
記住我


Childhood-onset systemic lupus erythematosus (SLE) is characterized by a persistent autoimmune disorder with inflammatory manifestations affecting multiple organ systems. The primary treatment medication for pediatric SLE involves glucocorticoids and other immunosuppressive medications. However, the prolonged administration of these immunosuppressive medications is associated with the occurrence of recurrent infections. Among these infections, pulmonary infection is identified as a prominent cause of mortality among children with SLE.1
Pneumocystis jirovecii (formerly Pneumocystis carinii) pneumonia (PJP), an opportunistic infection causing high mortality, has shown an increasing incidence in SLE patients over the past 2 decades.2,3Pneumocystis jirovecii pneumonia primarily affects individuals with impaired immune systems, including those diagnosed with AIDS, individuals undergoing chemotherapy for certain malignancies, and those using immunosuppressants after organ transplants or for treating autoimmune diseases.4 In a comprehensive review, 121 cases of PJP were identified among 76,156 SLE patients between 1987 and 2006, with an estimated frequency of 15.88 per 10,000 patients.2 Weng et al.3 found a frequency of 58/10,000 SLE patients with PJP from 2000 to 2011. Notably, the mortality rate of PJP in SLE patients is high, ranging from 36% to 60%.5,6 Although the actual incidence and mortality of PJP in children with SLE remain undetermined, childhood-onset SLE generally exhibits a more severe clinical trajectory compared with adult-onset cases.7,8 Therefore, it is crucial to identify children with SLE at a higher risk of developing PJP to provide timely preventive treatment.
There are several risk factors associated with PJP in adult SLE, with one of the most important being the prolonged use of high-dose immunosuppressive drugs, especially glucocorticoids.9–12 Studies indicate that PJP usually occurs after 4 weeks of high-dose steroid treatment.13 Therefore, various researchers have suggested that individuals with compromised immune function, prescribed a daily dose of prednisone equal to or exceeding 20 mg for at least 4 weeks, might consider utilizing trimethoprim/sulfamethoxazole (TMP/SMX) as a prophylactic measure against PJP.9,13,14 In addition, the risk of PJP in adult patients with SLE is linked to other factors, including a decrease in lymphocyte count,9,15,16 greater Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores,9 and the administration of immunosuppressants such as cyclophosphamide (CYC),10,17 mycophenolate mofetil,18 and rituximab.19,20 Nevertheless, there is a lack of comprehensive characterization of the potential risk factors associated with PJP in children with SLE. Therefore, a retrospective analysis was conducted to elucidate the risk variables associated with PJP in pediatric patients diagnosed with SLE.
MATERIALS AND METHODS Patients and Clinical DataA study was conducted at the 900th Hospital of the Joint Logistic Support Force to investigate the risk factors for PJP in children with SLE exposed to prolonged high-dose glucocorticoids. Medical records of pediatric inpatients and outpatients treated from January 1, 2011, to December 31, 2020, were selected by searching the hospital's database using the appropriate International Classification of Diseases, Tenth Revision codes for SLE (M32.901).
The criteria for inclusion in the study were as follows: (1) individuals who were younger than 18 years at the time of inclusion; (2) a diagnosis of SLE based on the criteria established by the American College of Rheumatology in 199721; and (3) participants who had received a minimum daily dosage of 20 mg of prednisone or an equivalent dose of corticosteroid for at least 4 weeks throughout the enrollment period. The exclusion criteria encompassed the following: (1) individuals with a follow-up duration of less than 1 year; (2) subjects lacking complete clinical records; (3) participants who had previously taken medications for PJP prophylaxis; and (4) individuals with a history of PJP, AIDS, current malignancy, or a solid organ transplant. Subsequently, all treatment instances were categorized into 2 groups, namely, PJP and non-PJP, based on the presence or absence of PJP in the individual.
