
記住我




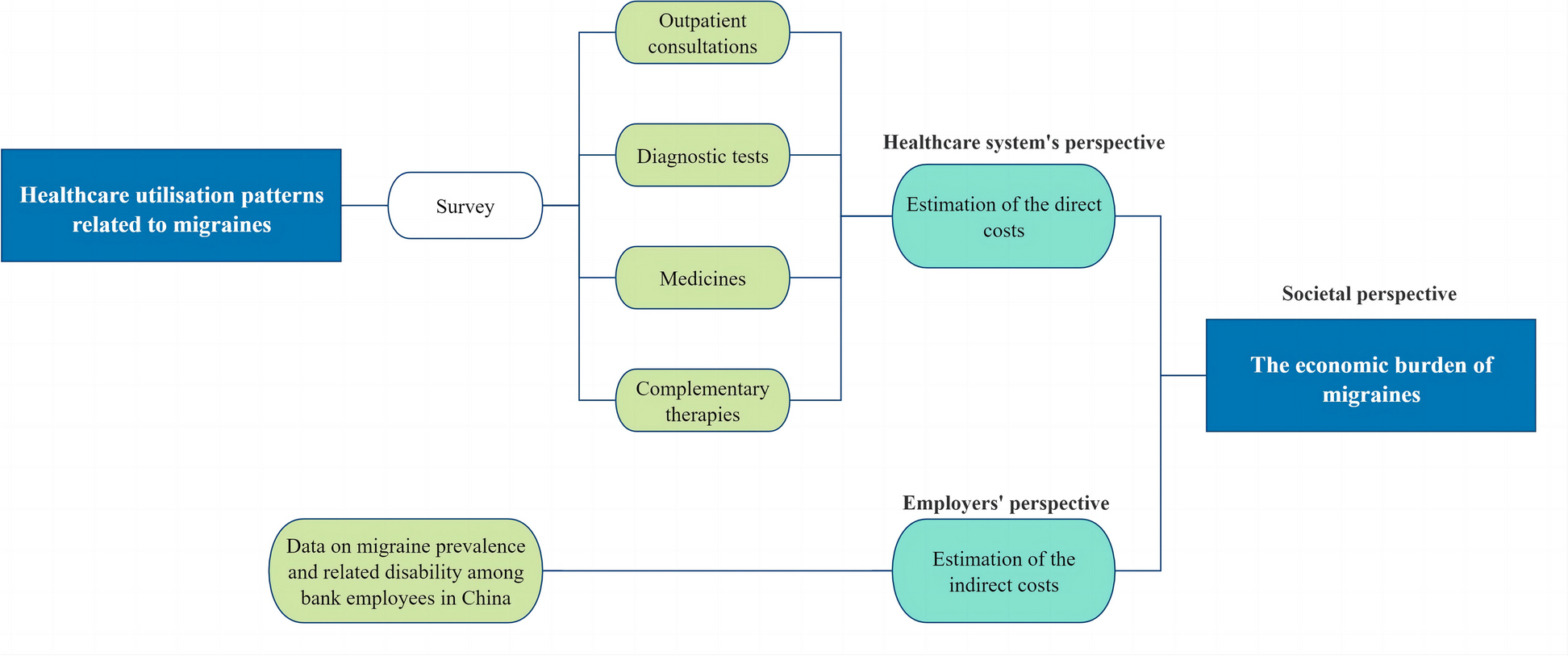

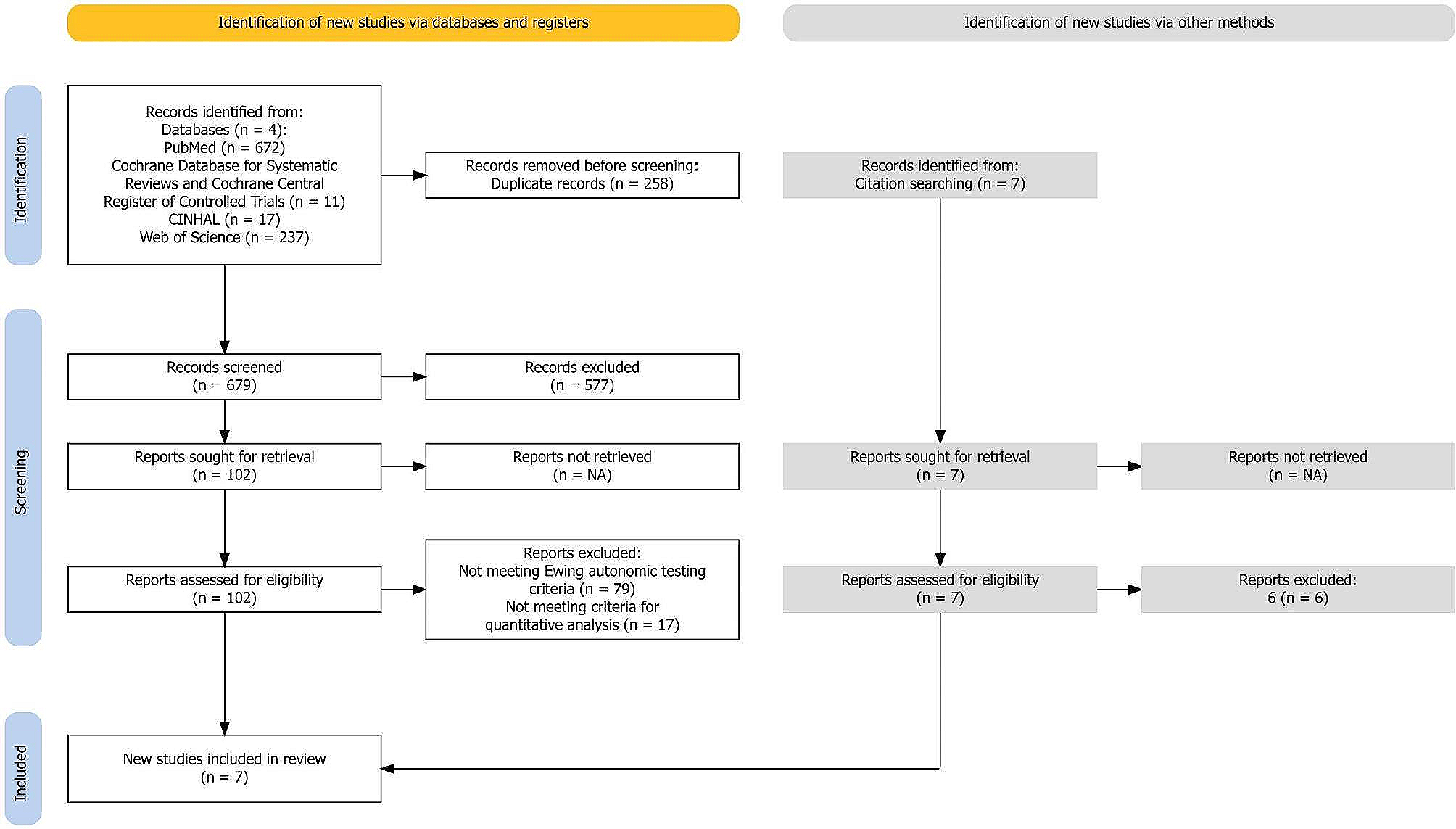
Figure 1 shows a graphical summary of the methodology used in this study.
Fig. 1
Graphical summary of the methodology used in this study
PatientsA convenience sample of patients consulting a specialized headache department from January 2019 to June 2022 was screened for inclusion. Only patients diagnosed with migraine in its chronic or episodic forms according to the ICDH-3, who satisfactorily completed a customized neuropsychological evaluation and a headache diary for at least one month were included. Patients who were pregnant, suffering from severe medical illnesses, or under treatment for psychiatric disorders were excluded.
Episodic or chronic migraine ICHD-3 diagnoses were performed by neurologists (PS & ML) based on information from paper diaries filled by patients. All included patients reported having a relatively stable headache frequency and intensity during the preceding months, similar to the one recorded in the headache diary. On these diaries, headache intensity, presence of nausea or vomiting, presence of photophobia and phonophobia, interference with daily activities, and intake of rescue medication were registered. Only the final diagnosis, and not the number or characteristics of monthly headache days and/or migraine days, were recorded in medical records.
