
記住我
The translational path of generative AI in healthcare is a journey that involves the integration of this advanced technology into the clinical setting [54]. This process has the potential to revolutionize the way healthcare is delivered, by automating tasks and generating relevant information, thus enhancing the efficiency of healthcare delivery [26, 35]. Generative AI can automate routine tasks such as data entry, appointment scheduling and even some aspects of patient care like monitoring vital signs or administering medication. This automation can free up a significant amount of time for clinicians, allowing them to focus more on direct patient care. By reducing the administrative burden on healthcare providers, generative AI can help improve the quality of care and increase patient satisfaction [41, 53]. In addition to automating tasks, generative AI can also generate relevant information for clinicians. For example, it can analyse patient data to predict health outcomes, identify potential health risks and suggest personalized treatment plans. This ability to generate insights from data can help clinicians make more informed decisions about patient care, potentially leading to improved patient outcomes.
However, the accuracy and completeness of the information generated by AI are crucial. Inaccurate or incomplete information can lead to misdiagnosis or inappropriate treatment, which can harm patients [14, 55]. Therefore, it is essential to ensure that the AI systems are well designed and thoroughly tested to produce reliable results. Despite the potential benefits, adopting generative AI in clinical medicine is not a straightforward process. It requires careful planning and execution [56]. This includes understanding the needs of the healthcare providers and patients, selecting the right AI technology, integrating it into the existing healthcare systems and training the staff to use it effectively. Moreover, there are also legal and ethical considerations, such as data privacy and security, that need to be addressed. Furthermore, it is important to manage expectations about what generative AI can and cannot do. Clinicians’ expertise and their ability to empathize with patients are still crucial in providing high-quality care.
The successful translation of generative AI into clinical practice hinges on thoughtful adoption strategies grounded in implementation science. Two models offer robust scaffolds: the technology acceptance model (TAM) at the individual user level [57] and the Non-Adoption, Abandonment, Scale-up, Spread and Sustainability (NASSS) framework for organisational integration [58]. Grounded in sociopsychological theory, TAM provides an evidence-based model for how end-user perceptions shape acceptance of new technologies like generative AI [59]. Its core tenets posit that perceived usefulness and perceived ease of use prove most determinative of uptake. TAM offers a quantifiable approach for predicting and influencing adoption that deployment efforts must consider. Segmenting staff and assessing beliefs allows tailored interventions addressing barriers like skills gaps, engagement, workflow integration and demonstrable benefits. Equally crucial, the NASSS framework delivers a holistic methodology assessing multi-level variables implicated in successfully embedding innovations. Its seven critical domains encompass technology design, value propositions, adopter priorities, organisational dynamics, wider contextual factors and their complex interplay [58]. Together, these lenses reinforce introduced generative AI responsibly, monitor progress and recalibrate based on emerging feedback. Melding TAM and NASSS perspectives provides a powerful blueprint for thoughtfully ushering generative AI into the twenty-first-century healthcare. They bring implementable strategies for the sociotechnical transition such innovations necessitate, promoting buy-in, facilitating integration, delivering sustained value and ultimately transforming care.
Based on these frameworks, the below content discusses the key components or steps a healthcare organisation or service should consider in integrating generative AI in their service delivery. The description will enable partners as to how to prepare their organisations and workforce to adopt and integrate generative AI to enable optimal care delivery. However, the description does not cover wider policy and legislative aspects that are required to facilitate the introduction of generative AI to healthcare. These characteristics are unique to various jurisdictions and continue to evolve rapidly, therefore are considered beyond the scope of this article.
First component: acceptance and adoptionThe successful implementation of AI in healthcare hinges on the understanding and acceptance of its applications by end users [54], including medical professionals and patients. This comprehension fosters trust in AI systems, enables their effective use and aids in navigating ethical and regulatory challenges. Moreover, a solid grasp of AI promotes continuous learning and adaptation to the evolving landscape of AI technology. Therefore, investment in improving awareness for all partners is crucial to ensure the effective adoption and utilisation of AI in healthcare.
