
記住我

Giulio Metro (GM): Hello and welcome to this podcast on pre- or perioperative chemoimmunotherapy (chemo-IO) for resectable stage III non-small cell lung cancer (NSCLC). As you may already be aware, recent evidence has clearly suggested a benefit for pre- or perioperative chemo-IO for resectable stage II–IIIB NSCLC patients [1,2,3,4,5,6]. However, some controversies have emerged with regard to how this strategy should be implemented in clinical practice. We will try to address few of them in this podcast. We decided to exclude stage II patients from the discussion. In fact, even though perioperative chemo-IO may be considered in these patients, upfront surgery remains a valid and widely chosen option. Conversely, we focused only on stage III NSCLCs, because these patients are those who may benefit the most from a shared decision-making process among different physicians within the multidisciplinary team (MDT). Specifically, resectable stage III NSCLCs require an insightful discussion, primarily between the thoracic surgeon, the oncologist, and the radiotherapist. As this podcast focuses mainly on anticancer medical treatment and surgery, there is no radiotherapist involved in it.
My name is Giulio Metro. I am an oncologist at the Santa Maria della Misericordia Hospital in Perugia, Italy, and I am mainly involved in the treatment of patients with thoracic malignancies. I am joined by Dr. Luca Bertolaccini, an experienced thoracic surgeon at the European Institute of Oncology (IEO) Scientific Institute for Research, Hospitalization and Healthcare (IRCCS) in Milan, Italy.
Luca Bertolaccini (LB): Thank you, Giulio, for the opportunity to discuss this critical topic with you.
