
記住我








Alzheimer’s disease (AD) is a neurodegenerative disease characterized by cognitive impairment, along with mental and behavioral abnormalities, and a decline in the ability to perform daily activities. It is the most common type of dementia and imposes a significant burden on the healthcare industry due to its high morbidity, disability, and mortality rates (Kaur et al., 2019; XXX, 2023). In 2015, approximately 47 million people worldwide suffered from dementia. It is estimated that the number of AD patients worldwide will reach 75 million by 2030, and this number is expected to increase to 131 million by 2050 (Watermeyer and Calia, 2019). Currently, the pathogenesis of AD is not well understood, and there are no definitive treatment options. However, the main recognized pathological features include neuroinflammatory plaques containing amyloid-β (Aβ), neural fibrillary tangles (NFTs) formed by aberrantly phosphorylated aggregates of tau proteins, and neuroinflammation (Braak et al., 2006; Silva et al., 2019; van der Kant et al., 2020; Leng and Edison, 2021). Carboplatin, donepezil, galantamine, etc. are conventional pharmacologic treatments for AD, and their mechanism of action is to inhibit acetylcholinesterase, which increases acetylcholine (Ach) levels in the brain (Birks and Harvey, 2018; Marucci et al., 2021; Pardo-Moreno et al., 2022). As a non-competitive N-methyl-D-aspartate (NMDA) receptor antagonist, memantine has been approved by the FDA for the treatment of AD, which can block the abnormal elevation of glutamate to damage neurons and reduce apoptosis of neuronal memory cells, and is mainly used in patients with moderate to severe AD (Wang and Reddy, 2017). Although these drugs provide some relief, they do not prevent disease-related neuropathological changes. Consequently, an increasing number of scientists and clinicians have begun to explore non-pharmacological treatments.
Transcranial magnetic stimulation (TMS) is a magnetic field stimulation technology that utilizes pulsed magnetic fields to act on the central nervous system (Barker et al., 1985). This process changes the membrane potential of cortical nerve cells, resulting in the generation of induced currents. These currents then affect brain metabolism and neural electrical activity, leading to a series of physiological and biochemical reactions (Kim et al., 2019; Begemann et al., 2020; Jannati et al., 2023). Repetitive TMS (rTMS), a mode of TMS, involves applying repeated magnetic signals to the cortex. By generating the sum of excitatory postsynaptic potentials, it extends the stimulation period and regulates the activity of brain areas associated with cognitive functions, thereby improving cognitive knowledge (Nguyen et al., 2018; Bao et al., 2021). Different stimulation sites of rTMS target various cognitive areas. Currently, rTMS is the most commonly used method, capable of altering cortical inhibition and excitation based on the stimulation frequency. Notably, rTMS has significant effects on cognitive enhancement. Varying frequencies of rTMS produce different regulatory effects on the cortex (Lefaucheur et al., 2020). High-frequency rTMS (>1 Hz) typically exhibits an excitatory effect, while low-frequency rTMS (≤1 Hz) often displays an inhibitory effect. Furthermore, the excitatory or inhibitory effects of rTMS may be reversed as the duration of the stimulation train changes (O’Reardon et al., 2007). The efficacy of rTMS is dependent on precise targeting to ensure the appropriate brain regions are being treated. It is essential for the physician to manually hold the stimulation coil or use a fixed bracket to secure it in place. Due to the inability to accurately sense the fit and angle of each stimulation coil on the scalp, subsequent treatments cannot be reliably replicated from previous sessions, leading to challenges in addressing target shift during treatment.
Systematic reviews (SRs)/Meta-analyses (MAs) are important tools for guiding evidence-based clinical practice and have been widely used in various medical disciplines in recent years. With the development of evidence-based medicine, more and more SRs/MAs have been conducted to investigate the effectiveness and safety of rTMS for AD. Overview of SRs/MAs is a widely used method for assessing the quality of evidence in evidence-based medicine. It involves collecting information on SRs/MAs that pertain to the same disease or health problem, providing a comprehensive approach to reassessing their quality. While SRs/MAs have always been considered a crucial source of reliable information, there are various factors in the evaluation process that can diminish their quality. These include incomplete literature sources, insufficient evaluation methods, and publication bias. By integrating the evidence from multiple SRs/MAs, an overview of SRs/MAs offers a more comprehensive and informative approach, thereby providing higher-quality evidence for clinical practice.
This overview utilized several assessment tools including the A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR-2), Risk of Bias in Systematic Reviews (ROBIS), Preferred Reporting Item for Systematic Review and Meta analysis (PRISMA), and the Grading of Recommendations, Assessments, Developments, and Evaluations (GRADE) (Schünemann et al., 2008; Whiting et al., 2016; Shea et al., 2017; Page et al., 2021). The aim of this overview was to thoroughly evaluate the methodological quality, reporting quality, risk of bias, and evidence quality of systematic reviews and meta-analyses (SRs/MAs) on the use of rTMS in the treatment of AD. The objective was to provide a critical assessment of the quality of relevant SRs/MAs and to objectively and comprehensively evaluate the effectiveness and safety of rTMS for AD.
2 Methods 2.1 Inclusion and exclusion criteriaWe included SRs/MAs based on RCTs of rTMS treatment for patients with AD, regardless of study countries, limited to Chinese and English. The patients met the diagnostic criteria of AD and were not limited by gender, age, race and course of disease. The intervention group was treated with rTMS without limitation of frequency, treatment site, and other treatment parameters, or rTMS in combination with other treatments, including cognitive training, acupuncture, rehabilitation therapy, and conventional medication for AD. The control group was treated with conventional medication for AD, cognitive training, rehabilitation therapy, sham stimulation, or with a blank control, which should be consistent with the treatment group at baseline. At least one of these results had to be reported in SRs/MAs: Alzheimer’s disease assessment cognitive scale (ADAS-cog), Mini-Mental State Examination (MMSE), mood, or behavior.
We excluded SRs/MAs if it met any of the following criteria: (a) duplicate published literature; (b) literature comparisons were made between two rTMS methods; (c) literature for which data could not be extracted or full text was not available; (d) other types of research, such as protocols, network meta-analyses, conference papers, and case reports.
2.2 Search strategyWe conducted a comprehensive search of SRs/MAs for rTMS treatment of AD from seven databases, including Embase, Web of Science, Cochrane Library, PubMed, China National Knowledge Infrastructure (CNKI), VIP, Sino-Med, and Wanfang databases published from the beginning to January 23, 2024. Search terms included: “Alzheimer’s disease,” “repetitive transcranial magnetic stimulation,” “transcranial magnetic stimulation,” “meta-analysis,” “systematic review.” We use Boolean logic to formulate search formulas that work across all databases. Detailed search strategy is provided in the Supplementary material.
2.3 Study selection and data extractionAccording to the comprehensive search strategy, the SRs/MAs obtained from the search was imported into Endnote to remove duplicate articles. Two reviewers removed irrelevant articles and selected articles of interest by reading titles and abstracts. Two reviewers made the final decision based on the inclusion criteria by reading the full text. In case of disagreement, a third reviewer was consulted. Data were extracted from the included literature, and information extracted included: authors, country, age of patients, type of study, number of documents, sample size, treatment group, control group, methodological evaluation tools, outcome indicators, and main conclusions.
