
記住我
This is a cluster randomized trial using hybrid type III implementation-effectiveness study type [49] to assess the comparative effectiveness of a set of Core and enhanced (i.e., Core+) implementation strategies on the implementation and sustainment of cervical cancer screening and treatment for WHLIV. The hybrid type III design focuses primarily on testing IS effectiveness while observing clinical effectiveness outcomes [49]. HIV comprehensive treatment centers (k = 12) will be matched by region and randomized 1:1 to Core or Core+ strategies. We will assess both implementation and clinical outcomes and explore potential mechanisms that affect the study outcomes, including organizational readiness, implementation climate, CCST self-efficacy, and implementation intentions. The study is guided by two implementation science frameworks — EPIS and RE-AIM.
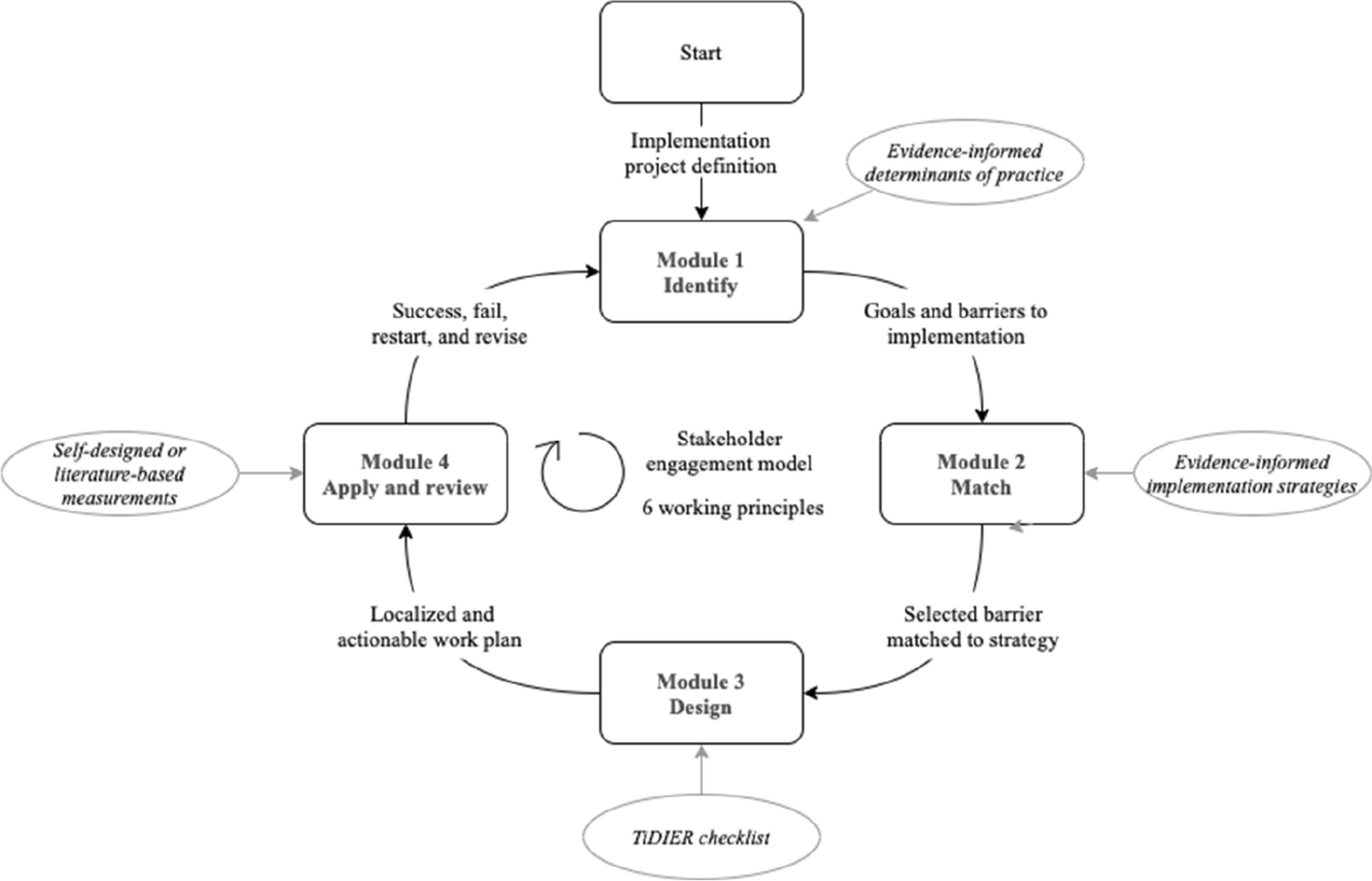
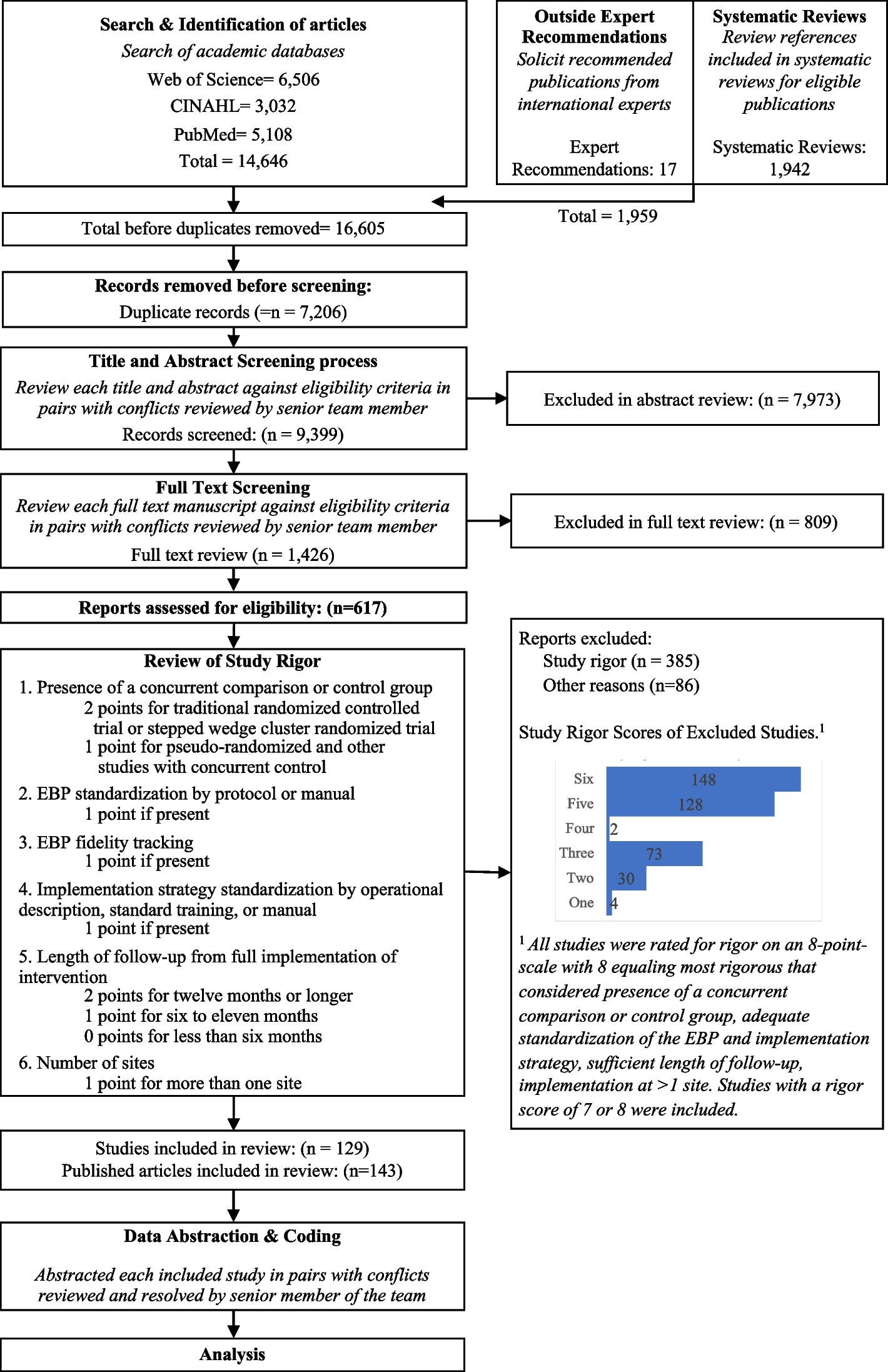
Exploration, preparation, implementation, and sustainment (EPIS) frameworkEPIS was selected because it is useful in guiding implementation in different settings including low-income countries [44, 46, 50]. Figure 1 shows the activities within each phase.