GM: Thanks, Luca, for accepting this invitation actually. So, let’s start with the discussion. We know that the definition of resectable stage III NSCLC is highly dependent on what the thoracic surgeon deems to be resectable or not. Luca, do you think that a clear definition of resectability exists?
LB: The consensual definition of resectable stage III NSCLC has been recently established through the collaboration of the European Organisation for Research and Treatment of Cancer (EORTC)-Lung Cancer Group and various scientific societies [7]. Patients deemed medically operable who may undergo multiple surgical procedures, from lobectomy to pneumonectomy, are included in this definition. Upfront resectability evaluation is mandatory, excluding cases of Pancoast tumors.
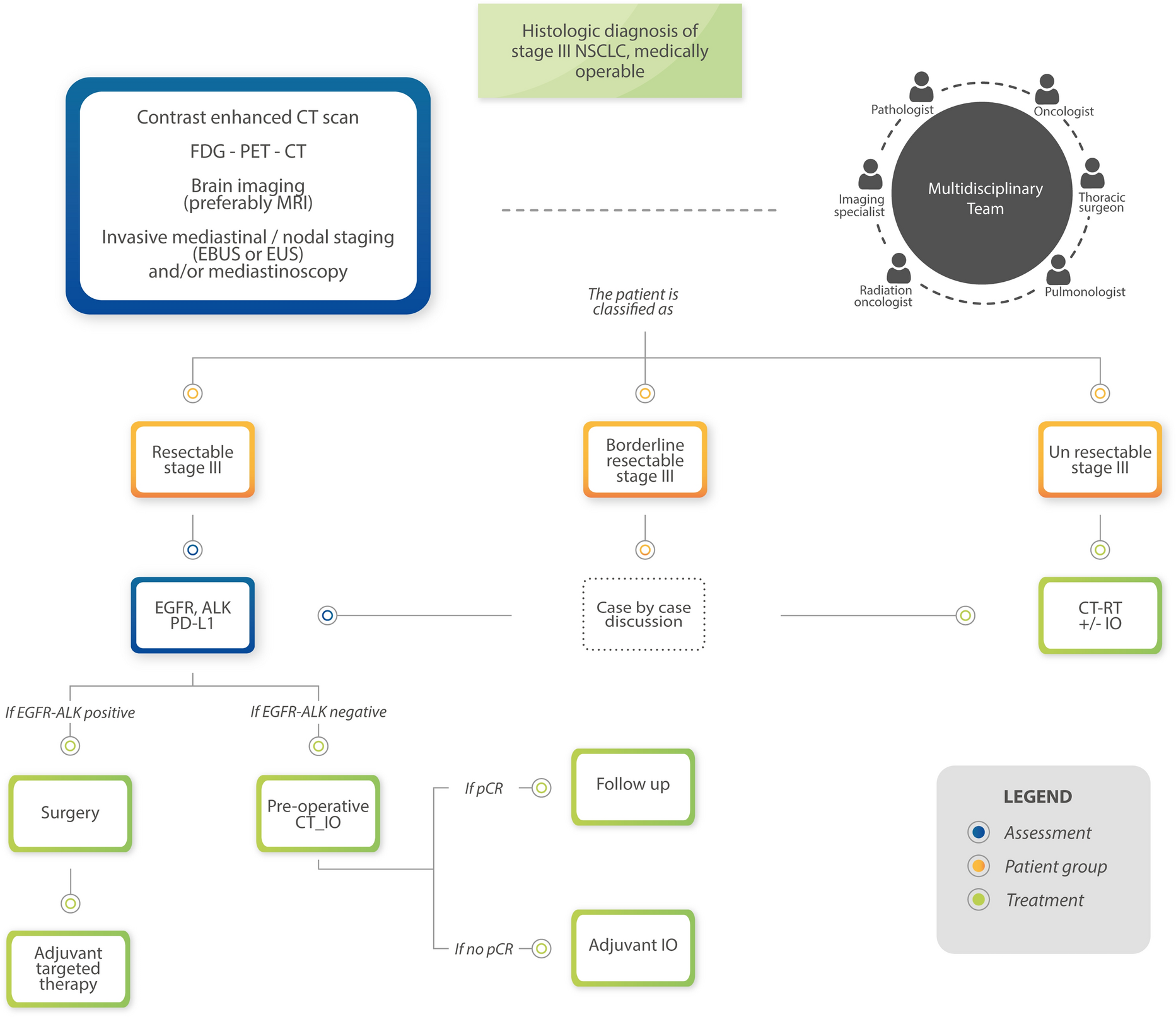
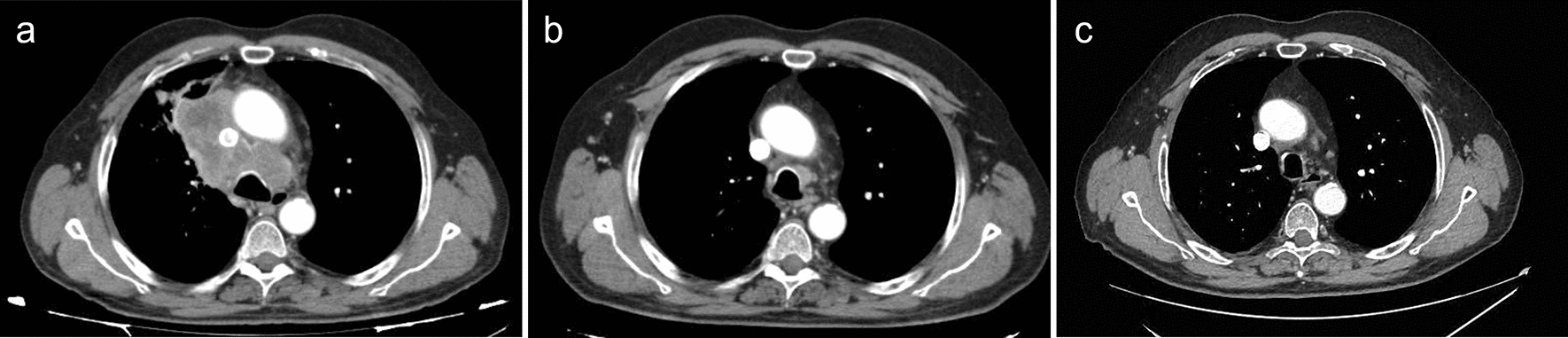
The resectability criteria varies according to the stage of the disease. For stage IIIA with cT3 N1 tumors, pathological exclusion of N2 involvement is necessary (Fig. 1). Regardless of specific T characteristics, cT3 N1 tumors are considered resectable. In the case of stage IIIA with cT1–2 N2 tumors, single-station N2, which is nonbulky and noninvasive, is resectable. Multiple-station N2 nonbulky and noninvasive cases necessitate individual evaluation for potential resection. The stage IIIA with cT4 N0–1 tumors may be resectable if separate nodules or size-based criteria are met. However, infiltration of major structures requires a detailed assessment in specialized centers where I have the privilege to work. Specifically, the use of adjunctive imaging techniques [for instance, cardiac and vascular magnetic resonance imaging (MRI)] may help select patients suitable for surgery in case the tumor invades major blood vessels and/or the heart.
