German claims data were analyzed to estimate the prevalence and cumulative incidence of DLBCL and characterize real-world treatment patterns, including identification of treatment lines, different regimens, and treatment duration. The included patient population (n = 2633) was older (median age 75 years), highly comorbid (median CCI 8), and included a large proportion of untreated patients (19.5%). This is comparable to other real-world studies of DLBCL incidence in patient populations [26, 31], although this population differs greatly from patients included in clinical trials, which tend to exclude patients with a poor prognosis [14].
The prevalence and cumulative incidence of DLBCL were calculated for the most recently available year within the inclusion period (2020) and the previous year (2019). Prevalence in 2019/2020 was 34.8/36.7 per 100,000 patients (age- and sex-adjusted: 30.9/33.3 per 100,000), and the annual cumulative incidence of DLBCL was 14.0/12.7 per 100,000 patients in 2019/2020 (age- and sex-adjusted: 12.3/11.3 per 100,000).
Limited data on DLBCL prevalence are currently available, with only rough 10-year prevalence estimates provided by Kanas et al. (≈45 per 100,000 patients) [6]. Our findings for annual prevalence were in line with these data and contribute to the sparse knowledge in this field.
Cumulative incidence of DLBCL in our study was higher than the incidence rate estimates in Germany (7 cases per 100,000 person-years) [5], but in line with worldwide reports of incidence rates (2.3 to 13.8 cases per 100,000 person-years) [4]. This larger estimate was observed despite our conservative approach of including only patients with inpatient diagnoses or two confirmed consecutive outpatient specialist codes. The higher cumulative incidence found in our dataset could reflect an aging population, as the incidence of DLBCL is estimated to increase in the upcoming years [6]. The decline observed in cumulative incidence in 2020 may be a result of fewer diagnoses due to the COVID-19 pandemic [33]. However, a previous study using the AOK PLUS dataset found that the number of cancer diagnoses in 2020 did not differ significantly from 2019 [34].
The study revealed a large proportion of patient mortality (≈60%), highlighting the high medical need among patients with DLBCL. This is in part due to the approximately 20% of the included population who did not receive any DLBCL treatment during follow-up. This finding is in line with Borchmann et al., a study that used a different German claims dataset to examine survival outcomes of patients with DLBCL and which also found that 20% of included patients did not receive a DLBCL treatment regimen [25]. A study using US insurance data also described that approximately 25% of patients with DLBCL receive no treatment [35].
In this study, untreated patients had poor prognosis, with median OS of 3 months, which may be due to the significantly older population among untreated patients. Untreated patients may have had more advanced-stage disease [36] or poor performance status [37], which could not be ascertained in the data. Approximately 25% of untreated patients were still alive over 4 years after initial diagnosis, although the median survival rate of untreated DLBCL is reported as less than 1 year [2, 8]. Some patients categorized as untreated may have been treated through clinical trials, which could not be captured in our data. However, clinical trial recruitment in Germany is low compared to other European countries—only 500 patients per million inhabitants (0.5%) take part in clinical trials [38]. Due to our methodology for including patients, we also cannot rule out the possibility of false DLBCL diagnoses. Our Kaplan–Meier survival curves shown in Fig. 2 are comparable to Daneels et al., a study using Belgian health insurance data to describe first- and second-line treatments for DLBCL, which also showed poor survival outcomes for patients who did not receive chemo/radiotherapy in the first line [26].
Patient mortality was also common among treated patients, with approximately 25% of patients dying within 6 months of initiation of therapy (21.0% and 28.0% after start of LOT1 and LOT2). Patient mortality within 12 months after start of LOT1 or LOT2 was 32.2% and 42.9%, respectively. This underscores the aggressive course of the disease, despite the array of currently available treatment regimens for DLBCL. Median survival after the start of therapy among patients who received a second line or further (20.9 months, n = 403) was shorter compared to all treated patients (45.9 months, n = 2119). This is consistent with literature stating that prognosis after treatment failure is usually poor [17].