Fig. 1
EPIS framework activities and outer/inner contexts
Prior to grant submission and funding, we completed the exploration phase [48] where we used survey and modified nominal group techniques (NGT) [51] to conduct a rapid and facilitated implementation mapping [52] exercise. Collaborators identified and ranked barriers and identified, selected, and ranked implementation strategies starting with the Expert Recommendations for Implementing Change (ERIC) [53] and other identified additional strategies. The final set of strategies were selected to address the barriers to integration of CCST into HIV treatment programs to form the Core IS. Stakeholders identified two additional strategies to be included in the Core+ IS condition [48].
In the preparation phase, we refined the IS and convened implementation resource team (IRT) [54] meetings to further reflect on the refined Core and Core+ IS fit with local context. Implementation resource teams were first conceptualized and tested in the dynamic adaptation process model and the Interagency Collaborative Team model for scaling up evidence-based practices [54, 55]. The IRT for this study is a community-engaged co-creation collaborative comprising the research team and the doctors and nurses from the study sites. Twelve site research coordinators (SRCs) were also recruited and trained during this phase.
The process of refinement of our proposed implementation strategies occurred in two phases. In the first phase, the research team developed an IS table which included the identified implementation determinants (barriers/facilitators), the initially proposed IS for each determinant, a definition of each IS, the population targeted by the IS, the proposed actions for the IS, and the responsible person(s) for these proposed actions. For each IS, we discussed its feasibility and importance in addressing the implementation determinant based on the IRT’s current knowledge of the context in the implementation sites. For each IS that IRT identified as not being the most feasible or important to address the implementation determinant, we selected another IS from the same category in the ERIC grouping of implementation strategies [53], and we included some strategies not included in ERIC. The refined strategies are shown in Table 1.
In the second phase, 12 doctors and 12 nurses, 1 from each study site, participated in 2 focus-group discussions (FGDs) to further refine the IS. Each FGD was facilitated by a member of the research team with experience in qualitative data collection, using a semi-structured FGD guide, while two members of the research team took notes. Written informed consent was obtained from all the participants after reading the information about the study and the FGDs and given the opportunity to ask questions. Verbal consent was also obtained from the participants for the audio recording of the FGDs. The participants were presented with the refined implementation strategies table developed in the first phase and were asked to contribute to further refinement of the table, particularly tailoring the target population, planned actions, actor, dose, and mode of delivery. They were also asked to state if any of the IS or their activities would not be feasible at their sites. For any IS where the participants had different views about tailoring, discussions were held, and a consensus was reached. Each FGD lasted for about 2 h. Details of the further refined strategies are shown in Table 2. All of this work was in preparation for the cluster randomized trial to be described in the next section.
Table 2 Implementation strategiesIn the implementation phase, we will implement the Core and Core+ IS and test their comparative effectiveness on select implementation outcomes while collecting data on potential mechanisms of effects and clinical effectiveness outcomes. We will also catalog any ad hoc adaptations and contextual factors affecting implementation, services, and clinical outcomes with a focus on sustainment.