2.4 Assessment methods 2.4.1 Methodological quality assessmentTwo reviewers utilized the AMSTAR-2 tool to assess the methodological quality of the included systematic reviews. The AMSTAR-2 comprises a total of 16 items, each categorized as “Yes,” “No,” or “Partially Yes.” Items 2, 4, 7, 9, 11, 13, and 15 are considered critical (Shea et al., 2017). If there are no items defects or only one non-critical items defect, the method is deemed of high quality, resulting in an accurate and comprehensive SRs/MAs conclusion. If there are multiple non-critical items defects but no critical items defect, the method quality is considered moderate, and the SRs/MAs conclusion remains accurate. If there is a critical entry defect, regardless of the presence or absence of non-critical entry defects, the method quality is classified as low, and the SRs/MAs conclusion is also low. If there are multiple critical items defects, with or without non-critical items defects, the method quality is critical low.
2.4.2 Report quality assessmentThe reporting quality of the included SRs/MAs was evaluated by two independent reviewers using the PRISMA 2020 checklist (Page et al., 2021). The PRISMA statement consists of 27 items in seven fields, each of which is scored according to the degree of conformity with the literature. If the criterion is met, it is rated as “Yes,” if it is partially met, it is rated as “Partially Yes,” if it is not mentioned, it is rated as “No.”
2.4.3 Risk of biasThe risk of bias of the included SR/MAs was assessed using the Risk of Bias in Systematic Reviews (ROBIS) tool (Whiting et al., 2016). The ROBIS tool assessment consisted of three phases, assessing the relevance, the extent of risk of bias (ROB) in the SRs/MAs process, and judging ROB. The second phase systematically assessed four key areas, including (a) study eligibility criteria, (b) identification and selection of studies, (c) data collection and study evaluation, and (d) synthesis and conclusions. The assessments were categorized as “high risk,” “low risk” or “unknown risk.”
2.4.4 Evidence quality assessmentTwo reviewers independently used the Recommended Assessment, Development, and Evaluation (GRADE) tool to assess the quality of evidence (Schünemann et al., 2008). It includes five aspects: the limitations of the study, the inconsistency of the results, the indirectness of the evidence, the imprecision and the bias of the report. We divide the quality of evidence into four levels: “High,” “Moderate,” “Low”, and “Very low.”
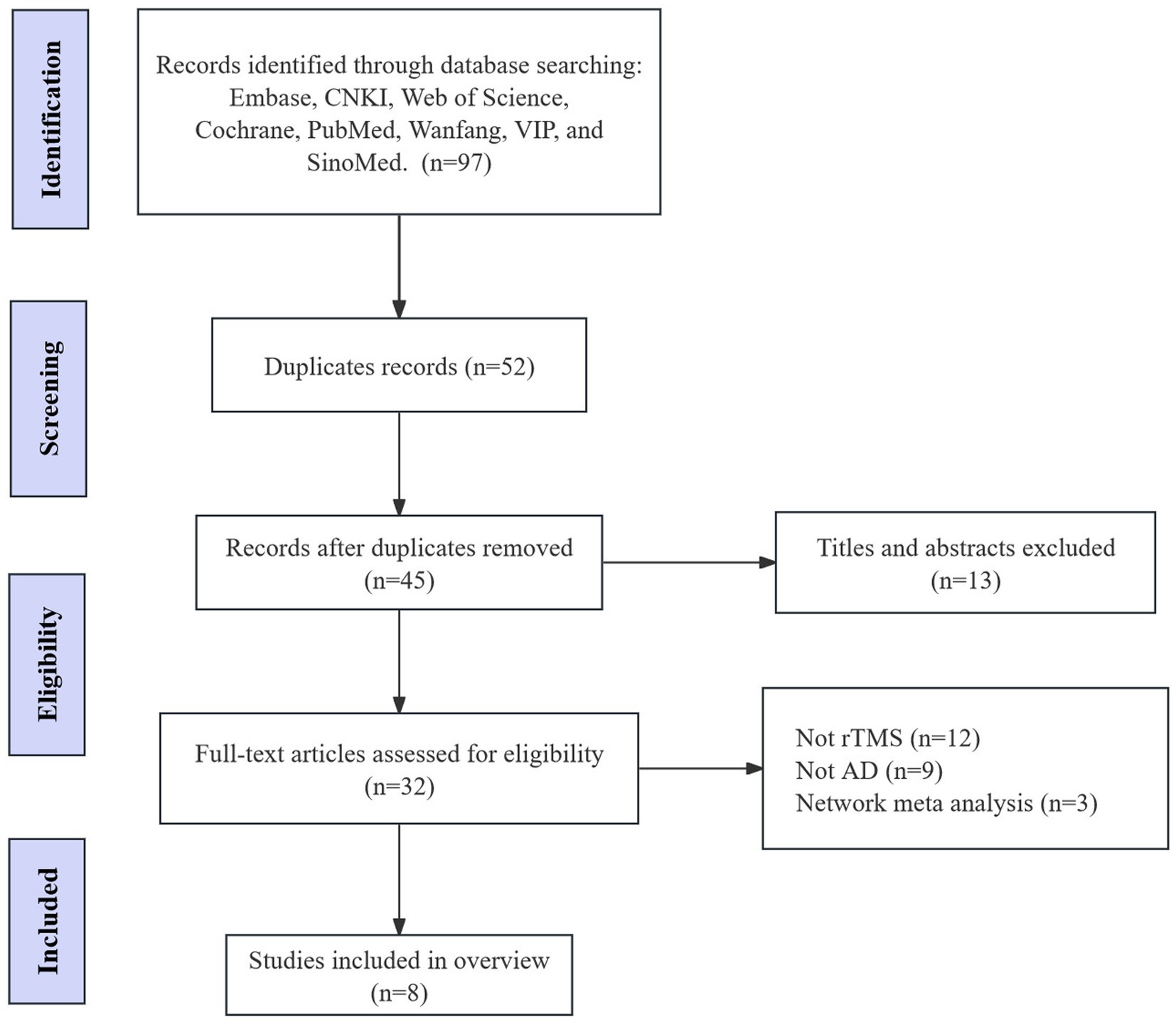
3 Results 3.1 Search resultsAccording to the search strategy, we retrieved 97 records. Among these studies, we excluded 52 duplicate papers. Thirteen papers were excluded by reading titles and abstracts. 32 articles were considered potentially eligible and the full texts of the papers were downloaded. After independent review by two authors, 24 SRs/MAs were excluded and 8 SRs/MAs were included for final analysis (Figure 1) (Liao et al., 2015; Cheng and Wu, 2016; Liang et al., 2017; Dong et al., 2018; Lin et al., 2019; Wang et al., 2020; Zhang et al., 2022; Xiu et al., 2024).
Figure 1. Flow chart of the literature search and study selection process.