Neuropsychologic profile-based classificationThe neuropsychological evaluation protocol comprised several tests. These tests were conducted to assess cognition, anxiety, depression, perceived stress, and headache-related impact and disability. The cognition tests involved the Verbal Paired Associates test from the Wechsler Memory Scale, the Wechsler Adult Intelligence Scale (WAIS) Reverse Digit Span subtest, the WAIS Digit-Symbol subtests, and the Trail Making Test A and B. Anxiety and depression were assessed through the Beck Anxiety Inventory (BAI) and Beck Depression Inventory-II (BDI-II) respectively. Perceived stress was evaluated using the Perceived Stress Scale 10-item version (PSS-10). Headache-related impact was assessed using the Headache Impact Test (HIT-6), and disability was measured using the Migraine Disability Assessment (MIDAS) (Table 1). Tests in the battery were selected based on the literature [7, 12,13,14] and the availability of locally adapted and validated versions, along with the existence of reliable reference data. Individual test results were converted into Z-scores based on normative data adjusted for age, gender, and education level. The Z-scores were then divided into three categories based on their range: mild alterations were between -1 and -1.5, moderate alterations were between -1.5 and -3, and severe alterations were below -3. Emotion and anxiety questionnaires have their own predetermined cut-off points. Evaluations were performed by a specialized psychologist (TCZ) in a dedicated room with adequate illumination, climatization, and sonorization. Patients were not using migraine medications known to impact cognitive abilities, nor had they utilized such medications in the preceding months. None of the patients were evaluated during a migraine attack.
Table 1 Psychological, cognitive, and severity aspects evaluated, and the tests employedStatistical analysesResults from the neuropsychological evaluation protocol were introduced into an automated K-means clustering algorithm implemented in SPSS (IBM® SPSS® statistics V26). K-means clustering is a form of unsupervised machine learning feature-based grouping technique, which separated the sample into two differing clusters based on their characteristics. We a priori defined a K=2 which allowed us to run comparisons between the two classification systems.
Diagnostic proportions and differences in neuropsychological assessment battery results were compared using the chi-squared test (categories) and ANOVA (Z-scores). Results from HIT-6 and MIDAS scores were compared between the two ICHD-3 diagnosis groups (i.e., chronic versus episodic) and the two neuropsychological profile-based classification groups (i.e., cluster one versus cluster two) using unpaired t-tests. p-values below 0.05 were considered statistically significant.
Voxel-based morphometry comparisonsFollowing the primary clinical part of this study, a complementary Voxel-based Morphometry (VBM) evaluation was performed to search for neuroanatomical contrasts between the two different grouping configurations (i.e., ICHD-3 diagnosis or automated K-means clustering).
High-resolution structural MRI images were obtained using a Philips Ingenia 3.0T scanner. A T1-weighted volumetric sequence with 1mm3 isotropic voxels was used for analysis. Forty patients (21 episodic and 19 chronic) from the original sample were originally included, but three had to be excluded after image visual inspection because of poor MRI quality (patient motion n=2, orthodontic appliances n=1). A final subset of 37 patients was available for evaluation. Following visual quality inspection, images were reoriented, co-registered with a template, segmented into different tissues (gray matter, white matter, cerebrospinal fluid, others), normalized, and smoothed (Gaussian Kernel, full-width half maximum (FWHM) of 8mm) as detailed in the software’s manual [15]. To enhance the normalization process and achieve a more precise alignment of the images, the Deformable Anatomical Registration Through Exponentiated Lie algebra (DARTEL) method was employed, minimizing inter-subject variability.
Image preprocessing and statistical tests were performed using SPM12 (http://www.fil.ion.ucl.ac.uk/spm) implemented in Matlab (The MathWorks 2021). Unpaired voxel-wise t-tests between groups derived from the ICHD-3 diagnosis or the neuropsychological profile-based K-means classification were carried out including age, sex, and total intracranial volume as covariates. A p-value <0.05 (Family-Wise Error (FWE) corrected) was considered statistically significant.
Ethical considerationsThe study was conducted following the principles of the Declaration of Helsinki and approved by the Ethics Committee of the School of Medicine University Hospital of the University of Córdoba. Written informed consent was not required for this study due to specific legal and ethical guidelines outlined in Law 25.326, Article 11(d) and Article 28, and Ministry of Health Resolution 1490/07, Chapter 4, Section 3. Therefore, all patients were provided comprehensive verbal explanations of the study and voluntarily consented to participate.
留言 (0)