Fig. 1
Flowchart of medically operable stage III non-small cell lung cancer. NSCLC non-small cell lung cancer, CT scan computed tomography scan, FDG-PET-CT fluorodeoxyglucose positron emission tomography–computed tomography, CT-IO chemoimmunotherapy, IO immunotherapy, CT-RT chemoradiotherapy, pCR pathologic complete response
For stage IIIB, tumors classified as cT3–4 N2 are resectable if they involve a single station N2. Limited discrete N2 multistation involvement may be considered for resection, with decisions made on a case-by-case basis. Stage IIIB tumors with cT1–2 N3 or stage IIIC with cT3–4 N3 involvement and infiltration of significant structures are considered to be unresectable.
So, it is important to note that while these criteria serve as a benchmark for evaluating the surgical R0 resection rates, the ultimate decision on the most appropriate treatment strategy lies on the MDT, considering all clinical factors and patient-specific variables. These guidelines provide a standardized approach for clinical trials and enhance the precision of treatment decisions for patients with stage III NSCLC.
GM: Thanks Luca, that is a great insight you gave us. Indeed, the decision on the technical resectability of the tumor should be made by the thoracic surgeon within the MDT. With regard to this, clinical staging should be meticulous. More specifically, it should include invasive mediastinal nodal staging to assign the correct stage and evaluate the extent of mediastinal involvement in terms of lymph nodes. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic ultrasound fine-needle aspiration (EUS-FNA) are now commonly adopted as the preferred methods for mediastinal lymph node staging, and their use should be advocated whenever it is required as per clinical guidelines [8]. However, as an oncologist, I would also like to focus on how the knowledge of tumor biomarker status would inform whether patients should undergo preoperative chemo-IO followed by surgery or immediate surgery. Currently, immunotherapy has been demonstrated to be poorly active in advanced NSCLC patients with EGFR mutations and ALK rearrangements [9]. As a result, it has been assumed that immunotherapy is also likely to be poorly effective in earlier stages of disease. For this reason, most of the available randomized studies comparing perioperative chemo-IO with preoperative chemotherapy alone specifically required documentation of an EGFR and ALK wild-type status prior to enrollment [2, 3, 5, 6]. Another study, CheckMate 816, which randomized patients to preoperative chemo-IO versus preoperative chemotherapy, did not overtly ask for EGFR and ALK assessment for enrollment. However, the same trial excluded patients who had already been tested for these biomarkers and resulted to be positive [1]. Therefore, current evidence supports EGFR and ALK testing before prescribing pre- or perioperative chemo-IO. For this reason, I recommend reserving the preoperative chemo-IO option for only EGFR and ALK wild-type patients. On the other hand, the importance of knowing the preoperative EGFR and ALK status is of paramount importance, as highly effective adjuvant targeted therapies have been made available for radically resected early stage EGFR-mutated and ALK-rearranged NSCLCs, namely osimertinib and alectinib [10,11,12]. On this basis, I would encourage patients with resectable stage III NSCLCs who are EGFR and ALK-positive to undergo immediate surgery followed by adjuvant targeted therapy. In contrast, there are a number of ongoing studies that are evaluating a targeted therapy in the neoadjuvant setting for patients with a given driver genetic alteration. However, the relatively low occurrence of pathological complete response (path CR) suggests the need for refinement of targeted therapy in this context. To be more specific, I foresee the possibility of adding chemotherapy to targeted therapies to increase the rate of path CR [13]. On the other hand, I think the role of PD-L1 as a clinical decision-making tool in selecting resectable NSCLCs for pre- or perioperative chemo-IO is far from being conclusive. Although its positive expression is generally associated with an increased benefit in terms of path CR and event-free survival compared with PD-L1 negative tumors, improved rates of path CR and positive hazard ratios for event-free survival have also been observed for PD-L1 negative tumors [1,2,3,4,5]. Therefore, although PD-L1 has a clear predictive role, I do not think that the decision on whether pre- or perioperative chemo-IO is to be administered should rely on this biomarker.