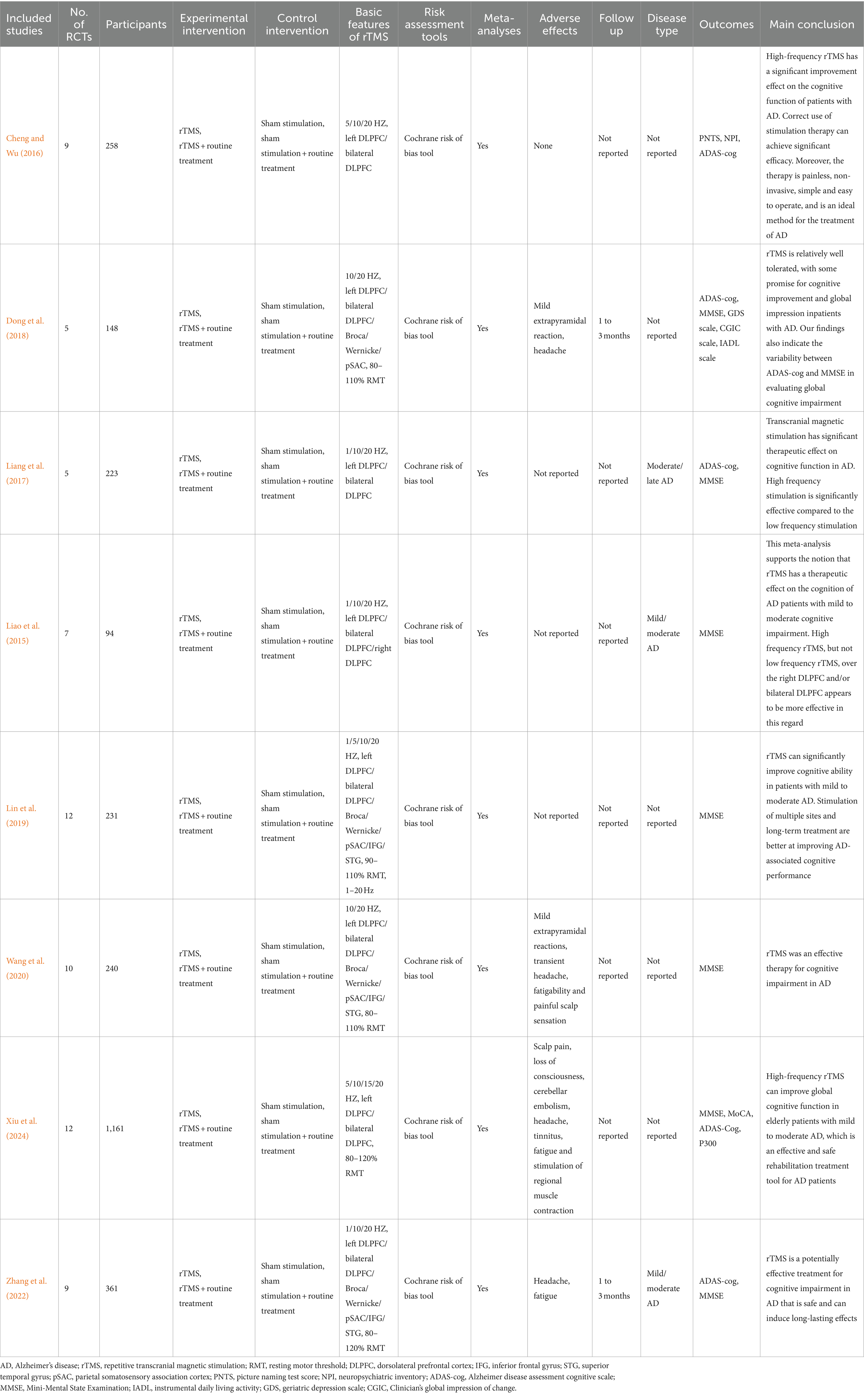
3.2 Characteristics of the included SRs/MAsThe basic characteristics of the included SRs/MAs are shown in Table 1. A total of 8 SRs/MAs were included, published in studies from 2015 to 2024. Six of the SRs/MAs were published in English, and the rest were published in Chinese. The number of original studies included in each SRs/MAs ranged from 5 to 12, with a maximum sample size of 1,161 participants and a minimum sample size of 94 participants. All SRs/MAs were assessed for risk using the Cochrane risk of bias tool. Interventions in the control group were mainly conventional medication, sham stimulation, conventional therapy or combination therapy to improve cognition. The experimental group had a variety of interventions, including unilateral high-frequency rTMS treatment, unilateral low-frequency rTMS treatment, bilateral low-frequency rTMS treatment, and rTMS combined with conventional treatment. Single-site stimulation included the right and left dorsolateral prefrontal cortex (DLPFC), PC, motor cortex, inferior frontal gyrus (IFG), and superior temporal gyrus (STG), and multi-site stimulation included two or more of these sites. Outcome measures included the Picture Naming Test Score (PNTS), Neuropsychiatric Inventory (NPI), Alzheimer’s Disease Cognitive Assessment Scale (ADAS-cog), Brief Mental State Examination (MMSE), Instrumental Activities of Daily Living (IADL), Geriatric Depression Scale (GDS), and Clinician’s General Impression of Change (CGIC). Only 2 of the 8 SRs/MAs reported the duration of follow-up after treatment, which ranged from 1 to 3 months. Only 3 SRs/MAs described disease staging.
Table 1. Characteristics of the included systematic reviews.
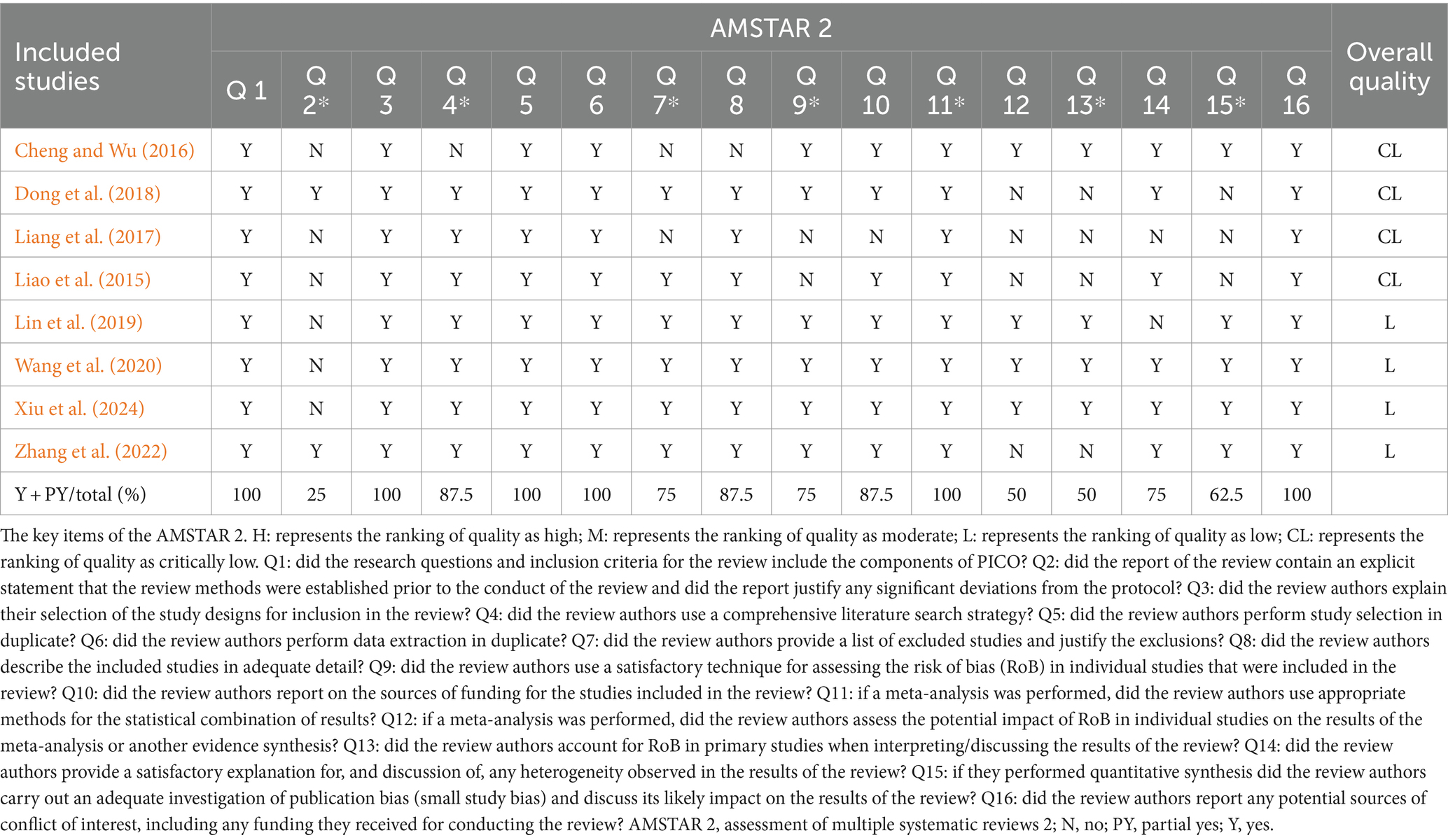
3.3 Methodological quality assessment of the included SRs/MAsWe utilized AMSTAR-2 to assess the methodological quality of the 8 included SRs/MAs. Out of the 8 research reports, 4 were classified as critically low quality, while the remaining 4 were rated as low quality. Only two SRs/MAs received a rating of “Yes” for key item 2, while the others were rated as “No” due to the absence of a review scheme (Dong et al., 