The study designated the commencement of high-dose steroid administration as the baseline date. For each treatment episode, the observation period was extended to 1 year from this baseline, as previous studies have indicated that most PJP cases tend to occur within this timeframe.6,9,13 However, if a PJP case or a censoring event such as death or loss of follow-up occurred, the observation period would be terminated. In addition, if the dosage of prednisone was reduced to less than 20 mg/d after more than 1 year from the initial baseline date and was subsequently increased again to 20 mg/d, it was considered a separate treatment episode.
Detection of PJPThe identification of potential PJP cases was accomplished by studying medical data. The instances that were identified were categorized as either suspected or confirmed PJP. The criteria for diagnosing a suspected case of PJP include the following22: (1) individual at high risk; (2) exhibits clinical symptoms such as difficulty breathing or coughing, fever (which may occasionally be absent), insufficient oxygen levels (which may not yet be evident), and chest pain (resulting from pneumothorax); (3) present radiographic evidence consistent with PJP includes bilateral mesenchymal infiltration around the portal vein and apical root23; and (4) with or without elevated serum lactate dehydrogenase levels. The criteria for confirming a diagnosis of PJP include the following: (1) pathogenic tests, such as sputum or bronchoalveolar lavage fluid or lung tissue biopsy, positive for Pneumocystis4,24; (2) symptoms and imaging findings consistent with PJP. The cases of PJP that were identified underwent adjudication by 2 doctors.
Statistical AnalysisThe statistical analysis was conducted using SPSS 26.0 software (IBM Corp., Armonk, NY). The descriptive statistics were presented using various measures, including the mean with SD, the median with first and third quartiles, and the number with percentage. A comparative analysis of variables between 2 groups was conducted using the Student t test for continuous variables and a χ2 test for categorical data. The significance level was deemed statistically significant at a p value of less than 0.05. In our investigation, univariate analysis was conducted to identify statistically significant differences (p < 0.05) between the group with PJP and the group without PJP. Furthermore, the risk variables for PJP were also derived from prior investigations conducted in adult patients with SLE. Subsequently, a multivariate Cox regression analysis was conducted utilizing the input technique to evaluate the relationships between covariates and the risk of PJP, as shown by hazard ratios (HRs) accompanied by a 95% confidence interval (CI). The predictive value of risk variables for PJP was evaluated using the areas under the curve (AUCs) of the receiver operating characteristic curve. The therapy sessions were subsequently categorized into several groups based on risk factors. Following the process of grouping, the statistical analysis involved the Kaplan-Meier method to compare the occurrence of PJP across several groups categorized by distinct risk variables.
RESULTS Study PopulationA total of 103 treatment episodes initially met the criteria, but 32 episodes were excluded from the study because of various reasons. These reasons included 9 episodes with less than 1 year of follow-up, 3 episodes lacking clinical information, and 20 episodes treated with PJP prophylaxis medication. Ultimately, the study included 71 treatment episodes involving 64 patients. Among these treatment episodes, 14 belonged to the PJP group, and 57 cases in the non-PJP group. During the observation period of 92.9 person-years, the incidence of PJP was 15.1 (95% CI, 14.3–15.9) per 100 person-years.
Clinical CharacteristicsA comparison was conducted between the characteristics of the PJP and non-PJP groups, as indicated in Table 1. Children in the PJP group exhibited a higher mean age compared with the non-PJP group, with values of 12.6 ± 0.5 years and 10.9 ± 0.3 years, respectively. This difference in age was found to be statistically significant (p = 0.024). The frequency of repeated high-dose steroid therapy was significantly higher in the PJP group than in the non-PJP group (50.0% vs. 19.3%; p = 0.018). The level of creatinine at the baseline was significantly elevated in the PJP group than in the non-PJP group, with values of 131.5 (79.6, 197.3) μmol/L and 57.2 (44.0, 91.0) μmol/L, respectively (p = 0.001). The PJP group exhibited a notably lower initial lymphocyte count at the baseline compared with the non-PJP group (1.0 [0.2, 1.8] vs. 1.5 [0.8, 2.1] × 109/L; p = 0.045). The lowest lymphocyte count throughout the observation period exhibited a statistical disparity (0.4 [0.2, 0.6] vs. 0.9 [0.6, 1.3] × 109/L; p < 0.001). During 1 year following the baseline date, the PJP group had a significantly higher frequency of CYC administration compared with the non-PJP group (64.3% vs. 35.1%; p = 0.046). There was no statistically significant difference in gender distribution observed between the PJP group and the non-PJP group. The disease activity of children at the baseline in both groups was comparable, as assessed by the modified SLEDAI score. No significant difference was observed between the 2 groups regarding white blood cells and hemoglobin, thrombocyte, or albumin levels. The administration of glucocorticoids and the use of immunosuppressants were more prevalent in the PJP group; however, no statistically significant differences were observed between the 2 groups.