However, I would like to point out that moving biomarker assessment before surgical resection may bring about new issues, such as the need for collecting enough tumor tissue at the time of initial biopsy and the necessity of a rapid turnaround time of molecular results. In addition, a re-biopsy for biomarker testing might be required in select cases of tissue exhaustion for histological examination.
By the way, Luca, there has been much concern about patients with resectable stage III NSCLCs who do not make it to surgery because of disease progression or who receive suboptimal R1/R2 resection after preoperative chemo-IO. Randomized studies have suggested this might happen in approximately 10–15% and 5–10% of patients, respectively [1, 3,4,5]. As a thoracic surgeon, what is your opinion about the fact that some of the patients treated with preoperative chemo-IO may miss surgery because of early progression? What do you think about the possibility that a few of the patients undergoing surgery after chemo-IO may not be radically resected?
LB: The scenario you described highlights a challenge in the treatment of patients with thoracic cancers who receive preoperative chemo-IO. In some cases, patients may experience early disease progression during or after chemo-IO treatment, making surgery no longer a viable option. This situation can be frustrating for both patients and healthcare providers, as the goal of treatment is to achieve a radical resection, meaning the complete removal of the cancerous tissue. If surgery is not possible owing to disease progression, alternative treatment options, such as additional systemic therapies or radiation therapy, might be considered depending on the patient’s overall health and the extent of the disease. It is important for oncologists and MDTs to carefully assess each patient’s case, considering factors, such as cancer stage, response to preoperative treatment, and the patient’s overall health. Individualized treatment plans should be developed to maximize the chances of achieving a radical resection and improving the patient’s long-term outcomes. Additionally, ongoing research and clinical trials are essential to improve the overall success rates of surgical interventions following preoperative chemo-IO.
GM: Yes Luca, you are right. I would like to add to your considerations that surgery canceling for adverse events, including immune-related ones, has been particularly low in randomized trials, being approximately 1–3% [1, 3,4,5]. Indeed, this may reflect the fact that patients were carefully selected in these trials, which may not apply to patients who are treated in real-world clinical practice. However, vigilant treatment monitoring with health staff training, patient education, and collaboration with a network of experts could help early intervention and improve the recovery outcomes in cases of treatment-related side effects. Another important point that should be stressed is the optimal duration of preoperative chemo-IO. A higher number of cycles may result in a higher risk of developing treatment-related toxicity. Although most of the studies have adopted four cycles, there is evidence suggesting that the delivery of three cycles of preoperative chemo-IO could be sufficient in the preoperative setting [14, 15].
