Based on earlier reports,9 we expected that measurements of pupillary unrest would be able to detect changes in pain after surgery. Nevertheless, our findings in patients experiencing substantial pain relief by regional anesthesia showed that our measure of pupillary unrest (PUAL) did not change with changes in pain intensity in a postsurgical patient population.
The first published investigation on the interplay of pupillary unrest and pain reported that painful contractions during labour and delivery increased pupillary unrest.9 Following epidural analgesia, with improved pain control, the contractions failed to increase pupillary unrest. A subsequent study by the same investigators reported that in recovery room patients following surgery, pupillary unrest correlated with reported pain scores, suggesting that the extent of pupillary unrest may indeed be a measure of pain.14
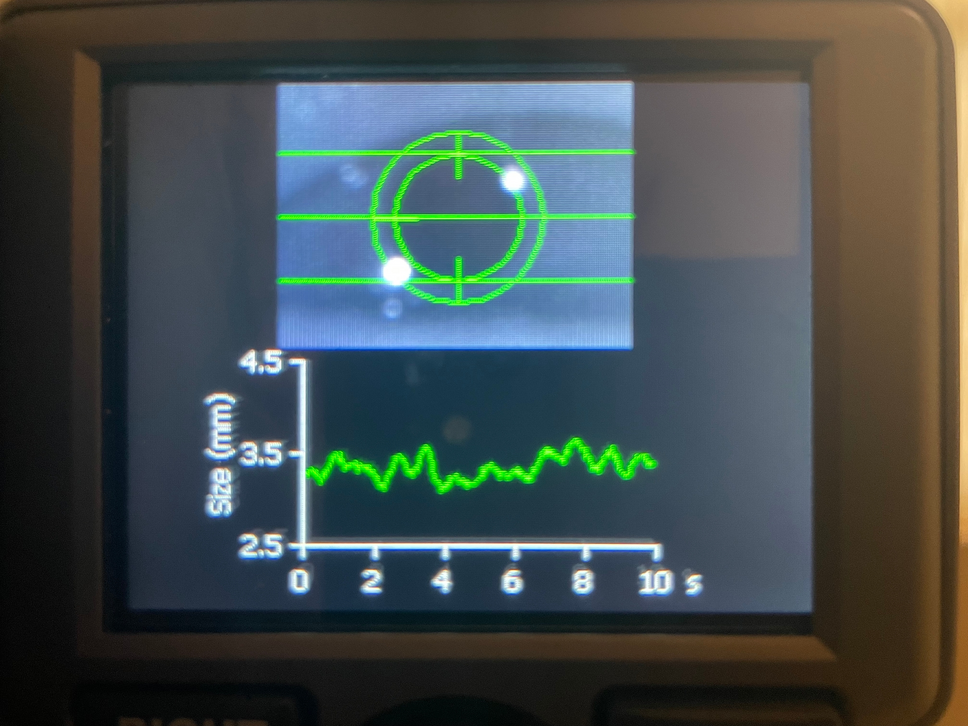
Pupillary unrest is a potential marker of pain as it is affected by opposing inhibitory and excitatory influences on the Edinger–Westphal (EW) nucleus. Sympathetic stimulation caused by pain could alter this balance and increase pupillary unrest by inhibition of the EW nucleus. Nevertheless, arousal caused by nonpainful stimuli has also shown to increase pupillary unrest.15 Opioids are known to block the inhibitory input to the EW nucleus, thus causing pupillary constriction and suppression of pupillary unrest.8,16 In this study, we tried to confirm that measurement of PUAL can still detect changes in pain intensity in a patient population that is likely to have been exposed to opioids.
Our finding that in a postsurgical, predominantly opioid-exposed patient population, PUAL was not able to detect changes in pain raises the question whether factors other than pain could explain the correlations previously observed between pupillary unrest and pain, or which factors could have masked the impact of pain on pupillary unrest in our patient population. There are several possible explanations for the findings of the present study and why they appear to contradict findings from earlier studies.
Pupil diameter and pupillary unrest reflect the activity of the locus coeruleus,17 the noradrenergic nucleus that controls arousal.18 It is possible that the observed increases in pupillary unrest were not caused by pain itself, but rather by the arousal triggered by pain, the associated stress response, or the emotional response caused by the painful experience. Such responses would not be expected to last long because they cannot be maintained for an extended period.19,20 Our findings are compatible with the hypothesis that pain is not able to sustain arousal and that the observed increases in pupillary unrest are short-lived, even if pain persists. Therefore, the subsequent relief from pain does not alter PUAL.
An alternative explanation for our findings is that pupillary unrest does change with pain, but that the pain-evoked effects on pupillary unrest were masked in our patients by opioids and other centrally acting agents. The effects of opioids on the EW nucleus could have masked the stimulatory effects of pain on pupillary unrest. Nevertheless, the observation that pupillary unrest at baseline was not severely depressed in our study population and that even dramatic changes in pain intensity did not alter pupillary unrest in these patients make it unlikely that the administration of opioids is solely responsible for the inability of pupillary unrest to accurately reflect increased pain. Furthermore, even in patients who had received smaller doses of opioids, the analgesic interventions failed to effect PUAL. If even small doses of administered opioids would be able to mask the association between pain and pupillary unrest, measurement of PUAL would have very little utility as a measure of pain in most clinical scenarios involving patients with substantial pain.
A recently published study supports and complements the findings of our study. In patients admitted to an emergency room with pain, no correlation was observed between patient-reported NRS and PUAL. Measurements of PUAL also failed to identify patients with moderate to high pain scores, even though opioid use prior to admission was an exclusion criterion for the study. Our finding that reducing pain is not associated with changes in PUAL in patients who have been experiencing sustained pain expands on these findings.
The present investigation used a simple methodology and has limitations. We were not able to quantify whether or to which extent PUAL was suppressed at baseline by the administered opioids as we were not able to measure opioid plasma concentrations. As already discussed, pain-evoked changes in pupillary unrest may become masked once a certain amount of opioids has been administered or pupillary unrest is depressed below a certain threshold. Nevertheless, the baseline values of PUAL in our study were comparable to those observed in opioid-naïve patients in their respective age group.21
Some patients received additional analgesics such as intravenous ketamine and lidocaine, whose effects on pupillary unrest are not well investigated. Nevertheless, excluding those patients who received these drugs in a subgroup analysis revealed identical findings. We decided to not exclude these patients, as their use reflects the clinical scenarios any tool designed to assess pain would be operated in.
This observational study was not preregistered on ClinicalTrials.gov at study start, which may raise concerns about bias, thus potentially limiting the impact of the findings. The results are also not supported by a sample size estimate at the time of study start because preliminary data were lacking. To address this limitation, we conducted a post hoc power analysis to show that our final sample size—while small—would have been large enough to detect relevant changes in pupillary oscillations with analgesia had they occurred.
It should also be noted that we are contrasting our findings to the earlier findings of Charier et al. who used a different algorithm to quantify pupillary oscillations,9 which has been termed the “variation coefficient of pupillary diameter.” Although both approaches are based on different algorithms, they both attempt to quantify pupillary unrest and the findings of investigations using these measurements should be comparable.
In summary, measurements of pupillary unrest did not identify changes in postsurgical pain in predominantly opioid-exposed patients when regional anesthesia was used to manage pain. Pupillary unrest has not been shown to be a reliable marker for pain in clinical settings of sustained pain. While pupillary unrest seems to be a useful indicator for the extent of central opioid effects, it does not appear, in clinical scenarios associated with pain, to be a promising tool to objectively measure pain.


留言 (0)