
記住我


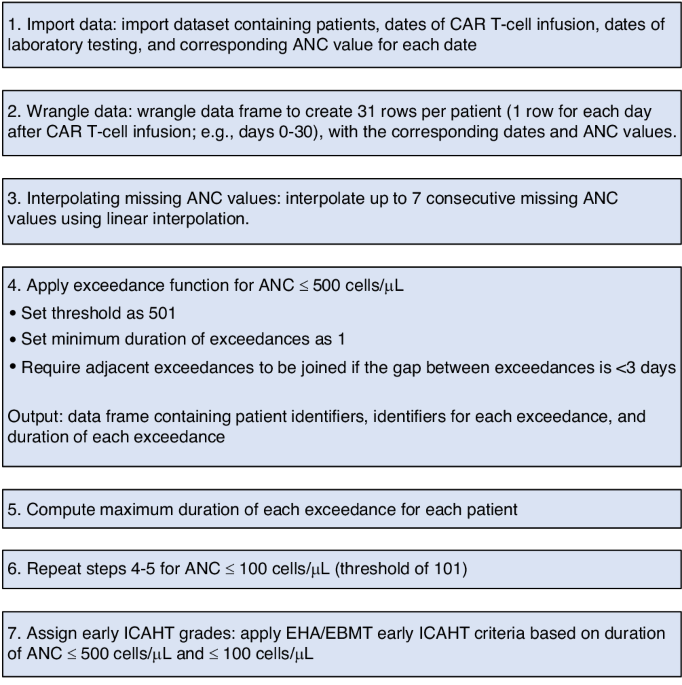
Between May 2013 and March 2015, thirteen transplant centers registered 172 patients for the study. Seven patients were excluded from the full analysis set, as five patients did not receive ATLG and for two patients no information on relapse was available. Twelve patients older than 65 years were included in the study, these were not excluded from the analyses. Thus, all analyses included 165 patients (Table 1).
Table 1 Baseline patient and disease characteristics in ATOS as compared to the ATLG treatment arm of our RCT.GvHD prophylaxis consisted of calcineurin inhibitors, mainly CSA (N = 154, 93%) with MTX or MMF and ATLG. Different dosing regimens were administered according to current local practice of centers. Median total ATLG dose was 46 mg/kg (IQR 32–60 mg/kg, range 15–91 mg/kg). A high variation of given total ATLG dose was to be observed between centers. Lowest total ATLG dose was given in the largest center with 40 patients (called center 1 with a median dose of 32 mg/kg, range 15–36 mg/kg), whereas median given total dose was around 60 mg/kg in most of the other centers (for details see Supplementary appendix Table S1).
With regard to disease status, 75 (45.5%) patients had early, 29 (17.6%) had intermediate, and 61 (37%) had advanced disease. Early disease was more frequent in AML and ALL, in patients with MAC, in patients with a mismatched transplant, and in patients with less than one year from primary diagnosis of current disease to transplantation. With regard to HLA-match, a transplant from a mismatched donor was given to 37 patients, 128 received a transplant from a matched donor. A mismatched transplant was given more often to younger patients, in cases of male patients with female donor, in patients with AML and MDS, and in patients with early disease status. With regard to conditioning intensity, 81 patients received MAC, 78 patients received RIC, five patients received other non-myeolablative regimens, and for one patient it was unknown. MAC was more applied in younger patients, in patients with ALL, and in patients with early or intermediate disease status. With regard to conditioning regimen group, 40 patients received regimen group A similar to Cy-TBI (29 MAC, 9 RIC, 2 other), 38 patients received regimen group B similar to Bu-Cy (28 MAC, 10 RIC), 64 patients received regimen group C similar to Bu-Flu (13 MAC, 50 RIC, 1 other), and 22 patients received regimen group D other regimens (11 MAC, 9 RIC, 2 other). Conditioning regimen group A was applied more often in younger patients, mainly in patients with ALL, more often in patients with early disease status, and in patients who received a transplant from a mismatched donor.
As compared to the 103 patients in the ATLG arm of our RCT [1], patients in ATOS were older, their disease status was more advanced, reduced intensity conditioning (RIC) was given, rates of transplantation with HLA mismatch (10/10, 4-digit) and with bone marrow were lower, and given median ATLG dose was lower (see Table 1).