In addition, I believe that it might be of interest to mention another neoadjuvant approach which has been recently investigated, combining stereotactic radiotherapy and a checkpoint inhibitor. In a phase II trial comparing neoadjuvant durvalumab alone versus neoadjuvant durvalumab plus radiotherapy, a major pathological response was observed in 16 out of 30 patients in the dual therapy group, with 8 patients experiencing a path CR. The small sample size and the lack of chemotherapy in the control arm limit the strength of the study, but it could pave the way for new strategies in the neoadjuvant setting [16].
Luca, changing topic, I wanted to ask you if you foresee any surgical challenges in operating on patients after preoperative chemo-IO.
LB: Yes. Patients who have received preoperative chemo-IO may face specific challenges during surgery owing to the effects of these treatments on their bodies. Preoperative chemo-IO can sometimes lead to tissue fibrosis and scarring, making it harder for surgeons to distinguish between cancerous and healthy tissue. This can increase the complexity of the surgery. Chemotherapy can also impair the body’s ability to heal wounds. Surgical incisions may take longer to heal, and there might be an increased risk of infection. Patients who have undergone chemo-IO might be at a higher risk of surgical complications, such as infections, delayed healing, fistula, or poor tissue perfusion. In addition, determining the optimal timing for surgery after chemo-IO is crucial. Surgery performed too soon after these treatments may not allow sufficient time for the patient to recover and might increase the risk of complications. On the other hand, delaying surgery for too long might allow the cancer to progress, reducing the chances of a successful resection. So to address these challenges, the MDTs carefully evaluate each patient’s case, including oncologists, surgeons, and other specialists. Individualized treatment plans are developed to optimize the timing of surgery and minimize risks. Close postoperative monitoring and supportive care are also essential to managing any complications that may arise after surgery. Additionally, ongoing research aims to improve our understanding of the interactions between chemo-IO and surgery, leading to better strategies for managing patients in this context.
GM: Yes, Luca, we still have to see the long-term outcomes of surgery after preoperative chemo-IO, which we will only see with a longer follow-up of completed and ongoing trials. By the way, I would like to focus on another crucial point, such as surgical intervention on NSCLCs, that has been defined as borderline resectable by a MDT, such as cT3–4 N2 patients, after a preoperative chemo-IO with a downstaging intent. In my opinion, current trials do not answer the question of whether preoperative chemo-IO can facilitate surgery through effective downstaging in the case of borderline resectable tumors. Moreover, it should be noted that for stage III patients, the integration of surgery into a multimodality treatment, such as chemo-radiotherapy has not been demonstrated to provide a statistically significant improvement in overall survival compared with chemo-radiotherapy alone [14, 15]. In addition, in the modern era, it is unclear whether a nonsurgical approach of chemoradiotherapy followed by a year of consolidation immunotherapy (such as the “PACIFIC” regimen) would be inferior to surgery given with pre- or perioperative chemo-IO. In the near future, the adoption of the 9th TNM staging classifications, which divides N2 involvement in N2a (single nodal station) and N2b (multiple nodal station), will help clarify the impact of preoperative chemo-IO as a downstaging tool for borderline resectable tumors on the basis of the number of nodal stations that are involved at first diagnosis [19]. An interesting study that may answer this practical question is the “BRIDGE” study in which unresectable stage III patients will initially be treated with preoperative chemo-IO for two cycles and then restaged for surgical purposes (NCT05925530). At the time of restaging by the MDT, tumors that are deemed resectable undergo two more cycles of chemo-IO followed by surgery and adjuvant immunotherapy. At the same time, those who are still judged to be unresectable are treated with chemoradiotherapy alone.
Luca, what do you think of the role of chemo-IO administered with a down-staging intent, possibly shifting from cases in which pneumonectomy is indicated to less invasive surgical resections, such as lobectomy?
