference, which was reported as the cost in 2019.18
The statistical analyses were performed with SAS v9.4 under SAS Enterprise Guide v8.3.
RESULTS Characterization of Participants, Patients With Schizophrenia, and Their TreatmentsPatients with schizophrenia comprised a mean of 44.1% of their caseload among the psychiatrists taking part in this study. All answers provided referred to patients with schizophrenia. Most of the psychiatrists participating in the study (98%) claimed that they lacked a protocol specifying a minimum hospitalization time for patients with schizophrenia in their hospital. According to the psychiatrists, patients with schizophrenia were on average 30.5±7.6 years old. Their most common symptoms were delusions and poor social interactions, for a mean of 4.6 and 4.1 out of 5 patients, respectively, and approximately half of them were obese (Table 1). A mean of 1.8±1.09 out of 5 patients had a family history of schizophrenia. Most of the patients (4.0±0.91) showed insufficient adherence to their treatment, and fewer than half (1.7±0.81) had been hospitalized during the past year. According to 96% of the psychiatrists, most of their patients were smokers (4.1±0.85), and, according to 98% of psychiatrists, more than half of their patients (2.7±0.92) consumed other substances (Table 1). The psychiatrists indicated that most of their patients had some level of cognitive impairment (Table 1).
TABLE 1 - Clinical Characteristics of Patients Diagnosed With Schizophrenia Patient characteristics Number of patients, mean±SD* Number of respondents, n (%)† Age, y 30.5±7.6 50 (100.0) Positive symptoms Delusions 4.6±0.63 50 (100.0) Suspiciousness/persecutory delusions 3.8±0.87 49 (98.0) Hallucinatory behavior 3.3±1.22 49 (98.0) Conceptual disorganization 3.0±1.13 45 (90.0) Excitement 2.9±1.43 33 (66.0) Hostility 2.6±1.04 42 (84.0) Other 1 1 (2.0) Negative symptoms Poor social interactions 4.1±0.93 49 (98.0) Passive/apathetic social withdrawal 3.2±1.13 49 (98.0) Difficulty in abstract thinking 3.2±1.17 39 (78.0) Blunted affect 2.7±1.13 44 (88.0) Lack of spontaneity and flow of conversation 2.7±1.04 38 (76.0) Stereotyped thinking 2.0±1.14 25 (50.0) Comorbidities Obesity 2.1±1.09 41 (82.0) Cardiovascular disease 1.4±0.91 25 (50.0) Diabetes mellitus 1.2±0.91 25 (50.0) Hepatitis C 0.6±0.70 10 (20.0) HIV 0.4±0.74 8 (16.0) Other 1.3±0.71 8 (16.0) Psychiatric comorbidities Tobacco use disorder 4.1±0.85 48 (96.0) Substance use disorder 2.7±0.92 49 (98.0) Anxiety disorder 1.6±1.00 12 (24.0) Depression 1.5±0.51 20 (40.0) Obsessive-compulsive disorder 0.8±0.45 12 (24.0) Posttraumatic stress disorder 0.6±0.55 5 (10.0) Other 1.0±0.00 2 (4.0) Cognitive impairment (n=49) Mild 2.2±1.12 49 (100.0) Moderate 1.7±0.65 31 (63.3) Severe 1.2±0.40 11 (22.4) No impairment 2.1±1.10 20 (40.8)*Out of the last 5 patients with schizophrenia treated by the psychiatrist.
†Number of psychiatrists answering this question.
Most of the psychiatrists (n=43) chose aripiprazole as the first treatment for half of their patients (2.5±0.93), irrespective of possible history of drug abuse [ie, of the 215 patients of the 43 psychiatrists (43 x 5), about half of them received aripiprazole as their first treatment] (Table 2). Most of the patients (4.0±1.08) were treated with benzodiazepines or hypnotics (Table 2). Few patients (0.7±1.08) were receiving cognitive-behavioral therapy.
TABLE 2 - Treatments Prescribed for Patients With Schizophrenia Treatments Number of patients, mean±SD* Number of respondents, n (%)† First treatment (n=45) Aripiprazole 2.5±0.93 43 (95.6) Olanzapine 1.2±0.66 16 (35.6) Risperidone 1.2±0.56 15 (33.3) Paliperidone 1.0±0.00 36 (80.0) Amisulpride 1.0±1.00 3 (6.7) Quetiapine 0 1 (2.2) Other‡ 1±0.00 4 (8.9) First treatment for those with drug abuse (n=48) Aripiprazole 2.6±1.14 45 (93.8) Paliperidone 1.5±0.67 33 (68.8) Olanzapine 1.5±0.89 20 (41.7) Risperidone 1.4±0.73 9 (18.8) Quetiapine 2 1 (2.1) Amisulpride 1 1 (2.1) Other§ 1.0±1.00 2 (4.2) Concomitant medication (n=50) Benzodiazepines or hypnotics 4.0±1.08 50 (100.0) Mood stabilizer 1.7±0.72 22 (44.0) Antidepressants 1.5±0.59 25 (50.0) Anticholinergics 1.2±0.44 13 (26.0) Other 1 1 (2.0)*Out of the last 5 patients with schizophrenia treated by the psychiatrist.
†Number of psychiatrists answering this question.
‡Lurasidone (n=1), cariprazine (n=1), and clozapine (n=2).
§Cariprazine (n=1) and clozapine (n=1).
The main factors leading to hospitalization of patients with schizophrenia were low adherence to antipsychotic treatment and substance use as reported by 100% and 92% of the psychiatrists, respectively (Table 3). Several factors were considered in treatment selection, with prevention of relapses (94%) and reduction in positive symptoms (82%) being predominant. Treatment choice was mainly based on the psychiatrists’ own clinical experience (96% of psychiatrists) (Table 4).
