
記住我



The patient is a 23-year-old male with DMD who had been managed on chronic oral steroids since age 3. Of note, he lived remote from any major medical center, and owing to logistic difficulties, was only able to attend clinic periodically. Due to significant progressive weakness, he had been managed at home with sip ventilator during the day and bi-level ventilation at night. His most recent forced vital capacity from 7 years prior was 0.9 L (22% predicted). At presentation, he was on carvedilol 9.375 mg twice daily, lisinopril 2.5 mg daily, and spironolactone 25 mg daily. He had previously tolerated doses as high as carvedilol 12.5 mg twice daily and lisinopril 10 mg daily, but those doses had been sequentially decreased due to symptomatic hypotension since an admission for pneumonia 5 years prior to his current presentation.
On presentation to clinic, he complained of acute on chronic (> 3 years) fatigue and lower extremity pitting edema. Over the prior 6 months he described progressive cough and orthopnea. He also noted swelling and intermittent orthopnea since the previously noted admission for pneumonia.
His clinical exam was remarkable for a pulse of 84 beats/min, blood pressure 124/86 mmHg, oxygen saturations of 97% in room air, a weight of 103.9 kg and a BMI of 41 kg/m2. Jugular venous distention and hepatomegaly could not be assessed due to his body habitus/body position. Mild pitting edema was noted to the calf bilaterally, as well as non-pitting edema of the arms to the level of the bicep. There was no peripheral hyperpigmentation or ulceration noted.
His nt-BNP was 150 pg/mL, similar to the year prior (128 pg/mL) and slightly elevated from a measurement 5 years prior (109 pg/mL). Additional laboratory evaluation including hepatic and renal function were unchanged. Cystatin C GFR was stable over the previous 5 years (85–92 mL/min/1.73 m2) and the total bilirubin was normal. His cardiac MRI demonstrated a LVEF of 39% and RVEF of 51% in the absence of ventricular dilation (left ventricular end diastolic volume 68 mL/m2, right ventricular end diastolic volume 55 mL/m2). These findings were stable when compared with serial cardiac MRIs over the previous 3 years.
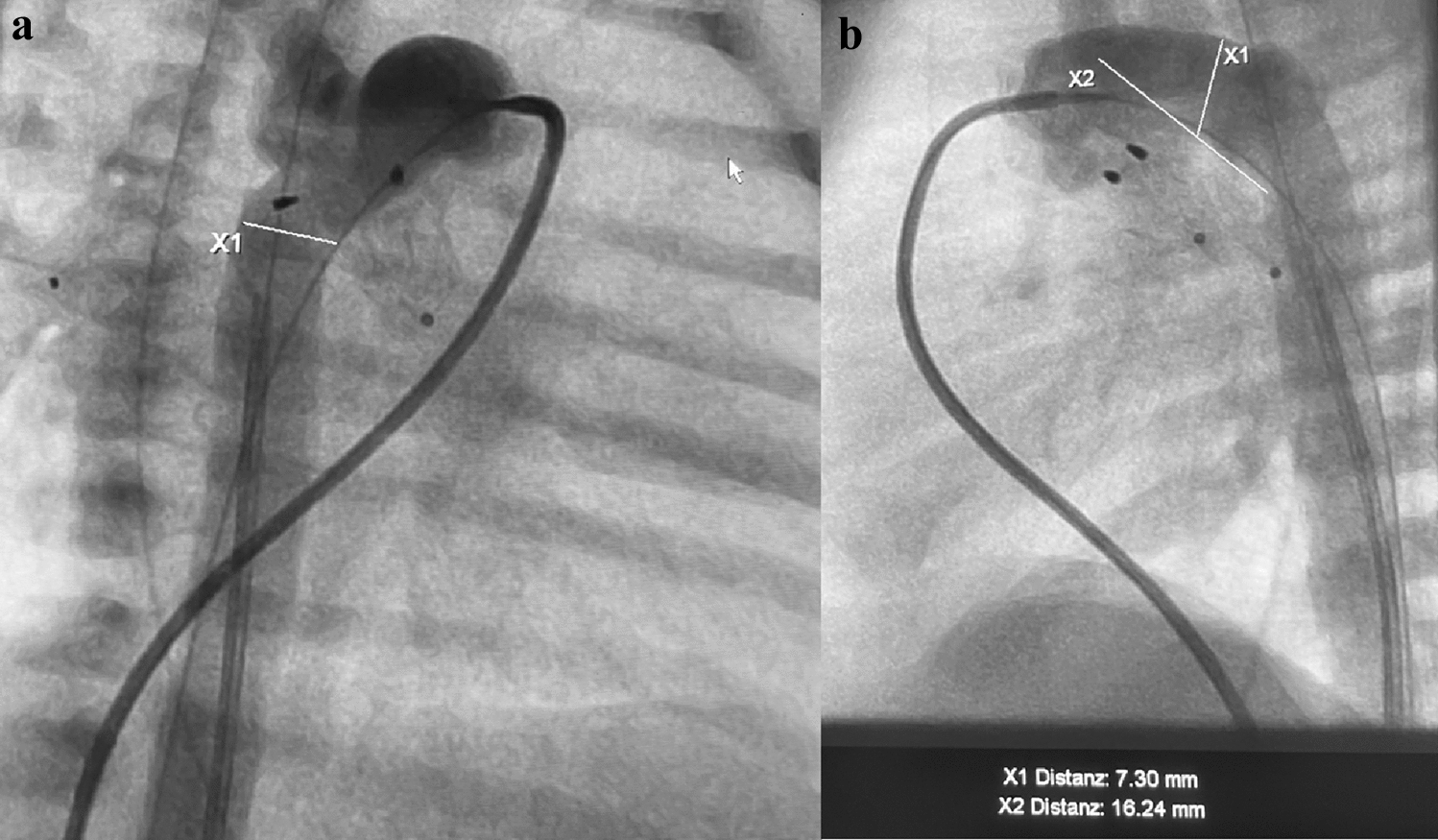
He was initially managed with changes in salt and fluid intake as well as clinically driven diuretic management. However, due to persistence of symptoms and the challenges in differentiating heart failure and respiratory/swallow symptoms, the patient underwent right heart catheterization under minimal sedation. Hemodynamics revealed a low thermodilution cardiac index of 2.34 L/min/m2, and elevated right and left ventricular filling pressures [mean right atrial pressure 15 mmHg, mean pulmonary artery wedge pressure 27 mmHg, and a normal pulmonary vascular resistance (2.5 Wu m2)]. During the cardiac catheterization, and after a pulmonary angiogram demonstrated an appropriately sized left lower pulmonary artery (greater than 7 mm in diameter), a wireless pulmonary artery pressure device (CardioMEMS, Abbott Laboratories, Atlanta, GA) was implanted and calibrated successfully (Fig. 1).
Fig. 1
Wireless pulmonary artery pressure device (white arrow) in situ after completion of the procedure
The patient had an uneventful recovery from the catheterization and was discharged home on increased diuretic therapy. During the 24 months of follow-up, the patient has been able to transmit pulmonary artery recordings at regular intervals (ultimately spaced out to every 2–4 weeks once he was stable). Briefly, changes in this patient’s symptoms, such as worsening cough or dyspnea were compared to pulmonary artery pressure recordings, and in cases of increased pressure and symptomatic worsening, diuretic dosing was increased. Titrations such as these were managed remotely without requiring patient travel. The symptoms of cough and dyspnea have now completely resolved, and he has not required any further admissions.
留言 (0)