
記住我


The study was approved by the Institutional Review Board of SMG-SNU Boramae Medical Center, Seoul, Republic of Korea (approval no. 10-2022-55; date of approval, 4 July 2022) and registered at ClinicalTrials.gov before patient enrolment (NCT05377346; principal investigator, Jin-Young Hwang; date of registration, 17 May 2022). The study protocol complied with the ethical guidelines of the Declaration of Helsinki. We obtained written informed consent from the study participants. This report conformed to the applicable Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Study design and patient selectionThis study involved patients aged > 18 yr who were scheduled for surgery under general anesthesia with a supraglottic airway from September 2022 to April 2023. The exclusion criteria were risk factors for pulmonary aspiration (e.g., achalasia or pregnancy), known or predicted difficult airway, anatomic variation or pathology of the upper airway, requirement for postoperative ventilator care, and surgeries requiring positions other than supine. We recorded the following patient characteristics: age, sex, weight, height, body mass index, American Society of Anesthesiologists Physical Status, and airway characteristics (Mallampati score, thyromental distance, sternomental distance, and neck circumference).
RandomizationWe randomly allocated the enrolled patients to one of two groups: those who underwent application of cricoid pressure (cricoid group) and those who underwent application of paratracheal pressure (paratracheal group) during and after i-gel insertion. For randomization, we generated a web-based random sequence with block sizes of 4 and 12 (Research Randomizer, Social Psychology Network, Wesleyan University, Middletown, CT, USA; available from URL: https://randomizer.org; accessed January 2024). We sealed the sequence in an opaque envelope, which was kept by an anesthesiologist who was not involved in the study.
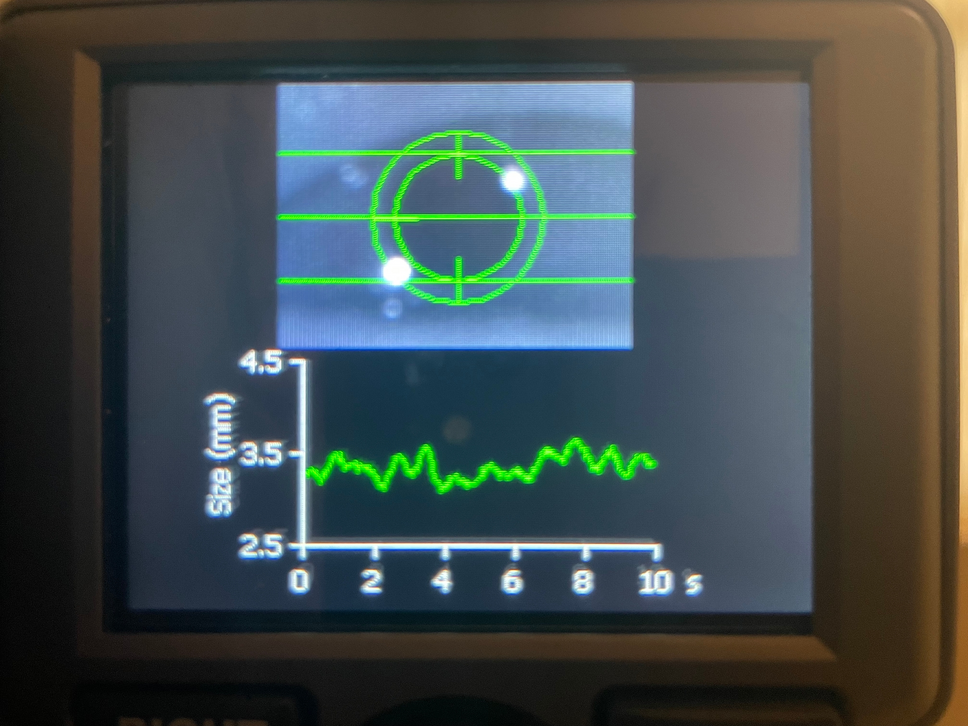
Anesthesia procedureThe patients entered the operating room without premedication. Routine monitoring included electrocardiography, pulse oximetry, and noninvasive blood pressure monitoring. After preoxygenation, anesthesia was induced with lidocaine (30 mg), propofol (1–2 mg·kg−1), fentanyl (1–2 μg·kg−1), and rocuronium (0.6 mg·kg−1). After neuromuscular blockade, we covered the patient’s neck with an opaque drape so that the anesthesiologists who performed the i-gel insertion were blinded to the group allocation. We selected the size of the i-gel according to the manufacturer’s recommendation: size 3 for patients with a body weight of < 50 kg, size 4 for those with a body weight of 50–90 kg, and size 5 for those with a body weight of > 90 kg. In the cricoid group, cricoid pressure was applied with a force of 30 N, equivalent to approximately 3.06 kg (9.8 N = 1 kg), using a three-finger maneuver. While applying cricoid pressure, the patient’s head was maintained in the sniffing position and was supported with the other hand of the clinician performing the maneuver to prevent head flexion (bimanual maneuver).14 In the paratracheal group, paratracheal pressure was applied with a force of 30 N against the vertebral body with a 3–12-MHz linear ultrasound transducer (Vscan with Dual Probe; GE HealthCare, Chicago, IL, USA) while observing the esophageal obstruction, and the clinician performing the maneuver also supported the patient’s neck (Fig. 1). Ultrasound was prepared in both groups for blinding. Two anesthesiologists with experience performing more than 300 i-gel insertions performed the i-gel insertion. After inserting the i-gel, the anesthesiologist attempted positive-pressure