Clinical efficacy endpointsThe cumulative incidence of engraftment (ANC > 1.0/nL) at month 3 after SCT was 0.93, 95% CI [0.90; 0.97], and that of engraftment (platelets > 50/nL) at month 12 after SCT was 0.88, 95% CI [0.82; 0.93].
Median follow-up of patients with regard to GvHD, relapse, and survival was 5.8 years (IQR 3.9–6.3 years). Estimated probabilities at 5 years follow up were for SGRFS 0.27, OS 0.52, DFS 0.43, NRM 0.23, relapse 0.34, acute GvhD °III/IV 0.13, severe chronic GvHD 0.27 (see Table 2). For a detailed comparison to the ATLG arm of our RCT [1] see supplementary appendix.
Table 2 Estimated probabilities of different endpoints over time in the ATOS study as compared to the ATLG arm of our RCT.OS rates differed dependent on disease status with 0.67, 0.49 and 0.37 for early, intermediate and advanced disease at 5 years (see Fig. 1). HRs adjusted for center and the above mentioned factors were intermediate vs. early 2.28, 95%-CI (1.11–4.68), and advanced vs. early 3.24, 95%-CI (1.70–6.16), p = 0.0016. With regard to HLA-match, GvHD incidences were slightly higher with a mismatch leading to a slightly decreased SGRFS rate with an HR adjusted for center (centers with less than 20 patients combined) and the above mentioned factors was 1.54, 95%-CI (0.96–2.47), p = 0.073 (see Fig. 2). With regard to conditioning intensity and conditioning regimen, no relevant relationships to clinical endpoints were observed.
Fig. 1: Probability of OS by disease status.
Estimated probability of overall survival (OS) by disease status - unadjusted and from Cox regression model adjusted for center, type of disease, conditioning intensity, time from primary diagnosis of current disease to transplantation, HLA-mismatch.
Fig. 2: Probability of SGRFS by HLA-mismatch.
Estimated probability of severe GvHD and relapse-free survival (SGRFS) by HLA-mismatch - unadjusted and from Cox regression model adjusted for center, patient age, patient and donor sex, type of disease, disease status, conditioning regimen.
Next, we analyzed the impact of the given ATLG dose on disease-relevant outcome parameters after transplantation. Figure 3 shows a slightly higher OS rate for patients treated with less than 45 mg/kg, which was chosen as cut-off dose, but after adjustment for center and prognostic factors, there was almost no difference. Noteworthy, the ATLG dose differed largely between centers, as shown in Table S1 (supplementary appendix). All 40 patients in the largest center 1 received less than 45 mg/kg, whereas 84 (67%) of 125 patients from the other centers received at least 45 mg/kg ATLG. As a consequence, the effect of the given ATLG dose cannot be separated from potential center effects. As shown in Fig. S1 (supplementary appendix), the highest OS rate were observed for patients from center 1 treated with about 30 mg/kg whereas OS rates of patients from other centers treated with less than 45 mg/kg and with at least 45 mg/kg were almost identical. This was true even after adjustment for other relevant prognostic factors. Consequently, no definite conclusions on the effects of the ATLG-dose can be drawn from this real-world data-set.
Fig. 3: Probability of OS by ATLG-dose.
Probability of overall survival (OS) by ATLG-dose - unadjusted and from Cox regression model adjusted for center, patient age, donor age, CMV status of patient, type of disease, disease status, time from primary diagnosis of current disease to transplantation, HLA-mismatch.
For a detailed outcome comparison to the ATLG arm of our RCT [2] see Table 2 and supplementary appendix Table S2, Figs. S2 and S3. In summary, the results are similar with the exception of a higher rate of severe chronic GvHD in this study as compared to the RCT, which may be due to different reporting.
New malignancies, hospital stays, quality of life, adverse drug reactionsOut of 165 study patients, two cases (one fatal) of lymphoproliferative disorders (PTLD) on days 55 and 74 after SCT were reported, in comparison to 5 (3 fatal) of 103 patients in the ATLG arm of our RCT [1]. Weekly PCR-testing for EBV copies was mandatory in ATOS, in contrast to the previous RCT, recruiting patients between 2003 and 2007. In ATOS, another reported malignancy was one recurrence of breast cancer on day 111 after SCT.
For further results on hospital stays, quality of life, adverse drug reactions, severe infections, and reasons of death see Supplementary appendix.
留言 (0)