2018; Zhang et al., 2022). Regarding key item 4, only one SR/MA did not present a comprehensive and detailed search strategy (Cheng and Wu, 2016). Additionally, two SRs/MAs did not provide a list of excluded studies, resulting in a “No” rating for key item 7 (Cheng and Wu, 2016; Liang et al., 2017). Similarly, two SRs/MAs did not fully evaluate the risk of bias in individual studies, leading to a “No” rating for key item 9 (Liao et al., 2015; Liang et al., 2017). Key items 13 and 15 exhibited flaws as well. Four SRs/MAs did not elucidate the risk of bias in individual studies, and four SRs/MAs did not thoroughly investigate publication bias. Considering one or more significant flaws in key items 2, 4, 7, 9, 11, 13, and 15, as well as multiple flaws in non-key items, all SRs/MAs are deemed to be of low or critically low quality. An overview of methodological quality of included SRs/MAs is presented in Table 2.
Table 2. Methodological quality of included SRs/MAs.
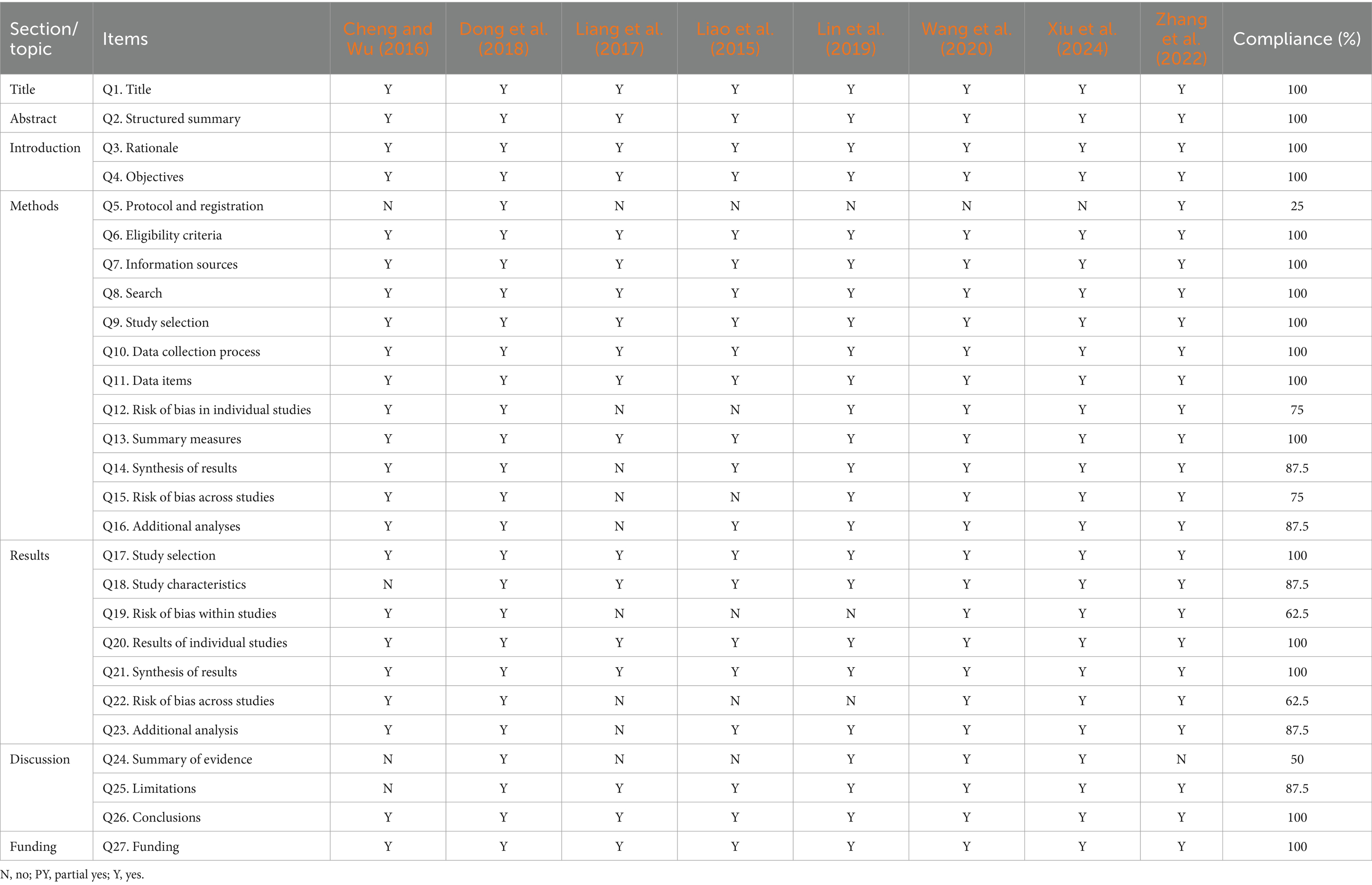
3.4 Reporting quality of the included SRs/MAsWe used PRISMA to assess the reporting quality of the eight included SRs/MAs (Table 3). Among the 27 items, 16 items were fully reported (100%), and 11 items had missing or insufficient reporting. In the methods section, only 2 studies reported protocol and registration, with a reporting rate of 25% (Dong et al., 2018; Zhang et al., 2022). Limitations were found in the risk of bias in individual studies (75%), synthesis of results (87.5%), risk of bias across studies (75%), and additional analyses (87.5%). In the “Results” section, only one SRs/MAs did not describe the characteristics of the study (87.5%) (Cheng and Wu, 2016), three SRs/MAs did not describe risk of bias within studies (62.5%) (Liao et al., 2015; Liang et al., 2017; Lin et al., 2019), three SRs/MAs did not describe the risk of bias across studies (62.5%) (Liao et al., 2015; Liang et al., 2017; Lin et al., 2019), and one did not report additional analyses (87.5%) (Liang et al., 2017). Half of the SRs/MAs reported summary of the evidence, and one SRs/MAs did not mention limitations (87.5%).
Table 3. Results of the PRISMA checklist for the included SRs/MAs.