Utilising the TAM and NASSS frameworks to the implementation generative AI in healthcare involves consideration of the following components:
▪ Perceived usefulness: This refers to the degree to which a person believes that using a particular system would enhance his or her job performance. In the context of generative AI in healthcare, this could be how the AI can help in diagnosing diseases, predicting patient outcomes, personalizing treatment plans and improving administrative efficiency. For instance, AI could generate predictive models for patient outcomes based on their medical history, current health status and a vast database of similar cases.
▪ Perceived ease of use: This refers to the degree to which a person believes that using a particular system would be free of effort. For generative AI in healthcare, this could mean how easy it is for healthcare professionals to understand and use the AI system. This includes the user interface, the clarity of the AI’s outputs and the level of technical support available.
▪ Attitude towards using: The value proposition of generative AI in healthcare is compelling, offering benefits like cost-effectiveness, speed and personalized treatment options [5]. If healthcare professionals perceive the AI system as useful and easy to use, they are likely to develop a positive attitude towards using it. This positive attitude could be further enhanced by providing adequate training and support and by demonstrating the successful use of AI in similar healthcare settings.
▪ Behavioural intention to use: Once healthcare professionals have a positive attitude towards the AI system, they are more likely to intend to use it. This intention could be turned into actual use by providing opportunities to use the AI system in a safe and supportive environment and by integrating the AI system into existing workflows.
▪ Actual system use: The final step is the actual use of the AI system in daily healthcare practice. This could be encouraged by providing ongoing support and by continuously monitoring and improving the AI system based on user feedback and performance data.
In addition to these factors, the model also suggests that external factors like social influence and facilitating conditions can influence the acceptance and use of a new technology [57, 59]. In the case of generative AI in healthcare, these could include regulatory approval, ethical considerations, patient acceptance and the overall healthcare policy and economic environment.
Second component: data and resourcesAdopting generative AI involves preparing data and resources within an organisation to effectively utilise this technology. This is a complex process requiring a systematic and strategic approach that involves several key steps.
▪ Identifying use cases: Healthcare organisations need to begin by identifying the specific use cases where generative AI can bring value. Generative AI aims to address various medical conditions, from chronic diseases like diabetes to acute conditions like stroke [6, 38, 60]. The complexity of the medical condition often dictates the level of sophistication required from the AI model. For instance, using AI for diagnostic imaging in cancer is complex and requires high accuracy. Understanding the specific use cases will help guide the data preparation process.
▪ Data collection: Generative AI models learn from data [8], so the healthcare organisation needs to collect and prepare relevant data for training the models. This could involve gathering existing primary data from various sources within the organisation or collecting new data if necessary. The data then needs to be cleaned and preprocessed, which may involve tasks such as removing duplicates, handling missing values and normalizing data.
▪ Data cleaning and preprocessing: It is necessary to clean and preprocess the collected data to ensure its quality and consistency [61, 62]. This may involve removing duplicates, handling missing values, standardizing formats and addressing any other data quality issues. Preprocessing steps may also include data normalization, feature scaling and data augmentation techniques to enhance the training process. It is important to highlight the need for uniformity in the quality of the datasets to enable seamless cross-functional data integration. Also, data quality is crucial as generative AI algorithms learn from data. The quality of data can be affected by various factors such as noise, missing values, outliers, biased data, lack of balance in distribution, inconsistency, redundancy, heterogeneity, data duplication and integration.
▪ Data annotation and labelling: Depending on the use case, the organisation may need to annotate and label the data to provide ground truth and clinical standard information for training the generative AI models, specifically for fine-tuning LLMs with local data [10]. This could involve tasks such as image segmentation, object detection, sentiment analysis or text categorization. Accurate and comprehensive annotations are essential for training models effectively.
▪ Data storage and management: Their will be a requirement to establish or utilise a robust data storage and management system to handle the large volumes of data required for generative AI. This may involve setting up a data warehouse, cloud storage or utilising data management platforms. All the while ensuring that the data is organised, accessible and secure for efficient training and model deployment. Data federation is a technology that can be considered here as it enables the creation of a physically decentralized but functionally unified database. This technology is particularly useful in healthcare as it allows various sources of data to keep the data within their firewalls. However, this step may not be required in most instances of the use of LLMs, particularly if they are drawn upon through application programming interface (API) calls or cloud services.