TABLE 1 - Demographics and Clinical Characteristics of SLE Children With the PJP and Non-PJP Characteristics Non-PJP Group (n = 57) PJP Group (n = 14) p value Female 41 (71.9) 10 (71.4) 1.000 Age, y 10.9 ± 0.3 12.6 ± 0.5 0.024* Repeated high-dose steroid therapya 11 (19.3) 7 (50.0) 0.018* SLEDAI (score) 16.0 (10.0, 20.0) 17.0 (16.0, 22.3) 0.078 Baseline laboratory datab White blood cell, ×109/L 6.3 (4.5, 9.0) 7.1 (4.8, 10.5) 0.506 Initial lymphocyte count, ×109/L 1.5 (0.8, 2.1) 1.0 (0.2, 1.8) 0.045* Hemoglobin, g/L 104.2 ± 2.8 95.5 ± 5.6 0.170 Thrombocyte, ×109/L 176.0 (117.0, 274.0) 145.5 (73.5, 273.0) 0.418 Albumin, g/L 27.3 ± 1.2 23.2 ± 1.6 0.117 Creatinine, μmol/L 57.2 (44.0, 91.0) 131.5 (79.6, 197.3) 0.001** Lowest lymphocyte count,c ×109/L 0.9 (0.6, 1.3) 0.4 (0.2, 0.6) <0.001** Hydroxychloroquine 7 (12.3) 3 (21.4) 0.651 Glucocorticoid Initial dose, mg/d 60.0 (50.0, 60.0) 60.0 (60.0, 60.0) 0.084 Steroid ≥45 mg/d for ≥3 mo 39 (68.4) 13 (92.9) 0.130 Steroid ≥20 mg/d for ≥6 mo 46 (80.7) 14 (100.0) 0.078 Steroid-pulse treatment 34 (59.6) 10 (71.4) 0.613 Concomitant immunosuppressant 45 (78.9) 13 (92.9) 0.412 CYC pulse treatment 20 (35.1) 9 (64.3) 0.046* Cumulative CYC dose,d mg/kg 0.0 (0.0, 131.2) 36.8 (0.0, 77.3) 0.228 MMF 40 (70.2) 7 (50.0) 0.153 CYC + MMF 15 (26.3) 3 (21.4) 0.973 TAC 1 (1.8) 2 (14.3) 0.178 CyA 4 (7.0) 1 (7.1) 1.000Data are presented as mean ± SD, median (first and third quartiles), or number (percentage).
*p < 0.05; **p < 0.01.
a Repeated high-dose steroid therapy was defined as whether the prednisone dose in these children was ever tapered to <20 mg/d for ≥12 consecutive weeks and later increased to ≥20 mg/d again.
b The baseline date was defined as the day on which high-dose steroids (≥20 mg/d prednisone or equivalent) were started.
c The lowest lymphocyte count was collected within 1 year from the baseline date.
d The cumulative CYC dose was collected within 1 year from the baseline date.
CyA, cyclosporine A; MMF, mycophenolate mofetil; TAC, tacrolimus.