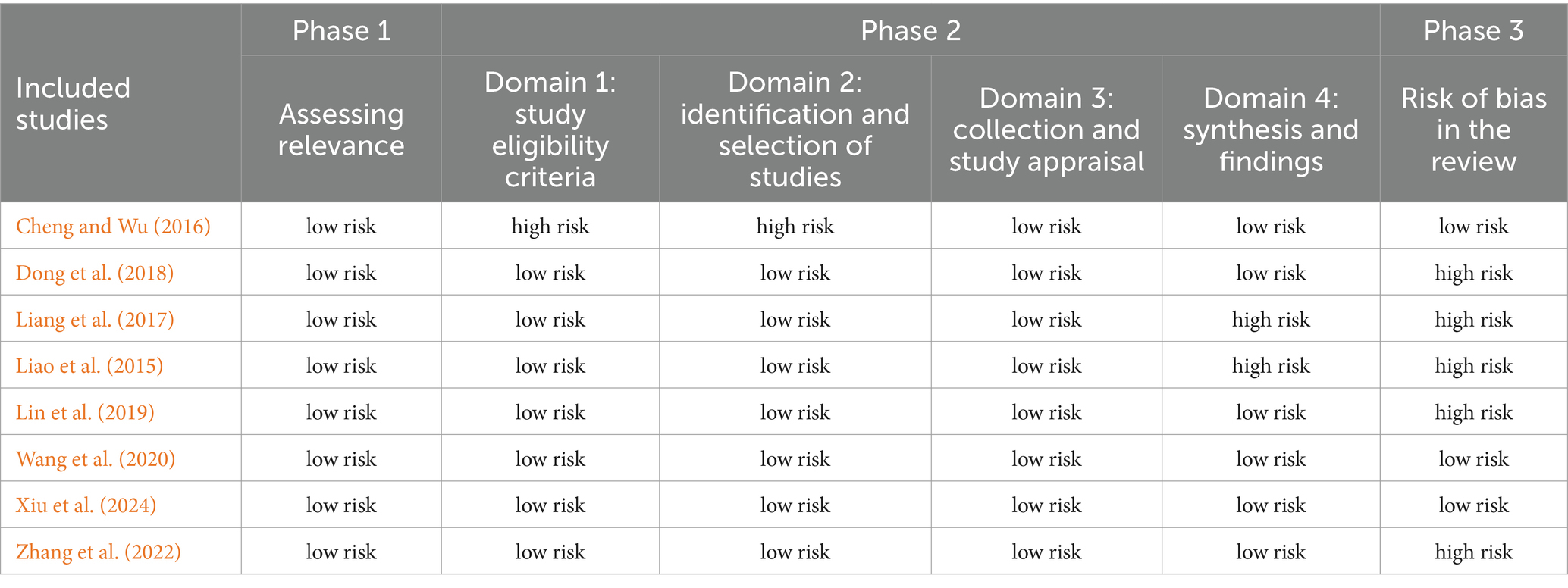
3.5 Risk of bias of the included SRs/MAsTable 4 presents the results of the risk of bias assessment of the included SRs/MAs using the ROBIS tool. The tool consists of three stages and four areas. In the first stage, all SRs/MAs were evaluated and found to have a low risk of bias, indicating their relevance to the study topic. Domain 1 focuses on assessing the eligibility criteria of the studies, and one SRs/MAs (12.5%) was rated as having a high risk of bias (Cheng and Wu, 2016). Domain 2 involves the assessment of study identification and selection, and seven SRs/MAs (87.5%) were rated as having a low risk of bias (Cheng and Wu, 2016). Domain 3 evaluates the collection and study appraisal, and all were rated as having a low risk of bias. Domain 4 assesses the attention given to the synthesis and findings, and six SRs/MAs (75%) were rated as having a low risk of bias (Cheng and Wu, 2016; Dong et al., 2018; Lin et al., 2019; Wang et al., 2020; Zhang et al., 2022; Xiu et al., 2024). In stage 3, when considering the overall risk of bias, five SRs/MAs were rated as high risk because they did not provide any explanation or supplement regarding the risk of bias, while the remaining SRs/MAs were considered to have a low risk.
Table 4. Risk of bias of the included SRs/MAs.
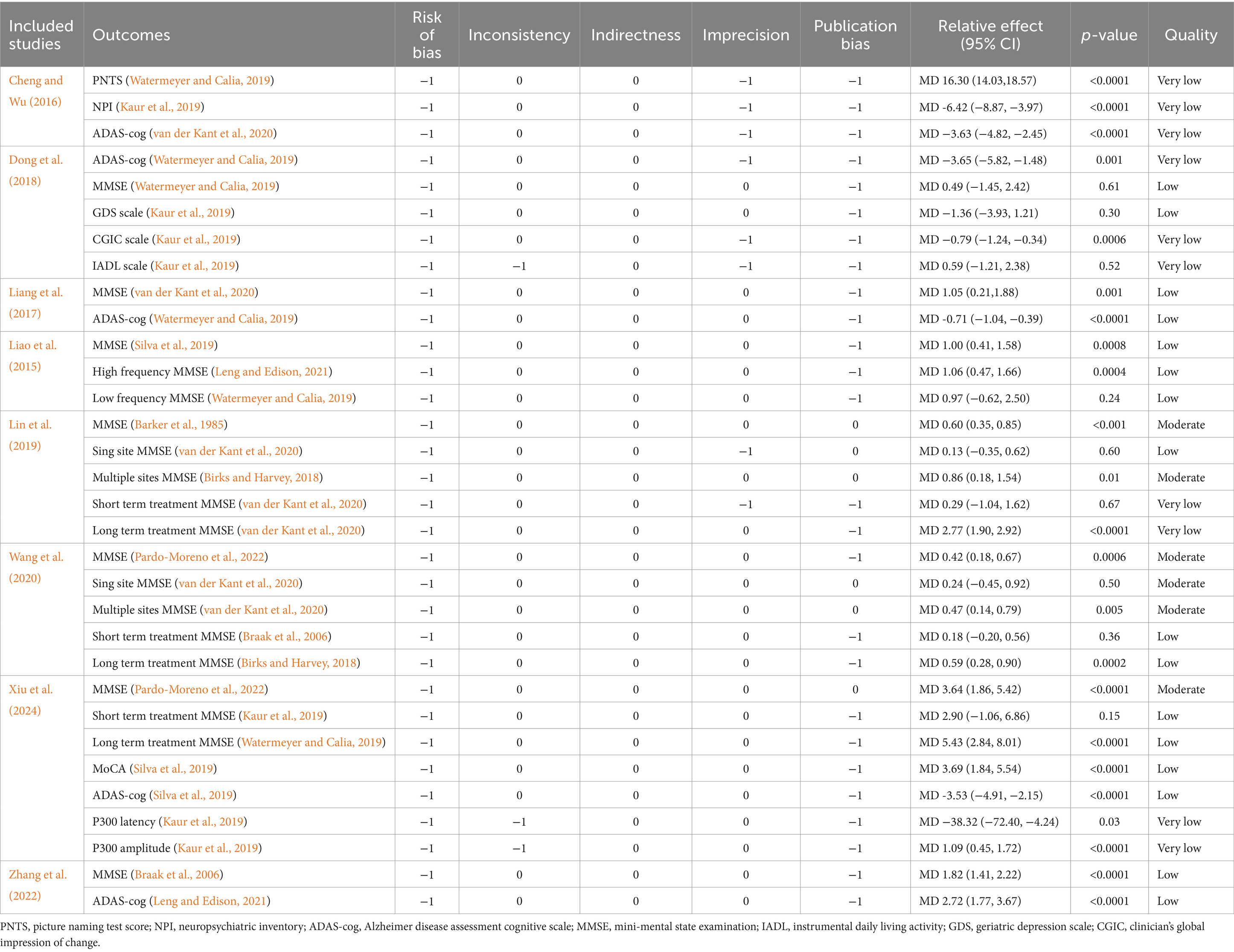
3.6 Evidence quality evaluation resultsWe evaluated the quality of evidence using the GRADE tool and found that 8 SRs/MAs provided evidence for 32 outcome indicators (Table 5). The results showed that there was no high-level evidence in the included outcomes, 6 were moderate evidence (18.75%), 16 were low evidence (50%), and 10 (31.25%) were very low evidence, and the quality of evidence was generally low. Overall, the quality of evidence was generally low. This could be attributed to several factors. Firstly, there might be publication bias as indicated by an asymmetric funnel plot or the presence of only positive results. Secondly, the included studies had a risk of bias due to issues such as lack of randomization, blinding, allocation concealment, incomplete outcome data, or selective reporting bias. Thirdly, the small sample size of the included studies and inconsistencies in interventions, data extraction, and outcome indicators could have affected the accuracy of the results. Lastly, there was significant heterogeneity among the studies.