▪ Computational resources: Generative AI models often require significant computational power and resources for training and inference such as GPUs or cloud computing services [8, 15]. In-house development and training of LLMs requires significant computational resources, which organisations must carefully consider [63]. Commercial LLMs offered through cloud services or APIs spare organisations this infrastructure burden. However, for those intent on training proprietary models tuned to their specific data and use cases, securing sufficient computing capacity is critical.
Factors that impact computational requirements include model size, training data volume and speed of iteration desired. For example, a firm aiming to train a model with over a billion parameters on tens of billions of text examples would likely pursue a high-performance computing cluster or leverage cloud–based machine learning platforms. The precise hardware configuration—including GPUs/TPUs, CPUs, memory, storage and networking—scales with the model architecture and training plan [63].
Ongoing model development and fine-tuning also necessitates available compute. Organisations can choose between continuing to allocate internal resources or outsourcing cycles via cloud services [63]. Budgetary planning should account for these recurring compute demands if continually enhancing in-house LLMs is a priority. Overall, while leveraging external LLMs can minimise infrastructure investments, serious internal LLM initiatives can rival the computational scale of industrial research labs.
Third component: technical integrationIntegrating generative AI into a healthcare information system or platform can bring numerous benefits, such as improved disease diagnosis, enhanced patient monitoring and more efficient healthcare delivery. However, generative AI technologies like GANs and LLMs are complex to understand and implement [8]. The technology’s maturity, reliability and ease of integration into existing systems are crucial factors affecting its adoption [58]. Therefore, integrating generative AI into a hospital or healthcare information system involves several steps ranging from understanding the needs of the system to implementing and maintaining the AI solution. The first step in integrating generative AI into a healthcare system is to identify the focus area of implementation [62]. This could be anything from improving patient care, streamlining administrative tasks, enhancing diagnostic accuracy or predicting patient outcomes. Once the need is identified, the right AI model needs to be chosen. Generative AI models, such as GANs, can be used for tasks like synthesising medical images or generating patient data [6, 37). LLMs can be used for EHR analysis and as a clinical decision support tool [40]. Once the model is chosen, it needs to be trained on the collected data. This involves feeding the data into the model and adjusting the model’s parameters until it can accurately predict outcomes or generate useful outputs.
Once the AI model is trained and tested, it can be integrated into the healthcare information system [56, 62]. This involves developing an interface between the AI model and the existing system, ensuring that the model can access the data it needs and that its outputs can be used by the system. Developing such an interface or API allows the generative AI models to be seamlessly integrated into the organisational or clinical workflow. After integration, the AI system needs to be extensively tested to ensure its functionality, usability and reliability.
Regular maintenance is also necessary to update the model as new data becomes available and to retrain it if its performance drops [56, 62]. Furthermore, gathering regular/scheduled feedback from healthcare professionals will ensure the organisation can make necessary refinements to improve the system’s performance.
When leveraging external LLMs for healthcare applications, stringent data governance practices are imperative to safeguard sensitive patient information [64]. As text or speech data gets routed to third-party LLM services for analysis, the contents contain protected health information (PHI) and personally identifiable information (PII) that must remain confidential.
While LLMs themselves are static analysis models rather than continuously learning systems, the vendors hosting these models and powering predictions still physically or computationally access submitted data [65, 66]. Irrespective of the vendors’ reassurances about privacy commitments, obligations and restrictions on ingesting customer content for model retraining, residual risks of data leakage or unintended retention persist. To mitigate these risks, comprehensive legal contracts between the healthcare organisation and LLM vendor are foundational to ensuring PHI/PII protection in accordance with health regulations. Business associate agreements, data usage agreements and master service provider contracts allow formally codifying allowable LLM data processing, storage, transmission and disposal protocols. Such contracts also establish liability and enforcement mechanisms in case of a breach attributed to the vendor, including notification, indemnification and restitution clauses. Strict access controls, encryption schemes, activity audit protocols and authorization procedures should complement these contractual protections. While LLMs themselves may not endlessly accumulate healthcare data like perpetually learning systems, due diligence around the long-term fate of data sent to LLM prediction services remains highly advisable for risk-averse legal and compliance teams [14]. Establishing robust data governance for emerging clinical LLM integration can prevent problematic regulatory, ethical and reputational exposure [64].
