
記住我



Data came from a cross-sectional study assessing a clinical cohort of TGD adolescents with psychometric self-report questionnaires. The data collection took place at the Hamburg Gender Identity Service for children and adolescents (Hamburg GIS) between January 2020 and December 2022. Thus, the study period fell within the time of the COVID-19 pandemic. The Hamburg GIS at the University Medical Center Hamburg-Eppendorf in Germany offers specialized diagnostics, counseling, and gender-affirming treatment to TGD youth and to youth who have questions about their gender or sexual identity. All families attending the Hamburg GIS are invited to participate in the study at their first appointment, thus before undergoing any form of counseling or treatment.
As part of a research project on “Gender- and Neurodiversity in Childhood and Adolescence” ongoing since 2020, the present study evaluated various updated questionnaires on the psychological health and the life experiences of TGD youth. The local ethics committee approved the study (12/2019-PTK-HH). Participation is voluntary, i.e., counseling or treatment is offered regardless of participation or nonparticipation in the study. All participants completed an informed consent form for their voluntary participation.
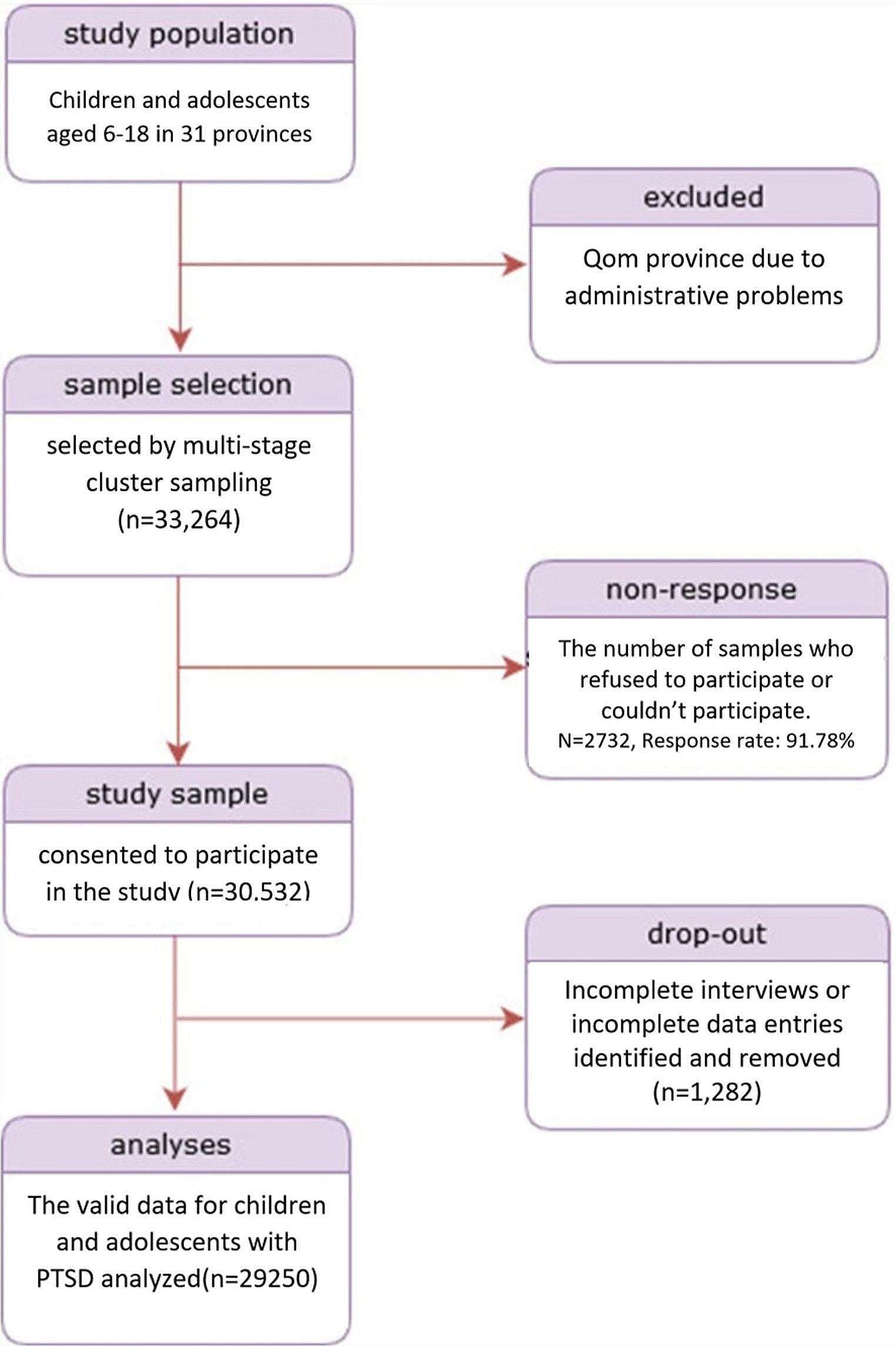
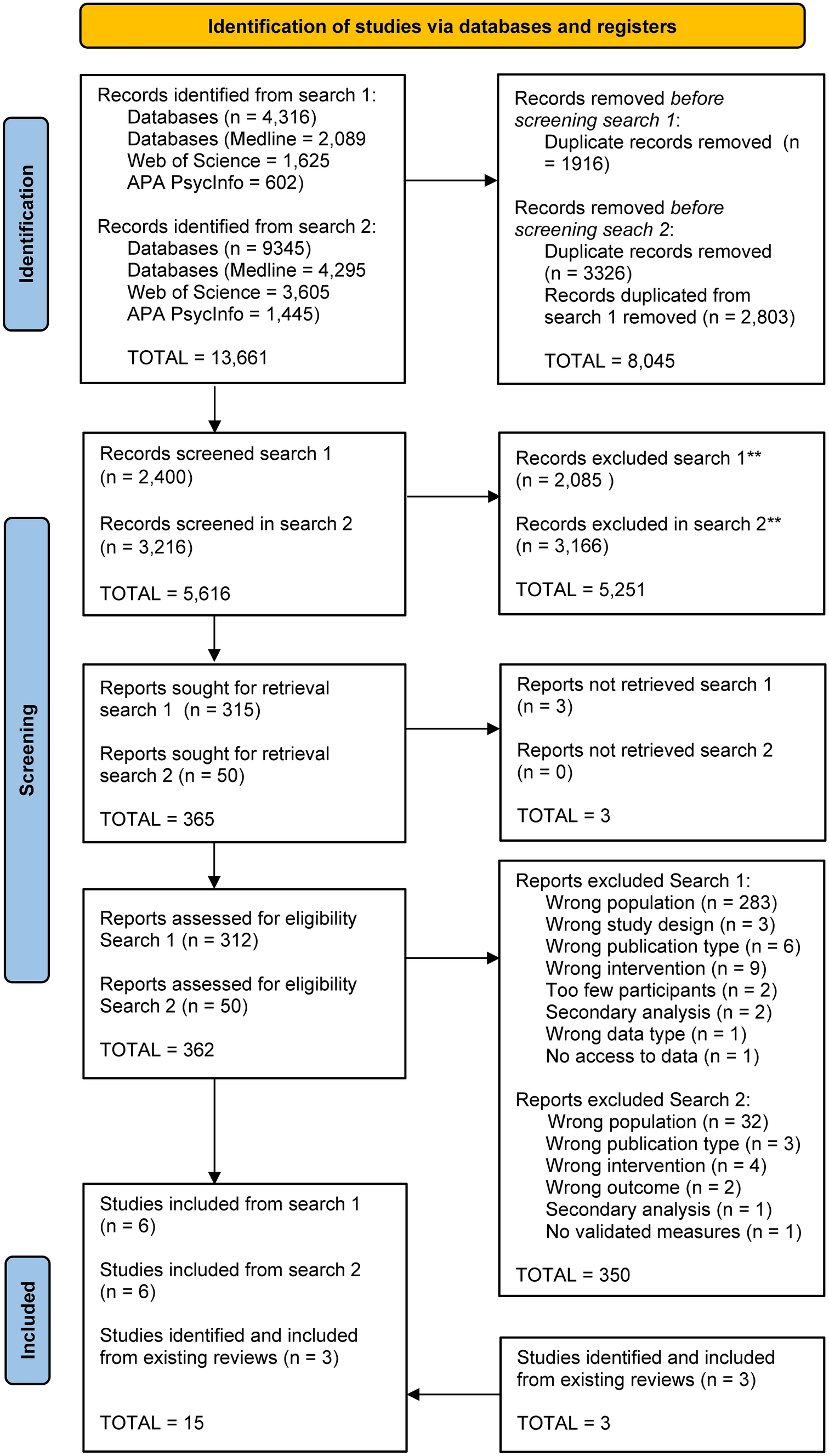
ParticipantsThe wider study population included children (aged 5–10 years) and adolescents (aged 11 years and above) who attended the clinic between January 2020 and December 2022. In this period, 415 families had presented to the Hamburg GIS (79% assigned female at birth [AFAB], 21% assigned male at birth [AMAB]; Fig. 1). Incomplete datasets, children, youth without a diagnosis of gender dysphoria, and other cases (for various reasons) were excluded from the analyses (see Fig. 1). The final sample comprised 165 TGD adolescents aged 11 to 18 years (87% AFAB, 13% AMAB) with a clinical diagnosis of gender dysphoria.