In the PJP group, 14 children experienced 2 confirmed and 12 suspected episodes (Table 2). The median time to PJP occurrence was 4.1 months, with an interquartile range of 2.3 to 5.0 months, and 85.7% of cases occurred within the first 6 months. At the time of PJP diagnosis, the median dose of corticosteroids was 60 (60, 60) mg, and 13 children (92.9%) received a daily prednisone dose of ≥45 mg, with a duration of ≥3 months. Similarly, 92.9% of children used other immunosuppressants, with 69.2% (9/13) specifically undergoing CYC treatment.
TABLE 2 - Characteristics of the 14 PJP Cases in SLE Children Patient Sex Age, y Renal Histopathology b Symptoms at Diagnosis of PJP Creatinine at the Baseline, μmol/L Lowest Lymphocyte Count,a ×109/L LDH at the Time of PJP Diagnosis, U/L Steroid Dose at the Time of PJP Diagnosis, mg/d Concomitant Immunosuppressive Treatment PJP Diagnosis Interval Between the Baseline and PJP, mo 1 F 13 IV (A/C) Dyspnea, cough, fever, hypoxemia, chest pain 85.0 0.07 — 60 CYC + MMF Confirmed 4.0 2 F 9 IV-G (A) Cough, hypoxemia 101.0 0.25 1691 60 CYC Suspected 4.4 3 M 13 IV-G (A) Cough, hypoxemia 197.0 0.41 847 60 MMF Suspected 1.7 4 M 11 IV-G (A) Dyspnea, fever, hypoxemia 81.8 0.58 1164 60 MMF + TAC Suspected 5.1 5 F 11 IV-G (A) Dyspnea, cough, hypoxemia 62.2 0.17 761 60 CYC Suspected 3.1 6 M 13 IV (A/C) Cough, fever, hypoxemia 167.0 0.37 844 60 CYC Confirmed 2.7 7 F 12 V + III (A) Cough, fever, dyspnea, hypoxemia 165.0 0.15 2511 60 CYC Suspected 4.1 8 F 16 V Cough, fever, dyspnea, hypoxemia 34.1 0.56 780 40 MMF + TAC Suspected 0.5 9 F 13 IV-G (A/C) Cough, dyspnea, hypoxemia 198.0 0.35 1050 60 CYC Suspected 6.7 10 F 12 IV-G (A/C) Cough, fever, hypoxemia 123.0 0.58 752 60 CYC Suspected 4.9 11 F 13 II + III (A) Cough, dyspnea, hypoxemia 288.0 0.58 661 60 MMF Suspected 4.8 12 F 13 IV-G (A/C) Cough, fever, dyspnea, hypoxemia 140.0 0.38 973 60 CYC Suspected 2.6 13 F 13 No Cough, fever 573.0 0.26 — 60 No Suspected 1.3 14 M 15 IV-G (A/C) Cough, dyspnea, hypoxemia 73.0 0.05 1426 60 CYC + MMF + AZA Suspected 12.0a The lowest lymphocyte count was collected within 1 year from the baseline date.
b Renal histopathology in SLE children was based on the International Society of Nephrology/Renal Pathology Society (ISN/RPS) 2003 classification of lupus nephritis.
AZA, azathioprine; F, female; LDH, lactate dehydrogenase; M, male; MMF, mycophenolate mofetil; TAC, tacrolimus.
In 20 excluded episodes with PJP prophylaxis, the level of creatinine at the baseline was 85.1 (55.5, 100.1) μmol/L, and the lowest lymphocyte count throughout the observation period was 0.5 (0.3, 0.7) × 109/L. The dose of prednisone at the time of PJP diagnosis was 60 (60, 60) mg, and all cases had taken at least a kind of immunosuppressant; however, no prophylactic case involved PJP (Supplementary Table S1, https://links.lww.com/RHU/A660).