TABLE 3 - Factors Promoting Hospitalization of Patients With Schizophrenia Factors Percentage, mean±SD* Number of respondents, n (%)† Low adherence to antipsychotic treatment 58.3±21.40 50 (100.0) Symptom exacerbation 46.5±31.23 39 (78.0) Substance use 37.0±18.96 46 (92.0) Lack of efficacy of antipsychotic treatment 19.4±16.94 17 (34.0) Psychosocial stress 17.9±13.83 22 (44.0) Antipsychotic adverse events 8.9±8.45 10 (20.0) Other medical disease 5.8±0.40 4 (8.0) Anosognosia 2.0 1 (2.0)*Percentage attributed to each factor.
†Number of psychiatrists answering this question.
*Percentage attributed to each factor.
†Number of psychiatrists answering this question.
‡Social and familiar environment and physical health.
Patients treated with AOM400 were, on average, 29.4±5.16 years old. According to the psychiatrists, the mean time from diagnosis to treatment initiation with AOM400 was 4.5±3.23 years, and patients were hospitalized for a mean of 18.3±7.70 days. Most of the psychiatrists (96%) answered that more than half of their patients (3.3±1.16) were previously treated with an oral antipsychotic before initiating AOM400. According to 60% of the psychiatrists, approximately half of their patients were previously treated with aripiprazole (2.6±1.38), while 72% reported previously treating 1.8±0.82 out of 5 patients with olanzapine (Table 5). The main reason reported for switching from a previous treatment was lack of adherence (92%), and the main objective reported for switching was to improve adherence to antipsychotics (94%) (Table 6).
TABLE 5 - Previous Antipsychotic Treatments Before AOM400 Initiation (N=50) Previous treatments Number of patients, mean±SD* Number of respondents, n (%)† Type of previous treatment Oral antipsychotic 3.3±1.16 48 (96.0) Combination of antipsychotics 2.1±1.26 28 (56.0) Other ILP 1.2±0.49 32 (64.0) None 2.0±1.00 3 (6.0) Previous antipsychotic Aripiprazole 2.6±1.38 30 (60.0) Olanzapine 1.8±0.82 36 (72.0) Combination of antipsychotics 1.8±1.03 17 (34.0) Risperidone 1.7±1.02 18 (36.0) Paliperidone 1.5±0.71 34 (68.0) Quetiapine 1.3±0.50 4 (8.0) Clozapine 1.0±0.00 2 (4.0) Other‡ 1.0±0.00 3 (6.0)*Out of the last 5 patients treated with AOM400.
†Number of psychiatrists answering this question.
‡Fluphenazine depot (n=1), lurasidone (n=1), and without previous treatment (n=1).
AOM400 indicates aripiprazole once monthly 400 mg.
*Out of the last 5 patients treated with AOM400.
†Number of psychiatrists answering this question.
AOM400 indicates aripiprazole once monthly 400 mg.
All patients treated with AOM400-TIS were previously stabilized with oral aripiprazole. Lack of adherence to the previous treatment was the main patient characteristic considered when choosing AOM400-TIS initiation, according to 98% of the psychiatrists (Table 7). Consequently, 88% of psychiatrists chose AOM400-TIS to improve adherence, in 4.6±0.90 out of 5 patients (Table 7). Most of the psychiatrists (80%) administered AOM400-TIS during hospital admission after stabilizing the symptoms that led to the hospitalization (Table 7). On average, patients were discharged 6.6±5.11 days after being initiated on AOM400-TIS. The main reasons for hospital discharge were improvement of positive symptoms (98% of psychiatrists; mean of 4.5±0.96 patients), followed by improvement in functionality (72% of psychiatrists; mean of 4.0±1.06 patients), and reduction of negative symptoms (34% of psychiatrists; mean of 3.5±1.23 patients).
TABLE 7 - Treatment Initiation With AOM400-TIS Number of patients, mean±SD* Number of respondents, n (%)† Reason for initiating with AOM400-TIS (n=50) Lack of adherence to previous treatment 4.0±1.15 49 (98.0) High hospitalization rate 2.8±1.54 31 (62.0) Oral treatment refusal 3.2±1.45 29 (58.0) Other 3.0±1.73 7 (14.0) AOM400-TIS treatment initiation (n=49) During hospital admission, after patient stabilization 3.7±1.56 40 (81.6) Before hospital discharge 2.6±1.72 18 (36.7) Halfway through the hospitalization period 2.1±0.94 21 (42.9) After testing oral tolerance to the treatment 3.0 1 (2.0) Reason for choosing AOM400-TIS (n=50) Improve treatment adherence 4.6±0.90 44 (88.0) Avoid concomitant oral aripiprazole 4.3±1.16 24 (48.0) Reduce hospitalization time 4.0±1.35 38 (76.0) Other 3.7±2.31 3 (6.0)*Out of the last 5 patients treated with AOM400-TIS.
†Number of psychiatrists answering this question.
AOM400-TIS indicates aripiprazole once monthly 400 mg two-injection start regimen.
The mean hospitalization time reported by the psychiatrists in the study was reduced by 3.5±3.86 days for their patients who initiated treatment with AOM400-TIS (14.2±4.18 d) compared with their patients with schizophrenia generally, regardless of their treatment (17.7±3.93 d). Compared with the national mean hospitalization time of patients in acute psychiatry units in Spain, which was estimated to be 19.18 days (2010–2015),17 the hospitalization period was reduced by 5.0±4.18 days in the patients who initiated treatment with AO
留言 (0)