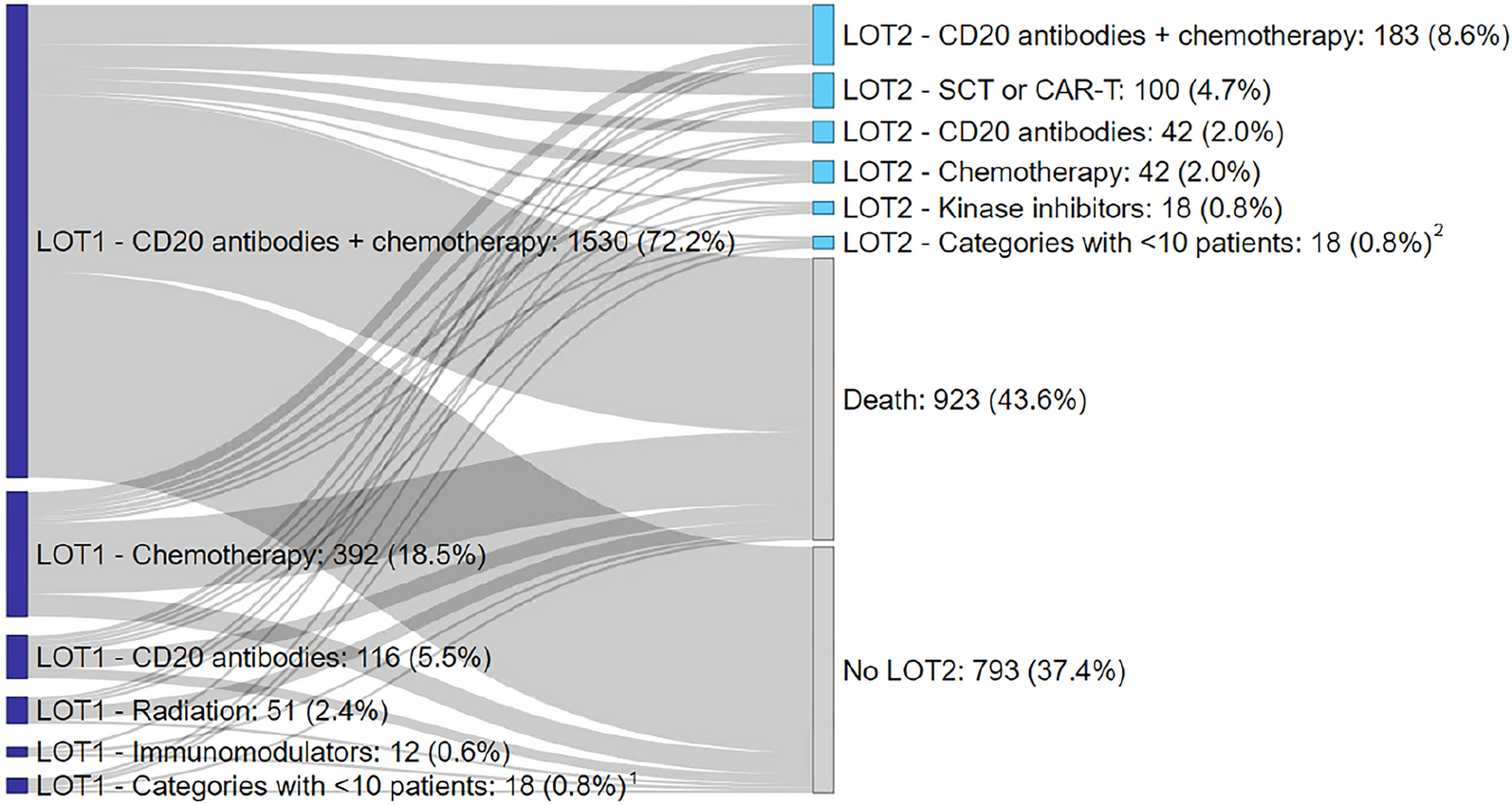
Among the 2119 patients who did receive DLBCL treatment, the vast majority (90.7%) were administered a chemotherapy regimen as a first-line therapy, mostly containing CD20 antibodies. The general guidelines for front-line DLBCL treatment recommend treatment with R-CHOP [39], and this regimen was also the most frequently identified chemotherapy combination (46.3% of outpatient treatments). Approximately 20% (n = 392) of chemotherapy patients did not receive CD20 antibodies. However, most of these patients (n = 346; 88.2%) received first-line treatment in the inpatient setting only, where chemotherapy treatments are identified only by OPS code. OPS codes for chemotherapy do not contain information about respective agents. We cannot rule out the possibility that in some cases, combination treatments such as R-CHOP were coded as chemotherapy in the inpatient setting, without the separate OPS code for rituximab (OPS 6-001.h, 6-001.j). Additionally, our results are consistent with Borchmann et al., which also found that approximately 20% of patients received regimens without rituximab in the first line [25]. Approximately 5% of all treated patients were given CD20 antibodies as monotherapy in the first-line treatment. As incident DLBCL is more commonly treated in combination with chemotherapy, patients who received monotherapy may have been older and presented with more comorbidities and therefore were unable to tolerate a full chemotherapy regimen [40]. Few patients (2.4%) received radiation therapy alone, likely as a treatment for localized disease [41].