While beyond the scope of this article to discuss in detail, the organisation will additionally have a responsibility to ensure the AI system complies with relevant healthcare regulations and privacy laws [55], such as Health Insurance Portability and Accountability Act (HIPAA) in the USA or General Data Protection Regulation (GDPR) in the European Union.
Fourth component: governanceWhile generative AI has several potential applications in clinical medicine, there are also several challenges associated with its implementation. Some of the challenges include the following:
▪ Data availability: Generative AI requires large amounts of data to train models effectively [8]. However, in clinical medicine, data is often limited due to privacy concerns and regulations. This can make it difficult to train models effectively.
▪ Bias in training data: Generative AI models require large amounts of training data to learn patterns and generate new data. If the training data is biased, the generative AI model will also be biased [13]. For example, if the training data is skewed towards a particular demographic group, the generative AI model may produce biased results for that group.
▪ Transparency: While powerful LLMs like ChatGPT demonstrate impressive conversational ability, the opaque sourcing of their massive training corpora has rightly drawn scrutiny [64, 65]. Absent transparency around the origin, copyright status and consent policies of underlying data, legal and ethical blind spots remain. For commercially offered LLMs, details of training processes understandably remain proprietary intellectual property. However, the use of scraped web pages, private discussions, or copyrighted content without permission during model development can still create liability. Recent lawsuits alleging unauthorised scraping by LLM providers exemplify the growing backlash.
▪ Model interpretability: Generative AI models can be complex and difficult to interpret, making it challenging for clinicians to understand how the model arrived at its conclusions [13, 67]. This can make it difficult to trust the model’s output and incorporate it into clinical decision-making.
▪ Inaccurate generation: While LLMs demonstrate impressive fluency and versatility in conversational applications, their reliability breaks down when applied to high-stakes domains like healthcare [14, 55]. Without the contextual grounding in factual knowledge and reasoning capacity needed for medical decision-making, LLMs pose substantial patient safety risks if overly trusted by clinicians [14]. Hallucination errors represent one demonstrated failure mode, where LLMs confidently generate plausible-sounding but entirely fabricated responses lied outside their training distributions. For patient assessments, treatment plans or other clinical support functions, such creative falsehoods could readily culminate in patient harm if not rigorously validated [64]. Additionally, LLMs often ignore nuanced dependencies in multi-step reasoning that underlie sound medical judgments. Their capabilities centre on statistical associations rather than causal implications [68]. As such, they frequently oversimplify the complex decision chains requiring domain expertise that clinicians must weigh. Blindly accepting an LLM-generated diagnostic or therapeutic suggestion without scepticism can thus propagate errors.
▪ Regulatory and ethical issues: The use of generative AI in clinical medicine raises several regulatory and ethical issues [14], including patient privacy, data ownership and accountability. Regulatory policies, ethical considerations and public opinion form the wider context. Data privacy laws like GDPR in Europe or HIPAA in the USA have implications for AI in healthcare [65]. These aspects need to be addressed to ensure that the use of generative AI is ethical and legal.
▪ Validation: Generative AI models need to be validated to ensure that they are accurate and reliable [62]. This requires large datasets and rigorous testing, which can be time-consuming and expensive.
To minimise risks arising from the application of generative AI in healthcare, it is important to establish a governance and evaluation framework grounded in implementation science [64]. Frameworks such as the NASSS framework and the TAM should inform subsequent steps to promote responsible and ethical use of generative AI [58, 69]. This implementation science informed approach includes several steps to ensure appropriate testing, monitoring and iteration of the technology. The NASSS framework provides a useful lens for assessing the complex adaptive systems into which generative AI solutions would be embedded [58]. This framework examines factors like the condition, technology, value proposition, adopter system, organisation, wider context, and interaction and mutual adaptation over time. Analysing these elements can reveal barriers and enablers to adopting generative AI across healthcare organisations. Similarly, the TAM focuses specifically on human and social factors influencing technology uptake [59]. By evaluating perceived usefulness and perceived ease of use of generative AI systems, TAM provides insights into how both patients and providers may respond to and interact with the technology. TAM encourages stakeholder participation in system design to optimize user acceptance.