Table 5. Results of evidence quality with GRADE.
3.7 Outcome measuresMost current SRs/MAs are mainly focused on the improvement of efficacy and safety of rTMS in AD patients in the following aspects: cognitive function, activities of daily living and adverse reactions.
3.7.1 Improvement of cognitive symptomsImpaired cognitive function is a common symptom of AD. These 8 SRs/MAs contained a total of 131 clinical trials. These studies selected MMSE, MoCA and ADAS-cog to assess cognitive function. Seven SRs/MAs investigated the MMSE scores of AD patients treated with rTMS (Liao et al., 2015; Liang et al., 2017; Dong et al., 2018; Lin et al., 2019; Wang et al., 2020; Zhang et al., 2022; Xiu et al., 2024). One of these 7 SRs/MAs showed that rTMS did not significantly improve the MMSE score of AD patients (MD = 0.59, 95% CI: −1.21 to 2.38, p = 0.52) (Dong et al., 2018), and the remaining SRs/MAs showed that rTMS could significantly improve the MMSE score of AD patients. Liao et al. further conducted a subgroup analysis based on the frequency of rTMS and found that high frequency rTMS could significantly improve the MMSE score (MD = 1.06, 95% CI: 0.47 to 1.66, p = 0.0004), while no significance was found for low-frequency rTMS (MD = 0.97, 95% CI: −0.62 to 2.50, p = 0.24) (Liao et al., 2015). Subgroup analysis of the two SRs/MAs based on stimulation site showed that multi-site stimulation improved cognition more significantly than single-site stimulation (Lin et al., 2019; Wang et al., 2020). Subgroup analysis of two SR/MA based on rTMS treatment courses showed that long-term rTMS treatment was more effective in improving cognition (Wang et al., 2020; Xiu et al., 2024).
Five SRs/MAs investigated the ADAS-cog of rTMS in the treatment of AD (Cheng and Wu, 2016; Liang et al., 2017; Dong et al., 2018; Zhang et al., 2022; Xiu et al., 2024). The pooled results of SRs/MAs showed that rTMS treatment of AD patients could significantly reduce ADAS-cog, which proved the improvement of cognitive function. Only one SRs/MAs evaluated cognition using MoCA, and this study showed that rTMS treatment of AD patients significantly improved MoCA (Xiu et al., 2024).
3.7.2 Adverse reactionsFour of the included SRs/MAs reported adverse reactions after rTMS treatment. Adverse reactions include mild extrapyramidal reaction, headache, fatigability, painful scalp sensation, loss of consciousness, cerebellar embolism, tinnitus (Dong et al., 2018; Wang et al., 2020; Zhang et al., 2022; Xiu et al., 2024).
4 Discussion 4.1 Summary of main findingsThis overview presents the first comprehensive descriptive analysis of SRs/MAs on the use of rTMS for AD. The analysis included 69 RCTs with a total of 2,676 participants. To assess the methodological quality, reporting quality, evidence quality, and risk of bias of the published SRs/MAs, we employed rigorous evaluation tools including AMSTAR 2, ROBIS, PRISMA, and GRADE. According to AMSTAR 2, four out of 8 SRs/MAs were rated as very low quality and 4 as low quality. Using the PRISMA checklist, we observed that out of the 27 items, 16 were fully reported while 11 were either missing or insufficiently reported. The application of the ROBIS tool indicated that 3 SRs/MAs had a low risk of bias. The GRADE results revealed that the included literature did not provide any high quality evidence. Moderate quality evidence was found in 6 outcomes (18.75%), while 16 outcomes (50%) provided low-level evidence, and 10 outcomes (31.25%) presented very low evidence. Overall, the quality of the evidence was generally low.
4.2 Mechanism of rTMS for Alzheimer’s diseaserTMS has been found to have an impact on the treatment of cognitive impairment, although its specific mechanism is still not fully understood. There are several possible mechanisms that have been suggested. rTMS can regulate the excitability of the cerebral cortex by altering the frequency of stimulation to specific regions of the brain (Chen et al., 2023). Different frequencies of rTMS have different effects. Low frequency stimulation (≤1 Hz) can inhibit the activity of local neurons and reduce cortical excitability, whereas high frequency stimulation (≥5 Hz) can excite the activity of local neurons and increase cortical excitability (Chen et al., 2023). High frequency stimulation can also influence the metabolism of brain functions by enhancing neural activity in the corresponding brain regions, leading to improvements in neurobiochemistry and related metabolites at the site of stimulation (Ahmed et al., 2012). This could explain why high frequency rTMS stimulation has shown better therapeutic effects in patients with AD. However, a recent controlled study demonstrated that 2 weeks of low-frequency (1 Hz) rTMS stimulation of the right DLPFC in AD patients improved recognition memory function compared to sham stimulation, and this improvement was sustained during a 1 month follow-up period (Turriziani et al., 2019). It is worth noting that rTMS stimulation has not yet been standardized in terms of frequency, and other therapeutic parameters such as high stimulation intensity may also enhance motor cortical excitability. In a meta analysis conducted by Liao et al., it was found that high-frequency rTMS (rather than low-frequency rTMS) applied to the right DLPFC and/or bilateral DLPFC appears to be more effective in improving cognition (Liao et al., 2015).
Studies have shown that patients with AD exhibit abnormal neural functional connections. rTMS has been found to regulate the synaptic plasticity and connectivity of neurons, promoting the remodeling of neurons and restoration of functional connections (Song et al., 2020). This process involves long-term potentiation (LTP) and long-term depression (LTD). High-frequency rTMS induces excitatory postsynaptic potential changes, resulting in the LTP effect. On the other hand, low-frequency rTMS induces inhibitory postsynaptic potential changes, leading to the LTD effect (Li et al., 2019). Neuroimaging-based studies have demonstrated that high-frequency rTMS increases local cortical blood perfusion and moderates cholinergic neuron damage resulting from localized blood perfusion, thereby slowing the progression of cognitive dysfunction. Dressle et al. used functional magnetic resonance imaging (fMRI) to confirm that suprathreshold rTMS increases cerebral perfusion in the cortex of the stimulation site (Dressler et al., 1990). Paus et al. used a continuous pulse sequence with a stimulation parameter of 10 s, high-frequency rTMS at a frequency of 10 Hz, and made positron emission tomography (PET) to measure the cerebral blood flow index, and found that the number of rTMS pulses was positively correlated with the cerebral blood flow index of the stimulation site (Aceves-Serrano et al., 2022). These mechanisms contribute to the therapeutic effects of rTMS in treating AD and improving cognitive function in patients. The most common adverse reactions of rTMS treatment are scalp pain during treatment and transient headache after stimulation, but usually the degree of pain is mild. The mechanism may be related to the action of variable pulse magnetic field on the scalp.