Fig. 1
Participants and sex ratios at the Hamburg GIS for children and adolescents
Variables and instrumentsSociodemographic as well as psychosocial characteristics and time spent onlineThe following sociodemographic characteristics were evaluated: birth-assigned sex, age at assessment (upon clinical entry), current gender identity, citizenship, parental socioeconomic status, and parental marital status and living situation. For detailed descriptions of the sociodemographic variables, see Levitan et al. [3] and Herrmann et al. [17].
In addition, we evaluated the following psychosocial characteristics to control for two predominately offline social experiences, which are well-documented risk and protective factors for internalizing problems in TGD youth (see Introduction): general family functioning and poor peer relations. The McMaster Family Assessment Device (FAD) was used to assess general family functioning [37]. The FAD has been used in previous studies on TGD youth [3, 10, 38]. For the present study, we used only the FAD subscale on general family functioning, which consists of 12 items, such as feeling accepted and understood (e.g., “Individuals are accepted for what they are”), supporting each other (“In time of crisis we can turn to each other for support”) and expressing feelings to each other (“We can express feelings to each other”). The adolescents rate the items on a 4-point scale (from 1 = “strongly agree” to 4 = “strongly disagree”). An average general family functioning score is created by adding the items and dividing the sum by the total number of items, resulting in a range from 1 to 4, with higher scores indicating lower levels of family functioning. For categorical analyses (problematic or unhealthy family functioning), the cutoff is 2.17 [39]. The internal consistency of the scale was good in the present study (Cronbach’s \(\alpha\) = .89).
Poor peer relations were assessed with the German 1991 version of the Youth Self-Report (YSR) [40, 41]. The YSR includes 119 items that adolescents rate on a 3-point scale ranging from 0 (“not true”) to 2 (“very true or often true”) concerning the past six months. An index for poor peer relations was created based on the following items: Item 25 (“I don’t get along with other kids”), Item 38 (“I get teased a lot”), and Item 48 (“I am not liked by other kids”). The poor peer relation index has been used in several clinical studies to assess problematic social interactions of TGD children and adolescents with peers [2, 3, 10]. The index can range from 0 to 6. Higher scores reflect poorer peer relations. In the present study, the internal consistency of the index was acceptable to questionable (Cronbach’s \(\alpha\) = .66).
To control for the quantity of Internet use, time spent online was measured with an item of the Trans Youth Social Media Questionnaire (TYSMQ). The TYSMQ is a self-constructed self-report questionnaire on TGD adolescents’ online activities and experiences. For its construction, we used and adapted items from two representative German studies on adolescents’ free time and media activities [19, 32]. We also added items to reflect the unique experiences of TGD adolescents. The questionnaire has already been used in another clinical study on TGD adolescents [17]. For time spent online, adolescents rated an item (“How many hours do you spend online/on the Internet daily?”) on an 8-point scale ranging from “none” to “7 or more hours.” Later, answers were dichotomized (0 = up to 5 h daily and 1 = more than 5 h daily) for analysis purposes.
Online (social) experiencesVarious online (social) experiences were measured with the TYSMQ and with single items. The following online (social) experiences were evaluated in the present study: experimenting with gender identity online (“Did you experiment with your gender identity on the Internet/social media before you did in everyday life?”), coming out online first (“Did you come out on the Internet/social media before you told your friends/parents?”), gender role online (“In which role or gender do you live on the Internet/social media?”), feeling understood and accepted in different life domains (e.g., “Do you feel understood and accepted on the Internet/social media for who you are?”), positive online social experiences (use of online support networks), and negative online social experiences (cyberbullying or other adverse online interactions). For more details on these items and the TYSMQ, please refer to Herrmann et al. [17].
For positive online social experiences (use of online support networks), adolescents were asked: “Do you visit online (Facebook) groups/forums or platforms that focus on networking, support, or treatment of transgender or LGBTQ people?” The item could be rated on a 4-point scale ranging from 0 (“never”) to 3 (“yes, often”). For the analysis, answers were divided into two categories: 0 = no (never) and 1 = yes (rarely too often).