We identified 403 patients (19%) that were administered a second-line treatment. This result was slightly higher than that of Daneels et al., which found that 16% of patients had refractory/relapsed disease, defined as second-line regimens within 2 years of diagnosis [26]. However, our study was able to capture second lines of treatment beyond 2 years of diagnosis, which may explain the higher percentages of identified patients. Reviews of DLBCL indicate that refractory/relapsed disease can occur in 30–40% of patients after initial treatment [15]. However, only 19% of patients in our study received LOT2 treatment, suggesting that a large proportion of refractory/relapsed patients get no second-line treatment due to death or ineligibility. Therefore, the actual proportion of refractory/relapsed patients in our sample may be higher than our findings.
Treatments received by patients in the second line were varied. In our study, SCT or CAR-T was performed as a second line for approximately one quarter of patients (n = 100; 24.8%), of which 82 patients were given autologous SCT. This is consistent with Harrysson et al., a Swedish medical chart review study, which found that approximately 22% of patients with a second line underwent SCT [17]. The overall low number of SCT treatments in our study also aligns with the study by Borchmann et al., which reported a very similar proportion of patients who underwent SCT. This implies that although SCT is a standard of care among transplant-eligible refractory/relapsed patients [20], many patients are unfit for SCT due to older age or a high number of comorbidities [19].
Additionally, despite CAR-T cell therapy being touted as an alternative to SCT for older and less fit patients [22], we observed very few patients receiving this treatment. CAR-T therapies axicabtagene ciloleucel (axi-cel) and tisagenlecleucel (tisa-cel) were first approved in Europe in 2018, which may explain the sparsity of this treatment in our dataset [42]. Lisocabtagene maraleucel (liso-cel) was not approved until 2022 [43], which is beyond the time frame of our analysis. Additionally, access to CAR-T after initial approval may have been constrained due to restrictive patient selection and limited numbers of CAR-T centers [42]. Our findings are in line with the number of CAR-T treatments performed in Germany [44] and the low numbers observed in Harrysson et al. [17].
The majority of patients (55.8%) were given chemotherapy regimens in the second line, with most patients in this category receiving chemotherapy containing CD20 antibodies. Daneels et al. also found that the majority of second-line regimens contained rituximab and chemotherapy, predominantly platinum-based [26]. Transplant-ineligible patients have historically been given chemoimmunotherapy regimens such as R-GemOx and BR with palliative intent, although these therapies often do not result in long-lasting remission [45]. Among LOT2 outpatient treatments (n = 196), only approximately one quarter (26.5%) of the regimens consisted of R-GemOx or BR, highlighting the heterogeneous treatment landscape and lack of a standardized approach among patients unfit for transplantation. With the addition of more market-authorized regimens such as Pola-BR (2020) and Tafa-Len (tafasitamab and Lenalidomide 2021) [46, 47], the variety of treatment options for DLBCL continues to grow.
Third-line or further treatments were also highly heterogeneous. The most frequent type of LOT3+ treatment was chemotherapy (54.4%), with a very low proportion of patients treated with chemotherapy without CD20 antibodies. This is in line with current guidelines, which recommend combination therapies, usually including a CD20 antibody [48]. Non-chemotherapy regimens comprising one third of the LOT3+ treatments and kinase inhibitors such as ibrutinib were administered in 13% of treatments. There is recent evidence that ibrutinib monotherapy may be used to effectively treat refractory/relapsed DLBCL with low toxicity [23]. The relatively frequent usage of non-chemotherapy regimens and newer treatment options in a real-world setting reflects the rapidly evolving treatment landscape of DLBCL and underlines the need to address treatment challenges among transplant-ineligible refractory/relapsed patients.