ventilation with gentle manual bagging under each maneuver. If an adequate tidal volume could not be achieved, the anesthesiologist repositioned the i-gel, and ventilation was re-evaluated. We defined successful insertion as the presence of a square expiratory carbon dioxide curve on capnography and an adequate tidal volume in the absence of a pharyngeal leakage sound with a peak airway pressure of ≥ 12 cm H2O during gentle manual ventilation.15 We allowed two attempts, and each attempt proceeded for 60 sec. If the i-gel could not be inserted within 60 sec, the anesthesiologist ventilated the patient with a facial mask and attempted i-gel insertion again. If the second attempt was unsuccessful, we recorded the case as a failure and the i-gel was inserted without the allocated maneuver. We defined the time required for insertion as the duration of time from picking up the i-gel to detecting the square waveform on capnography, and it was calculated by adding the time taken for each attempt. In successful cases, the allocated maneuvers were maintained, and we recorded the tidal volume and peak inspiratory pressure while the mechanical ventilation was set in volume-control mode with a tidal volume of 8 mL·kg−1 of ideal body weight, respiratory rate of 12 breaths·min−1, and zero end-expiratory pressure. Subsequently, the tidal volume and peak inspiratory pressure without the allocated maneuver were recorded using the same ventilator settings. The resistance felt by the anesthesiologist while inserting the i-gel was evaluated on a 4-grade scale (1, no resistance; 2, moderate resistance; 3, severe resistance; and 4, impossible to insert the i-gel). Finally, we assessed the accuracy of the insertion location by the anatomical alignment of the i-gel in the larynx using a fibreoptic bronchoscope with an outer diameter of 4.1 mm (Olympus LE-P, Olympus Optical Co., Tokyo, Japan) positioned at the end of the tube section of the i-gel. The accuracy was recorded on a five-grade scale (1, only glottis observed; 2, posterior surface of epiglottis and glottis observed; 3, anterior part or tip of epiglottis and > 50% of glottis observed; 4, down-folded epiglottis and < 50% of glottis observed; and 5, glottis completely obscured by down-folded epiglottis).16
Fig. 1
Diagram of cricoid pressure and paratracheal pressure
The primary outcome was the overall success rate of i-gel insertion. The secondary outcomes were the time required for insertion, the accuracy of the insertion location evaluated with a fibreoptic bronchoscope, resistance during insertion, and the tidal volume and peak inspiratory pressure with or without each maneuver after i-gel insertion.
Statistical analysisAll statistical analyses were performed with IBM SPSS Statistics for Windows version 26.0 (IBM Corp., Armonk, NY, USA). We tested continuous variables for normality with graphical methods such as histograms and Q–Q plots, as well as the Kolmogorov–Smirnov test. Values are expressed as mean (standard deviation), median [interquartile range (IQR)], or number (percentage). Point and interval estimates were determined for between-group differences. We tested continuous data with Student’s t test or the Mann–Whitney U test, and categorical data with the Chi square or Fisher’s exact test. In all analyses, P < 0.05 was considered statistically significant.
The sample size calculation was based on a pilot study of 30 patients in our centre. The insertion success rate was 0.93 while applying paratracheal pressure and 0.67 while applying cricoid pressure. With a type I error of 0.05, a power of 0.8, and a dropout rate of 10%, we included 76 patients (38 patients in each group).
留言 (0)