4.3 Results-based discussionSRs/MAs reported methodological quality of low (50%) or very low (50%) according to AMSTAR-2. It is worth noting that 25% (2/8) of the SRs/MAs provide previous protocols, while 75% (6/8) cannot guarantee whether SRs/MAs strictly followed the research plan during the production of the research report, thus increasing the risk of bias. Additionally, 25% (2/8) SRs/MAs did not list exclusions and reasons for exclusion, which may increase selection bias. 50% (4/8) SRs/MAs did not clarify the risk of bias of individual studies, 50% (4/8) SRs/MAs did not thoroughly investigate publication bias, and 62.5% (5/8) conducted a quantitative synthesis, which made the methodological quality of the reported studies was low.
According to PRISMA, of the 27 reporting items, 16 were fully reported (100%) and 11 were omitted or underreported. Underreporting was present in the entries for protocol and registration (25%), risk of bias in individual studies (75%), synthesis of results (87.5%), risk of bias across studies (75%), additional analyses (87.5%), summary of evidence (87.5%).
Based on the results of GRADE tool evidence quality grading, 18.75% (6/32) of the results were classified as moderate evidence, while 50% (16/32) were classified as low evidence. Additionally, 31.25% (8/32) of the results were categorized as very low evidence, indicating a generally low quality of evidence. Several factors contributed to decline in quality. Firstly, the design of most studies incorporates many factors that increase bias and heterogeneity, which is the main reason for the decline in the quality of the evidence. Common factors include blinding procedures, allocation concealment, and randomization techniques. There are few recent high-quality RCT trials on rTMS for the treatment of AD, which is directly attributed to the small number of included studies, small sample sizes, inconsistent treatment selection, data extraction, and outcome labeling. Heterogeneity may also be affected by the diversity of rTMS therapy parameters and its combination with other therapies (such as cognitive training, different drugs), as well as individual differences in patients, psychological health, disease extent, and disease course factors. Secondly, the quality of evidence was also affected by publication bias (26/32), inconsistency (3/32), and imprecision (8/32) in the SRs/MAs conducted. Publication bias may arise when a small number of clinical trials with positive results are selectively published, or when there is an asymmetric funnel plot indicating potential bias in the results. Inconsistency was observed through low overlap of confidence intervals between studies and high heterogeneity in the combined results (I2 > 50%), without a reasonable explanation provided by the investigators. These factors collectively contributed to the reduced quality of evidence.
4.4 Implications for further studyIn response to the aforementioned problems, future researchers should strive to address these limitations when conducting systematic reviews on the use of rTMS in the treatment of AD. For instance, reviewers should consider registering or publishing the protocol in advance to minimize the risk of bias and ensure the rigor of the SRs/MAs process. In terms of literature search and selection, gray literature should be taken into account, and a comprehensive list of excluded literature with explanations should be provided to ensure transparency and avoid publication bias. In cases of significant heterogeneity during data analysis, subgroup analysis should be performed. When assessing the risk of bias, it is essential to thoroughly analyze the reasons behind the bias and discuss the potential impact of publication bias. Additionally, the review should mention the funding sources, as commercially funded studies may introduce bias in favor of the funder. Researchers should adhere to the relevant guidelines such as AMSTAR-2, PRISMA, and ROBIS assessments to minimize bias and enhance the quality of the study. Moreover, when appropriate, researchers should carefully select original research and elevate the level of original research included in SRs/MAs, considering the GRADE approach.
4.5 LimitationsThis overview has certain limitations. Differences in RCTs design and rTMS intervention details may result in higher ROB for SRs/MAs, thereby reducing the quality of the evidence and methods. The details of rTMS intervention are complex, and we cannot conduct a quantitative combined analysis of its effect size. As we have previously discussed, the effectiveness of rTMS relies on accurate positioning. If the positioning error exceeds 5 mm, rTMS may be ineffective. At present, these positions are only accurate at the anatomical, and various functional compensation and decompensation will occur after cerebral cortex injury, and the function of neural network will also change. In addition to the accurate anatomical positioning, it is worth considering whether the future can combine functional brain detection technology to achieve more accurate and individualized rTMS for better treatment efficacy and longitudinal monitoring (Rossi et al., 2021). In addition to frequency, intensity and stimulation site, continuous and intermittent rhythms may also have different effects on cognitive performance. Based on the present results, it may help in clinical decision-making for AD treatment. Because quality assessment is a subjective process and different authors may have their own judgments about each factor, the results may differ from other reviews, although our overview has been evaluated and checked by two independent reviewers.
5 ConclusionBased on the evidence collected, rTMS appears to be effective and safe in improving cognitive function in AD patients, although the methodological quality of the SRs/MAs reduces the reliability of the conclusions and the overall quality is low. However, based on the available results, we still support the value of rTMS as an intervention to improve cognitive function in AD. In future studies, it is necessary to confirm the efficacy of rTMS in AD patients and provide more reliable and scientific data to contribute to evidence-based medicine.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributionsHX: Conceptualization, Data curation, Formal analysis, Investigation, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. Y-xL: Investigation, Methodology, Project administration, Writing – review & editing. Y-sX: Investigation, Methodology, Writing – review & editing. W-hF: Funding acquisition, Visualization, Writing – review & editing. H-xH: Methodology, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1383278/full#supplementary-material
ReferencesAceves-Serrano, L., Neva, J. L., and Doudet, D. J. (2022). Insight into the effects of clinical repetitive transcranial magnetic stimulation on the brain from positron emission tomography and magnetic resonance imaging studies: a narrative review. Front. Neurosci. 16:787403. doi: 10.3389/fnins.2022.787403
PubMed Abstract | Crossref Full Text | Google Scholar
Ahmed, M. A., Darwish, E. S., Khedr, E. M., El Serogy, Y. M., and Ali, A. M. (2012). Effects of low versus high frequencies of repetitive transcranial magnetic stimulation on cognitive function and cortical excitability in Alzheimer’s dementia. J. Neurol. 259, 83–92. doi: 10.1007/s00415-011-6128-4