Risk Factors for PJPTo further explore the risk factors associated with PJP occurrence, the 6 covariates with statistically significant differences were obtained from the aforementioned univariate analysis (including age, repeated high-dose steroid therapy, creatinine, initial lymphocyte count, the lowest lymphocyte count, and utilization of CYC). In addition, gender and prior studies recognized as relevant to risk factors for PJP occurrence (including elevated SLEDAI scores and the use of high-dose steroids)9,13,14 were analyzed as independent variables in a multivariate regression. The results indicated that creatinine (HR, 1.009; 95% CI, 1.001–1.017; p = 0.021) and the lowest lymphocyte count (HR, 0.007; 95% CI, 0.000–0.373; p = 0.014) may be independent risk factors for PJP occurrence (Table 3).
TABLE 3 - Risk Factors for PJP in Children With SLE Exposed to Prolonged High-Dose Glucocorticoids Variates Multivariable Analysis Adjusted HR (95% CI) p value AUC (95% CI) Optimal Cutoff Value Sensitivity, % Specificity, % Female 0.901 (0.210–3.853) 0.888 — — — — Age (y) 1.247 (0.810–1.920) 0.315 — — — — Repeated high-dose steroid therapya 1.466 (0.283–7.598) 0.648 — — — — SLEDAI (score) 1.000 (0.881–1.134) 0.998 — — — — Creatinine, μmol/L 1.009 (1.001–1.017) 0.021* 0.786 (0.647–0.925) 72.5 μmol/L 85.7 63.2 Initial lymphocyte count (×109/L) 0.929 (0.812–1.063) 0.283 — — — — Lowest lymphocyte countb (×109/L) 0.007 (0.000–0.373) 0.014* 0.883 (0.802–0.964) 0.6 × 109/L 100.0 87.2 Initial dose of steroid (mg/d) 0.929 (0.812–1.063) 0.283 — — — — CYC 0.802 (0.135–4.775) 0.809 — — — — Creatinine combined with the lowest*p < 0.05.
a Repeated high-dose steroid therapy was defined as whether the prednisone dose in these children was ever tapered to <20 mg/d for ≥12 consecutive weeks and later increased to ≥20 mg/d again.
b The lowest lymphocyte count was collected within 1 year from the baseline date.
Receiver operating characteristic curves were constructed to assess the predictive value of independent risk factors for developing PJP. The receiver operating characteristic curves demonstrated that the AUC values for predicting the risk of PJP with creatinine, the lowest lymphocyte count, and the combination of creatinine and the lowest lymphocyte count were 0.786 (95% CI, 0.647–0.925; p = 0.001), 0.883 (95% CI, 0.802–0.964; p < 0.001), and 0.934 (95% CI, 0.870–0.997; p < 0.001), respectively. This indicates that the combined prediction of the 2 factors has a higher value in predicting the occurrence of PJP. In addition, when the creatinine level was greater than 72.5 μmol/L and the lowest lymphocyte count was less than 0.6 × 109/L, the sensitivity and specificity for predicting PJP were 78.6% and 96.5%, respectively (Table 3).
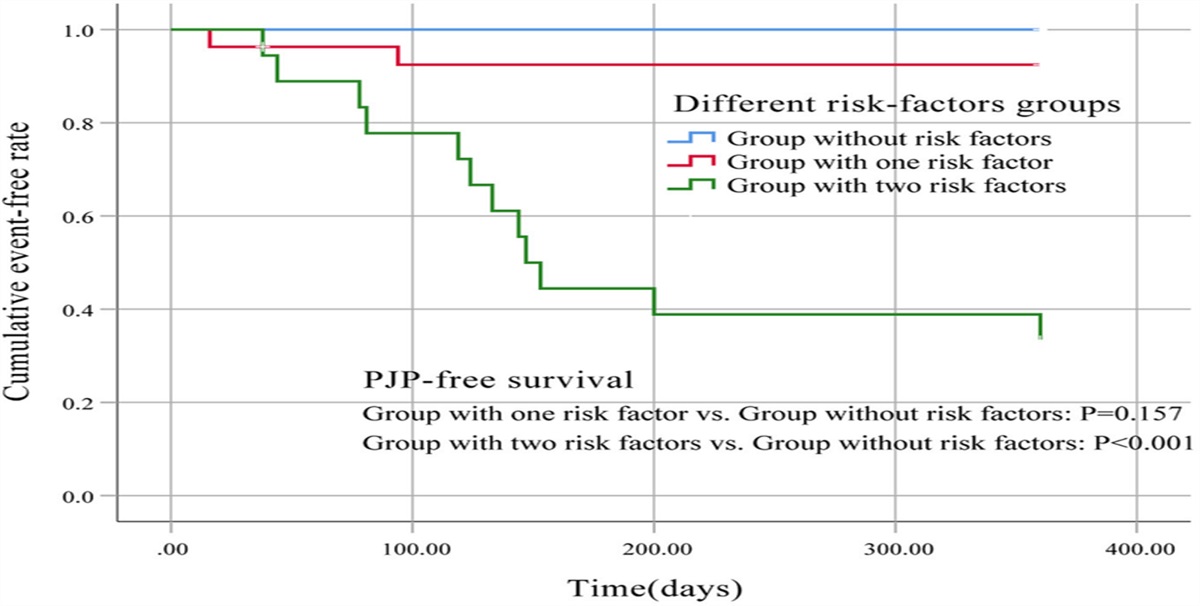