LB: The use of chemo-IO with a down-staging intent, particularly in cases where pneumonectomy was initially indicated, is a topic of ongoing research and clinical interest in the field of thoracic oncology. Shifting from pneumonectomy to less invasive surgical resections, such as lobectomy, can offer several potential advantages and considerations. Lobectomy preserves more lung tissue than pneumonectomy, essential for maintaining lung function. Preserving lung function can significantly improve the patient’s quality of life postsurgery. Less invasive surgeries should generally have lower complication rates and a shorter recovery than a pneumonectomy [20]. This can be especially beneficial for patients who may not tolerate the extensive nature of a pneumonectomy. Patients who were initially deemed unfit for a pneumonectomy owing to comorbidities or poor lung function might become eligible for surgery after a downstaging approach. This could expand the pool of patients who can potentially benefit from surgical intervention. Studies have suggested that patients undergoing less extensive lung resections tend to have better postoperative outcomes, including reduced rates of complications and improved overall survival [21]. The decision to perform a specific type of surgery should be individualized on the basis of the patient’s overall health, tumor characteristics, and response to preoperative chemo-IO. A MDT, including thoracic surgeons, medical oncologists, and pulmonologists, collaborates to determine each patient’s most suitable treatment plan. Ongoing clinical trials and research efforts continue to explore the optimal sequencing of chemo-IO, the duration of treatment, and the most appropriate surgical approaches. These studies aim to refine treatment protocols and further improve patient outcomes. It is important to note that the decision regarding the type of surgical resection is highly individual and depends on various factors. Patients should have detailed discussions with their healthcare providers to understand the potential benefits, risks, and expected outcomes of the different surgical approaches after preoperative chemo-IO.
GM: Yes, Luca, I agree. Now I would like to focus on another hot topic, namely the role of adjuvant immunotherapy (IO) after preoperative chemo-IO. In the pre-immunotherapy era, the achievement of a path CR in patients who underwent surgery after preoperative chemotherapy had high prognostic value, being associated with a significantly increased survival [22]. At present, emerging evidence suggests that perioperative chemo-IO significantly prolongs survival versus chemotherapy alone, regardless of the pathologic response achieved [23]. However, the true impact of adjuvant IO on the survival of patients treated with surgery after preoperative chemo-IO is uncertain. All the phase III randomized trials of preoperative chemo-IO included the adjuvant IO component, except for CheckMate 816 [1,2,3,4,5,6]. In an attempt to simplify, it might be argued that if a patient achieves a path CR, the need for further adjuvant therapy using the same IO agent used in the preoperative setting might be questionable. On the other hand, if no path CR has been achieved, the appropriateness of continuing with the same adjuvant IO drug could also be questionable.
In Checkmate 816, which, I recall, was the only trial that did not include adjuvant IO, event-free survival curves for patients achieving a path CR suggested a high cure rate regardless of the preoperative treatment received (chemo-IO or chemotherapy only), which supports the fact that path CR might be used as a surrogate for cure with no need for additional adjuvant IO. However, the debate on adjuvant IO exists for patients with no path CR. Interestingly, similarly to CheckMate 816, in KEYNOTE-671 and CheckMate77T, the event-free survival curves of patients who received perioperative chemo-IO (meaning adjuvant component included) versus those who were treated with preoperative chemotherapy only did not appear to be much different for those experiencing a path CR. Conversely, the same curves appeared to diverge in favor of perioperative IO in cases of no path CR. This may suggest that adjuvant IO might be beneficial, especially for the group of patients who do not achieve a path CR. Therefore, it can be envisioned that patients who achieve a path CR are best managed with no further adjuvant therapy, which might be considered only for those who do not experience a path CR.
Nevertheless, besides the above speculations, biomarkers are needed to refine adjuvant treatment after preoperative chemo-IO. Among these, the detection of circulating tumor DNA through liquid biopsy to assess minimal residual disease after surgery could be valuable in identifying which patients should receive intensification of antitumor treatment, such as adjuvant immunotherapy [24].
Well, I think that concludes our discussion for today. Thank you Luca for sharing your thoughts on this critical topic. I hope our listeners have appreciated this discussion and found it helpful for decision-making with other specialists dedicated to treating resectable early-stage non-small cell lung cancer.
留言 (0)