For negative online social experiences (cyberbullying or other adverse online interactions), adolescents were asked whether they had ever had negative experiences online or experienced cyberbullying online or on social media. The item was rated on a 4-point scale from 0 (“never”) to 3 (“yes, often”). Similar to the positive online social experiences, two categories for negative online social experiences (0 = no and 1 = yes) were built. In addition, adolescents were able to indicate whether the negative online social experiences had been related to their gender identity or sexual orientation and whether they had been victim, perpetrator, or both victim and perpetrator of this behavior.
Internalizing problemsInternalizing problems were assessed with the YSR [40, 41]. Using the German population-based, age-specific, and sex-specific norm scores by Döpfner et al. [40], T scores for the three YSR scales (total problem score, internalizing, and externalizing problems) were computed to determine whether the scores of the present study were within the normal range of the German population. Furthermore, clinical range scores (> 90th percentile; T score > 63) were calculated. In the present study, the internal consistency of the internalizing scale was excellent (Cronbach’s \(\alpha\) = .92).
For exploratory purposes and to evaluate psychological functioning more comprehensively, YSR scores for externalizing and total problems (sum of all problems) were additionally calculated, and an index for suicidality was created. As suggested by the YSR manual [40] and to avoid artificial conflation, we excluded the following items for the calculation of the total problem score: asthma (Item 2), allergies (Item 4), socially desirable items (16 items), and cross-gender identification (Item 5 and Item 110). As described in previous studies [2, 42], Items 84 and 85 were set to zero if the free-text answers were gender-related. The internal consistencies of the externalizing scale (Cronbach’s \(\alpha\) = .86) and the total problem scale (Cronbach’s \(\alpha\) = .95) were good to excellent. In addition, two items from the YSR were used to create an index for suicidality, as in other clinical studies on TGD adolescents [4, 6, 43]: Item 18 on self-harming behavior and suicide attempt (“I deliberately try to hurt or kill myself”) and Item 91 on suicidal ideation (“I think about killing myself”). The sum score of the index ranges from 0 to 4, with higher scores indicating higher levels of suicidality. In the present study, the internal consistency of the index was acceptable to questionable (Cronbach’s \(\alpha\) = .67).
Statistical analysesT-tests and chi-square tests (or Fisher’s exact tests) were conducted to explore possible sex differences (AFAB vs. AMAB) in the sociodemographic and psychosocial characteristics and the time spent online and various online (social) experiences. Paired t-tests were performed to compare the degree of feeling understood and accepted online with different offline life domains. Standardized effect sizes (d and odds ratios, OR) were calculated to quantify the magnitude of the effect.
For a descriptive evaluation of internalizing problems, the raw scores, T scores, and clinical ranges (> 90th percentile; T scores > 63) for the YSR internalizing scale were used. In addition, we calculated 95% confidence intervals to compare the present sample with age- and sex-equivalent population-based German norms [40]. A significant deviation from the reference group can be assumed if the confidence intervals are not within the range of the T distribution (M = 50, SD = 10). Vice versa, whenever confidence intervals overlap, there is no significant difference [44]. For exploratory purposes, the externalizing scale, the total problem score, and the suicidality index were evaluated similarly.
For testing our hypotheses, a multiple linear regression analysis was performed. The raw scores of the YSR internalizing scale were used as an outcome variable. Predictors were entered in a block-wise manner. In the first step, the birth-assigned sex, age, general family functioning, and poor peer relations were entered as control variables. In the second step, positive online social experiences (use of online support networks) were added. In the third step, negative online social experiences (cyberbullying or other adverse online interactions) were introduced to the regression analysis. In the fourth step, the interaction between positive and negative online social experiences was added. An a priori power analysis (using G*Power) demonstrated that in a multiple linear regression analysis with 165 cases and seven predictors, a medium effect (f = 0.15) can be tested with a power of 95%. For exploratory purposes, similar analyses were conducted with externalizing problems, the total problem score, and the suicidality index as outcomes. As in other similar studies [3, 10], three items on poor peer relations (Items 25, 38, and 48) were excluded from the total problem score when exploring its association with online social experiences because the poor peer relation index was already a predictor in the model.
Single missing values were imputed with the expectation–maximization algorithm [45] and the mean values. SPSS 27 was used for all statistical analyses.
留言 (0)