In the sustainment phase, we will assess sustainment of CCST and IS at each site and provide summaries to stakeholders regarding the planned and ad hoc adaptations that occurred during implementation.
Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM)We selected RE-AIM as our evaluation framework for assessing individual- and setting-level outcomes important to program impact and sustainment [56, 57]. As shown in Table 3, we address relevant RE-AIM constructs: Reach, Effectiveness, Adoption, Implementation, and Maintenance (also known as Sustainment) [56, 57]. In operationalizing these five dimensions, we adapted the metrics recommended by the Integrative Systems Praxis for Implementation Research (INSPIRE) model [58]. We defined the constructs as follows: reach (screening rate); clinical effectiveness (posttreatment screen negative); adoption (uptake of IS by study sites); IS fidelity (degree to which the IS occurred according to protocol); implementation clinical intervention fidelity (delivery of CC screening, onsite treatment, and referral according to protocol); and maintenance (or sustainment) (the degree to which integration of CCST continued).
Table 3 Measures by EPIS phase and study aimsSite selectionThe study will leverage the 21 comprehensive HIV treatment sites across the six geopolitical zones of Nigeria that have been designated as Nigeria Implementation Science Alliance (NISA) Model Innovation and Research Centers (NISA-MIRC) [65]. The NISA-MIRC sites are part of the ICON-3 Practice-based Research Network which is made up of the 21 NISA-MIRCs and the 6 Regional Centers of Excellence. The NISA-MIRCs have over 60,000 WLHIV in care who are eligible for enrollment into clinical trials and other implementation research studies [65]. Our proposed study will be anchored at 12 sites (see Figure 2 and Additional file 1) from the 21 NISA-MIRCs. The criteria for selection were based on the following: (1) geographical spread (two sites per region), (2) highest proportion of consented WLHIV for enrolment into clinical trials and other implementation research studies, and (3) match of the same type of site per region (secondary or tertiary).
Fig. 2
12 NISA-MIRCs selected for ACCESS study
RandomizationThe unit of randomization will be the sites. Each site represents a cluster in the randomization representing the clinic site and the WLHIV receiving treatment at the site. We will conduct simple random allocation with the sites randomized to either the Core or Core+ IS. There are six geographic regions in Nigeria, and sites will first be matched by region, and then each site in a matched pair will be randomized to Core or Core+ IS. A random number generator will be used to assign the sites. A flow diagram for the randomization and intervention allocation is shown in Figure 3. The healthcare workers and the patients will be blinded to whether their sites are allocated to the core package of IS or an enhanced package of IS.
Fig. 3 Methods for each study aim
Methods for each study aim
Aim 1: To refine strategies to integrate cervical cancer screening and treatment of cervical precancers within existing comprehensive HIV treatment programs. This has been described above in the EPIS preparation phase, and the findings are included in Tables 1 and 2.
Aim 2: To determine the comparative effectiveness of the Core vs Core+ Implementation Strategies on CSST
Study populationTo be eligible for enrolment into the trial, a woman must meet all the following criteria:
Be between 25 and 63 years
Have been diagnosed with HIV
Enrolled into HIV care in the sites
WLHIV will not be eligible to be enrolled into the trial if they have been previously diagnosed with preinvasive or invasive CC, received CC screening at any time within the previous 12 months, or are not willing to participate in the study procedures.
Recruitment and retentionThe medical records team will provide a list of potentially eligible WLHIV based on the eligibility criteria. The eligible WLHIV will be approached by the SRCs for recruitment into the study. For those who indicate interest, the SRCs will provide more details about the study, after which signed informed consent will be obtained electronically using REDCap. The consent forms will be read to all the participants in the English language. When there is a language barrier, the multilingual SRCs will interact with the potential participants in their local dialect. At enrollment, appointments for their next visit (data collection) will be scheduled.