Both NASSS and TAM demand a thoughtful change management strategy for introducing new technologies like generative AI. This means conducting iterative testing and piloting of systems, co-developing governance policies with diverse voices, emphasizing transparency, providing extensive user training resources, developing protocols to assess AI quality and fairness, allowing user customization of tools, and continually evaluating impact to enable appropriate adaptation over time. Drawing from these models ensures responsible and ethical integration guided by end-user needs. The following are corresponding steps:
▪ Establish or utilise a governance committee: This committee should be composed of experts in AI, healthcare, ethics, law and patient advocacy. The committee’s responsibility is to supervise the creation and implementation of generative AI applications in healthcare, making sure they adhere to the highest moral, statutory and professional standards.
▪ Develop relevant policies and guidelines: Create policies and guidelines that address issues like data protection and security, informed consent, openness, responsibility and fairness in relation to the usage of generative AI in healthcare. The guidelines should also cover potential AI abuse and lay out precise reporting and resolution processes.
▪ Implement robust data management practices: This includes ensuring data privacy and security, obtaining informed consent for data use, and ensuring data quality and integrity. It also involves using diverse and representative datasets to avoid bias in AI outputs.
▪ Mitigate inaccurate generated data: Overall, while LLMs have strengths in certain narrow applications, their limitations in recalling latest findings, grounding advice in biomedical knowledge and deliberative analytical thinking pose risks in clinical roles [14]. Mitigating these requires both technological and process safeguards. At minimum, meticulous testing on massive, validated datasets, transparent uncertainty quantification, multi-modal human-AI collaboration and consistent expert oversight prove essential before contemplating LLM adoption for patient-impacting functions. With careful governance, LLMs may aid clinicians but cannot replace them.
▪ Risk assessment: Prior to implementation, healthcare organisations must undertake structured risk assessments to inventory and quantify potential patient harms from generative AI adoption. Multi-disciplinary teams including clinicians, IT security, legal/compliance, risk management and AI engineers should participate. A broad examination of use cases, data dependencies, performance assumptions, safeguards, governance and liability scenarios provide the foundation. Identified dangers span clinical inaccuracies like inappropriate treatment suggestions to operational risks like biased outputs or diagnostics halted by technical outages. Other key considerations are malicious misuse, defects propagating as training data and breach of sensitive records compromising privacy or trust.
For each plausible risk, the assessment calibrates probability and severity estimates for variables like user types, information classes and mitigating controls. Continuous risk monitoring based on leading indicators and usage audits ensures the initial assessment adapts alongside inevitable model and application changes over time. Periodic probabilistic modelling using safety assurance methodologies further reinforces responsible governance. Overall, a nimble quantified risk approach prepares organisations to responsibly pursue generative AI’s benefits while protecting patients.
▪ Ensuring transparency: Ensure transparency of generative AI models by providing clear documentation of the underlying algorithms, data sources and decision-making processes. This promotes trust and enables healthcare professionals to understand and interpret the generated outputs. For risk-averse healthcare organisations, partnering with LLM vendors who refuse reasonable data transparency raises concerns. If unsuitable, illegal or fraudulent data underpins model predictions, patient safety and organisational reputation may suffer [13, 68]. Furthermore, litigation alleging regulatory noncompliance, privacy violations or misrepresentation based on questionable LLM data sourcing could follow [14]. Nonetheless, for many clinical functions, externally developed LLMs can sufficiently assist physicians without full transparency into underlying corpora. Simple conversational applications likely pose little concern. However, for more impactful care recommendations or patient-specific outputs, clinicians should validate suggestions accordingly rather than presume integrity [64]. Overall, the inaccessible nature of commercial LLM training data is an obstacle, but not a wholesale deal-breaker with careful governance around how predictions get utilised. Still, transparency remains an ongoing advocacy issue that healthcare providers should champion [64].