Incidence of PJP in Different Risk-Factors GroupsTo further validate the predictive value of creatinine and the lowest lymphocyte count for the occurrence of PJP in high-risk pediatric patients, we categorized 71 treatment episodes into 3 groups based on the presence or absence of creatinine levels greater than 72.5 μmol/L and the lowest lymphocyte count less than 0.6 × 109/L. These groups include the following: the group with 2 risk factors (n = 18), the group with 1 risk factor (n = 27), and the group without risk factors (n = 26). Kaplan-Meier survival curves indicated that the incidence of PJP in the group with 2 risk factors was significantly higher than in the group without risk factors, with statistical significance (p < 0.001). There was no statistically significant difference between the group without risk factors and the group with 1 risk factor (p = 0.157) (Figure). This result further emphasizes that the combination of creatinine and the lowest lymphocyte count can better predict the occurrence of PJP.
 FIGURE:
FIGURE: Kaplan-Meier curve showing PJP-free survival in different risk-factors groups. The risk factors were creatinine >72.5 μmol/L and the lowest lymphocyte count <0.6 × 109/L.
DISCUSSIONPneumocystis jirovecii pneumonia is a life-threatening infection that often requires ventilator support and has a high fatality rate, particularly in individuals with impaired immune systems. Children with SLE have an increased susceptibility to PJP because of weakened immune function, progressive organic damage, and the use of immunosuppressive medications. The correlation between higher death rates and PJP highlights the necessity of recommending PJP prophylaxis for children at high risk. However, there is still a lack of clarity regarding the risk factors associated with PJP in children diagnosed with SLE. To the best of our knowledge, this is the first study to investigate risk factors for PJP in children with SLE receiving prolonged high-dose steroids.
One of the independent risk variables for PJP in children diagnosed with SLE was an elevated level of creatinine. An increased creatinine level often indicates renal involvement. Previous research has indicated that individuals with SLE who experience renal involvement are more susceptible to developing PJP.9,10,18 This association may be attributed to the fact that SLE patients with renal involvement tend to receive more aggressive immunosuppressive treatment compared with those without renal issues. Furthermore, it should be noted that these individuals exhibit a diminished capacity to eliminate immunosuppressive medications by renal excretion. The substantial pharmaceutical load imposes a prolonged state of immunosuppression on the body, rendering individuals susceptible to the development of PJP. In contrast to adult patients diagnosed with SLE, children with SLE exhibit a higher likelihood of experiencing renal involvement.7,8 Nevertheless, there is a lack of research investigating the potential relationship between the extent of renal involvement and the occurrence of PJP in pediatric patients diagnosed with SLE. In this study, we observed that a creatinine level exceeding 72.5 μmol/L was a significant threshold for PJP in children with SLE. This finding provided valuable guidance for determining the need for PJP prophylaxis in SLE children with renal dysfunction.