PubMed Abstract | Crossref Full Text | Google Scholar
Bao, Z., Bao, L., Han, N., Hou, Y., and Feng, F. (2021). rTMS alleviates ad-induced cognitive impairment by inhibitng apoptosis in Samp8 mouse. Aging (Albany NY) 13, 26034–26045. doi: 10.18632/aging.203796
PubMed Abstract | Crossref Full Text | Google Scholar
Barker, A. T., Jalinous, R., and Freeston, I. L. (1985). Non-invasive magnetic stimulation of human motor cortex. Lancet 325, 1106–1107. doi: 10.1016/s0140-6736(85)92413-4
Crossref Full Text | Google Scholar
Begemann, M. J., Brand, B. A., Ćurčić-Blake, B., Aleman, A., and Sommer, I. E. (2020). Efficacy of non-invasive brain stimulation on cognitive functioning in brain disorders: a meta-analysis. Psychol. Med. 50, 2465–2486. doi: 10.1017/s0033291720003670
PubMed Abstract | Crossref Full Text | Google Scholar
Braak, H., Alafuzoff, I., Arzberger, T., Kretzschmar, H., and Del Tredici, K. (2006). Staging of Alzheimer disease-associated neurofibrillary pathology using paraffin sections and immunocytochemistry. Acta Neuropathol. 112, 389–404. doi: 10.1007/s00401-006-0127-z
PubMed Abstract | Crossref Full Text | Google Scholar
Chen, X., Liu, F., Lyu, Z., Xiu, H., Hou, Y., and Tu, S. (2023). High-frequency repetitive transcranial magnetic stimulation (Hf-rTMS) impacts activities of daily living of patients with post-stroke cognitive impairment: a systematic review and meta-analysis. Neurol. Sci. 44, 2699–2713. doi: 10.1007/s10072-023-06779-9
PubMed Abstract | Crossref Full Text | Google Scholar
Chen, X., Xiu, H., Hou, Y., Chen, X., Liu, F., and Tu, S. (2023). High-frequency repetitive transcranial magnetic stimulation (Hf-rTMS) on overall cognition in patients with post-stroke cognitive impairment: a systematic review and meta-analysis. Am. J. Phys. Med. Rehabil. doi: 10.1097/phm.0000000000002377
PubMed Abstract | Crossref Full Text | Google Scholar
Cheng, J., and Wu, W. (2016). Meta-analysis of the effect of high-frequency repetitive transcranial magnetic stimulation on Alzheimer’s disease. Chin J Practic Med 32, 2539–2543. doi: 10.3969/j.issn.1006-5725.2016.15.037
Crossref Full Text | Google Scholar
Dong, X., Yan, L., Huang, L., Guan, X., Dong, C., Tao, H., et al. (2018). Repetitive transcranial magnetic stimulation for the treatment of Alzheimer’s disease: a systematic review and meta-analysis of randomized controlled trials. PLoS One 13:e0205704. doi: 10.1371/journal.pone.0205704
PubMed Abstract | Crossref Full Text | Google Scholar
Dressler, D., Voth, E., Feldmann, M., and Benecke, R. (1990). Safety aspects of transcranial brain stimulation in man tested by single photon emission-computed tomography. Neurosci. Lett. 119, 153–155. doi: 10.1016/0304-3940(90)90821-p
PubMed Abstract | Crossref Full Text | Google Scholar
Jannati, A., Oberman, L. M., Rotenberg, A., and Pascual-Leone, A. (2023). Assessing the mechanisms of brain plasticity by transcranial magnetic stimulation. Neuropsychopharmacology 48, 191–208. doi: 10.1038/s41386-022-01453-8
PubMed Abstract | Crossref Full Text | Google Scholar
Kaur, D., Sharma, V., and Deshmukh, R. (2019). Activation of microglia and astrocytes: a roadway to neuroinflammation and Alzheimer’s disease. Inflammopharmacology 27, 663–677. doi: 10.1007/s10787-019-00580-x
PubMed Abstract | Crossref Full Text | Google Scholar
Kim, T. D., Hong, G., Kim, J., and Yoon, S. (2019). Cognitive enhancement in neurological and psychiatric disorders using transcranial magnetic stimulation (Tms): a review of modalities, potential mechanisms and future implications. Exp Neurobiol 28, 1–16. doi: 10.5607/en.2019.28.1.1
PubMed Abstract | Crossref Full Text | Google Scholar
Lefaucheur, J. P., Aleman, A., Baeken, C., Benninger, D. H., Brunelin, J., Di Lazzaro, V., et al. (2020). Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Clin. Neurophysiol. 131, 474–528. doi: 10.1016/j.clinph.2019.11.002
PubMed Abstract | Crossref Full Text | Google Scholar
Leng, F., and Edison, P. (2021). Neuroinflammation and microglial activation in Alzheimer disease: where do we go from here? Nat. Rev. Neurol. 17, 157–172. doi: 10.1038/s41582-020-00435-y
PubMed Abstract | Crossref Full Text | Google Scholar
Li, Y., Li, L., and Pan, W. (2019). Repetitive transcranial magnetic stimulation (rTMS) modulates hippocampal structural synaptic plasticity in rats. Physiol. Res. 68, 99–105. doi: 10.33549/physiolres.933772
Crossref Full Text | Google Scholar
Liang, B., Wang, X. W., Zhang, H., Wang, Y., Liang, T., and Tang, J. T. (2017). Meta-analysis of transcranial magnetic stimulation in patients with Alzheimer’s disease. Sci Technol Herald 35, 95–99.
Liao, X., Li, G., Wang, A., Liu, T., Feng, S., Guo, Z., et al. (2015). Repetitive transcranial magnetic stimulation as an alternative therapy for cognitive impairment in Alzheimer’s disease: a meta-analysis. J. Alzheimers Dis. 48, 463–472. doi: 10.3233/jad-150346
PubMed Abstract | Crossref Full Text | Google Scholar
Lin, Y., Jiang, W. J., Shan, P. Y., Lu, M., Wang, T., Li, R. H., et al. (2019). The role of repetitive transcranial magnetic stimulation (rTMS) in the treatment of cognitive impairment in patients with Alzheimer’s disease: a systematic review and meta-analysis. J. Neurol. Sci. 398, 184–191. doi: 10.1016/j.jns.2019.01.038
PubMed Abstract | Crossref Full Text | Google Scholar
Marucci, G., Buccioni, M., Ben, D. D., Lambertucci, C., Volpini, R., and Amenta, F. (2021). Efficacy of acetylcholinesterase inhibitors in Alzheimer’s disease. Neuropharmacology 190:108352. doi: 10.1016/j.neuropharm.2020.108352
Crossref Full Text | Google Scholar
Nguyen, J. P., Suarez, A., Le Saout, E., Meignier, M., Nizard, J., and Lefaucheur, J. P. (2018). Combining cognitive training and multi-site rTMS to improve cognitive functions in Alzheimer’s disease. Brain Stimul. 11, 651–652. doi: 10.1016/j.brs.2018.02.013
PubMed Abstract | Crossref Full Text | Google Scholar
O’Reardon, J. P., Solvason, H. B., Janicak, P. G., Sampson, S., Isenberg, K. E., Nahas, Z., et al. (2007). Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol. Psychiatry 62, 1208–1216. doi: 10.1016/j.biopsych.2007.01.018
PubMed Abstract | Crossref Full Text | Google Scholar
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). Prisma 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372:n160. doi: 10.1136/bmj.n160
PubMed Abstract | Crossref Full Text | Google Scholar
Pardo-Moreno, T., González-Acedo, A., Rivas-Domínguez, A., García-Morales, V., García-Cozar, F. J., Ramos-Rodríguez, J. J., et al. (2022). Therapeutic approach to Alzheimer’s disease: current treatments and new perspectives. Pharmaceutics 14:61117. doi: 10.3390/pharmaceutics14061117
PubMed Abstract | Crossref Full Text | Google Scholar
Rossi, S., Antal, A., Bestmann, S., Bikson, M., Brewer, C., Brockmöller, J., et al. (2021). Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: expert guidelines. Clin. Neurophysiol. 132, 269–306. doi: 10.1016/j.clinph.2020.10.003
PubMed Abstract | Crossref Full Text | Google Scholar
Schünemann, H. J., Oxman, A. D., Brozek, J., Glasziou, P., Jaeschke, R., Vist, G. E., et al. (2008). Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ 336, 1106–1110. doi: 10.1136/bmj.39500
留言 (0)