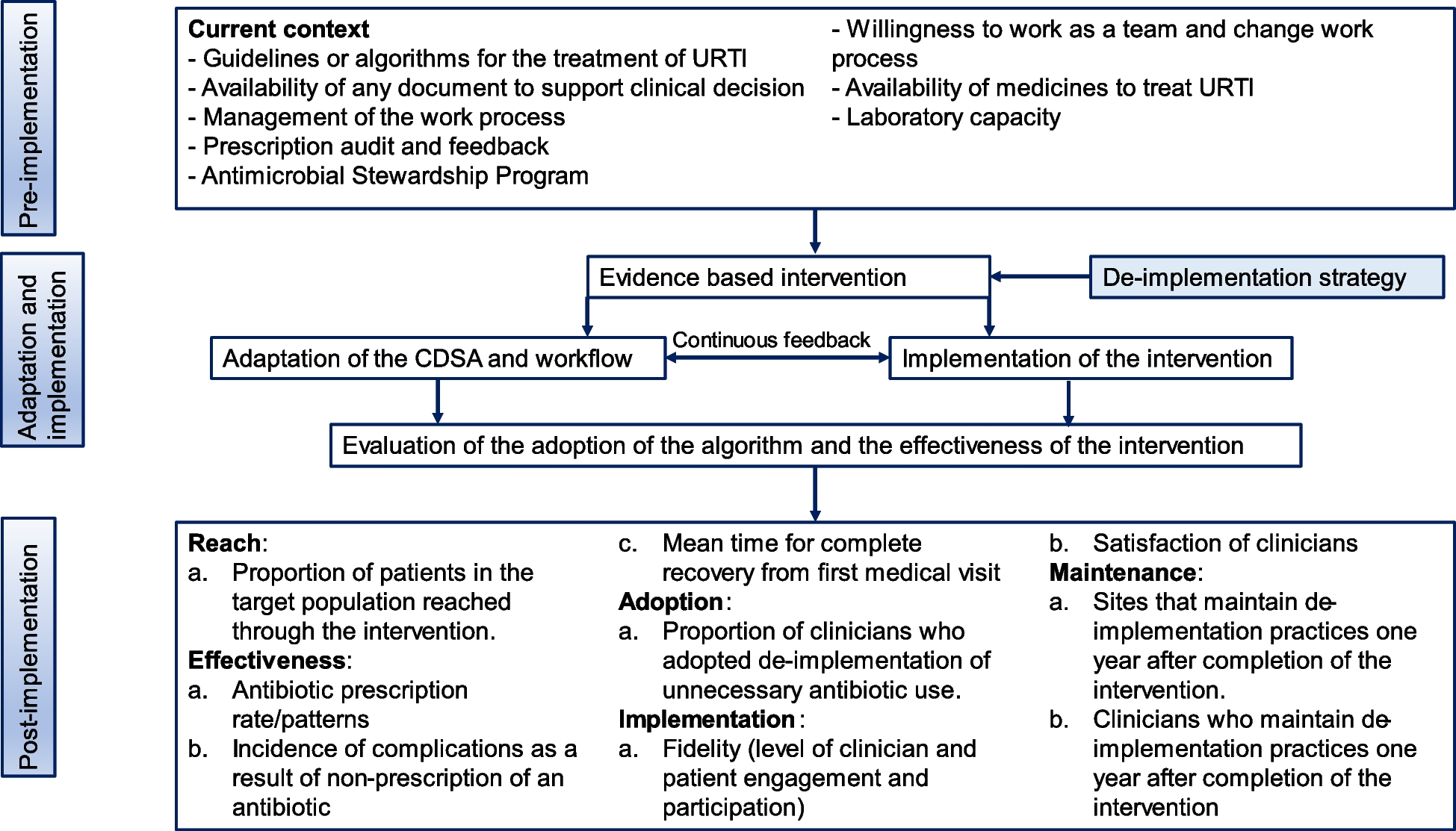
▪ Regulatory compliance: Ensure compliance with relevant regulatory frameworks, such as data protection laws and medical device regulations. Collaborate with regulatory authorities to establish guidelines specific to generative AI in healthcare Establishing procedures for ongoing monitoring and evaluation of the models is crucial in addition to the measures to enable governance for the generative AI models [67, 70]. This involves collecting input from patients and healthcare experts as well as regular monitoring of performance, safety and ethical considerations. Healthcare organisations can reduce risks and guarantee the appropriate and ethical use of generative AI in healthcare by adhering to every step in this framework (Fig. 2). The governance framework harnesses the potential advantages of generative AI technology while promoting openness, responsibility and patient safety.
Fig. 2
留言 (0)