Our investigation results indicated that a decrease in lymphocyte count was identified as an independent risk factor for PJP. In addition, we determined that a lymphocyte count below 0.6 × 109/L served as a critical threshold for determining the necessity of PJP prophylaxis in children diagnosed with SLE who are undergoing long-term treatment with high-dose steroids. The finding above aligns with the outcomes of prior investigations conducted on adult SLE patients. Lertnawapan et al.9 suggested that a significant reduction in lymphocyte count to a level of less than 0.75 × 109/L during SLE therapy indicated the need for prophylaxis against PJP. The occurrence of PJP in patients with connective tissue disease was found to be associated with a lymphocyte count of less than 0.5 × 109/L within 2 weeks of starting prednisone treatment at a dosage of 30 mg or more per day, as reported in a previous study.16 The reduction in lymphocyte count impacted the elimination of Pneumocystis, resulting in the development of PJP as a consequence. The clearance of Pneumocystis by lymphocytes mainly occurs through 2 primary mechanisms. T lymphocytes, often known as T cells, are a type of white blood cell that plays a crucial role in the adaptive immune response. According to a study by Roths et al.,25 mice exhibiting severe combined immunodeficiency displayed a shortage in functional lymphocytes and subsequently developed spontaneous Pneumocystis infection. Nevertheless, it was shown that the reintroduction of CD4+ T lymphocytes into mice resulted in a restoration of their capacity to eliminate the infection efficiently.26,27 This finding indicates that CD4+ T lymphocytes play a crucial role in the clearance of Pneumocystis. CD4+ T lymphocytes are vital in eradicating infections by recruiting and activating various immune effector cells, such as monocytes and macrophages.4 In addition, CD8+ T lymphocytes contribute to the clearance of Pneumocystis through the regulation of proinflammatory proteins and chemokines.28 B lymphocytes, often known as B cells, are a type of white blood cell that plays a crucial role in the adaptive immune response. B lymphocytes were found to generate Pneumocystis-specific immunoglobulins M and G antibodies, with the latter playing a crucial role in facilitating the phagocytosis of Pneumocystis by alveolar macrophages.29 In addition to their role in antibody production, B lymphocytes were observed to influence the clearance of Pneumocystis through their involvement in the proliferation and activation of T lymphocytes.30
Given that both a high level of creatinine and a low number of lymphocytes were risk factors for PJP, we compared these 2 risk factors to assess their suitability in predicting PJP. The AUC for the combination of creatinine and the lowest lymphocyte count in predicting the risk of PJP was determined to be 0.934 (95% CI, 0.870–0.997; p < 0.001). These findings indicate that the combination of creatinine and the lowest lymphocyte count is a highly effective predictor of PJP, exhibiting a sensitivity of 78.6% and a specificity of 96.5%. Furthermore, there was a notable increase in the occurrence of PJP among children with 2 risk factors (p < 0.001). Hence, it may be inferred that children diagnosed with SLE who exhibit creatinine levels greater than 72.5 μmol/L in the initial phase of the disease are more susceptible to PJP when their lymphocyte count falls below 0.6 × 109/L during treatment. It is advisable for these individuals to consider using TMP/SMX as a preventive measure against PJP.
Studies have established a connection between the therapeutic dosage and duration of glucocorticoids and the occurrence of PJP. In addition, it has been found that extended periods of high-dose steroid usage are associated with an increased risk of PJP.9,12 Nevertheless, the relationship between the cumulative dose of glucocorticoids and the incidence of PJP remained uncertain. This study aimed to examine the population of children diagnosed with SLE who were administered a minimum daily dosage of prednisone equal to or exceeding 20 mg for at least 4 weeks. No statistically significant differences were observed between the PJP and non-PJP groups in terms of the use of prednisone at a dosage of 45 mg or higher per day for 3 months or longer, as well as the use of prednisone at a dosage of 20 mg or higher per day for 6 months or longer. The
留言 (0)