We observed that a large proportion of patients received treatment in inpatient settings only, although DLBCL is described as more commonly administered in the outpatient setting [49]. A study using US inpatient data found that chemotherapy was administered in approximately 30% of hospitalizations for DLBCL and more commonly for younger patients with fewer chronic conditions [49]. To our knowledge, no existing studies address the proportion of inpatient treatment for DLBCL within the context of Germany or Europe. Additional research is necessary to investigate reasons for the high proportion of inpatient treatment among these patients. We found that the proportion of patients receiving inpatient-only treatment decreased for LOT3+ treatments (36.0%) compared to LOT1 (48.1%) and LOT2 (51.4%). This may be because our study could not capture treatment in clinical trials, which occur more frequently in the hospital setting. However, as claims data do not contain information on the medical records of patients, it is difficult to interpret this finding.
Consistent with the literature, our study found that patients that were refractory or relapsed did so within a short period of time after DLBCL diagnosis [16, 17]. Although the dataset contained no information about symptom onset, we found that among patients with at least a second line, approximately 50% of patients received LOT2 treatment within 1 year after diagnosis. For patients with at least three treatment lines, 18.9% were already given a third line during the first year of follow-up. This number increased to 48.5% by 3 years of follow-up and 83.0% by 5 years of follow-up. This rapid progression between lines of therapy highlights the unmet need among refractory/relapsed patients. It is possible that the relatively short median time between treatment lines is due to our treatment line algorithm, which was used due to the lack of clinical information in claims data. However, our algorithm is consistent with methods used for other real-world studies [25, 26]. Short times between treatment lines may be indicative of refractory rather than relapsed disease. For example, Daneels et al. define refractory disease as the initiation of a second-line regimen within 12 weeks from the end of first-line therapy, whereas relapsed disease is defined as a second-line regimen beginning beyond 12 weeks of the end of the first-line therapy [26].
The main strength of this claims data analysis is the ability to capture incident cases irrespective of patient characteristics, such as age and comorbidities, and willingness to participate in clinical or observational studies, therefore contributing to high external validity. Additionally, we included patients who did not receive any DLBCL treatment, to avoid selection bias in excluding untreated patients. Our study also allowed for a long observation period, with up to 10 years of follow-up for patients with a first DLBCL diagnosis in 2012. The dataset covered both inpatient and outpatient treatment, and subsequently provides full coverage over all sectors of healthcare in Germany and information about the treatment setting of patients with DLBCL. Lastly, information from real-world clinical practice is limited (to our knowledge, there is no registry for patients with DLBCL in Germany), and therefore claims data analysis provides insight into this patient population. Our study contributes to the current body of real-world evidence on the epidemiology and treatment approaches for DLBCL.
We also acknowledge some intrinsic limitations, particularly related to the use of a retrospective anonymous claims dataset. The dataset did not include clinical details, such as stage of DLBCL at diagnosis or disease progression, as data are primarily used for reimbursement purposes. Treatment lines were identified indirectly via the specified algorithm, as we could not confirm the refractory/relapsed status of patients. Formally, we cannot rule out the possibility of false diagnosis, although we implemented a conservative approach to only include patients with inpatient diagnoses or two confirmed consecutive outpatient specialist codes. Our analysis also does not differentiate between subtypes of DLBCL, such as primary central nervous system lymphoma or post-transplant lymphoproliferative disease, which may be captured under the same ICD-10-GM code as DLBCL. Regional bias may be present, as AOK PLUS only insures patients from two German states (Saxony/Thuringia). However, in accordance with the German legal framework, health service reimbursement rules are identical across Germany, and previous studies have found no major regional differences in health care structures between Saxony/Thuringia and other German states [27].
A large number of treatment regimens were observed, and to protect patient anonymity, treatment categories were necessary to summarize the data. However, this subsequently led to loss of information. Additionally, detailed prescription data were only observed for treatments in the outpatient setting (outpatient only or inpatient/outpatient treatments). In the inpatient sector, chemotherapy treatments could be identified by OPS code, but the data did not contain information about the respective agents. Therefore, we could not ascertain the specific type of chemotherapy regimens received during inpatient treatment.
Our study also does not reflect all potential medical interventions applied to patients, such as participation in clinical trials which do not qualify for medical claims. Finally, due to the long study period, innovative therapies from recent years may be underrepresented compared to treatments that have been established for a longer time.


留言 (0)