Data collectionSociodemographic and baseline data will be collected from the enrolled participants who will also be followed up to assess the outcomes of interest using structured follow-up questionnaires in addition to their electronic medical records. Data on potential determinants and mechanisms will be obtained from the healthcare providers, using the following validated instruments (see Additional file 2).
Organizational Readiness for Implementing Change (ORIC)The ORIC assesses organizational readiness through two subscales, change commitment, and change valence. The ORIC has established high inter-item consistency and inter-rater reliability for both subscales [66].
Implementation climate measure (ICM)The six-item ICM has three subscales that assess perceptions of the degree to which a specific evidence-based practice (EBP) or innovation is expected, supported, and rewarded (i.e., recognition) in a clinic or organization [67]. The ICM has established strong psychometric properties.
Measure of innovation-specific implementation intentions (MISII)The MISII is a three-item pragmatic measure of direct service providers’ (e.g., physicians, nurses, providers) intentions to engage with and use a specific innovation such as CCST [68]. The MISII has strong psychometric properties.
Self-Efficacy/EBP Beliefs ScaleThis scale assesses the perceived value of the EBP and self-efficacy regarding the ability to implement the EBP. We will use the seven items that directly assess self-efficacy and we will tailor them to refer to CCST [69].
Outcome measuresThe measures for the implementation and clinical outcomes and the potential mechanisms are summarized in Table 3.
Sample size and power calculationWe examine the sample size for the primary implementation outcome of “reach,” indicated by the CC screening rate in WLHIV. Based on preliminary data from previous studies, we assumed a conservative screen rate of 14% in the core implementation strategy group [70]. We plan to enroll 12 sites (6 sites per intervention group). Hade et al. [71] reported the range of intraclass correlation (ICC) fall in 0.02–0.07 in the group-randomized breast and CC screening studies. We performed a sensitivity analysis by assuming a range of ICC of 0.02–0.07 for site cluster effect on the outcome and a feasible sample size of 200 subjects per site. We estimated that we could achieve at least 80% power for ICC of 0.02–0.06 (84% for ICC = 0.06 and > 99.9% for ICC = 0.02) to detect a minimum improvement of 20 percentage points in screening rate (that is, 34% screening rate) in Core+ group using a two-sided type I error of 0.05, and we could still achieve 78.6% power for ICC = 0.07. The 34% screening rate is achievable and a conservative estimate for the Core+ group based on our prior related work [61]. The power analysis was conducted using the statistical software R package cluster Power [72].
Data analysisPreliminary analyses will begin with an examination of the distribution of variables to assess and describe their characteristics (means, standard deviations, quartiles, ranges, frequencies, and percentages) for overall and for Core and Core+ groups separately and to allow assessment of randomization. Randomization will be tested by performing a series of Wilcoxon rank-sum tests for continuous variables and chi-square (or Fisher’s exact) tests for categorical variables to compare the groups on baseline demographic and clinical variables. Variables on which the groups differ initially will be explored as covariates in subsequent analysis. Intent-to-treat analysis will be conducted as the primary analysis. All estimates (point estimates and 95% confidence intervals) for the study outcomes will be adjusted by the cluster effect of clinics as described below.
The screening rate (primary outcome) will be summarized by frequency and proportion. A generalized linear mixed-effect model (GLMM) [73] with a binomial link will be used to examine the difference in screening rate (reach outcome) between Core and Core+. A random intercept will be included in the model to account for the cluster effect of the site. Multivariable random effects models will be used to examine the impact of covariates on estimated intervention effects. The GLMM will be also used to compare secondary outcome measures related to adoption, implementation strategies fidelity, and clinical intervention fidelity between two intervention groups, with a binomial link for a binary outcome and a Gaussian link for a continuous outcome. The ICM, MISII, and Self-Efficacy/EBP Beliefs Scale data collected from providers will also be analyzed similarly using the GLMM.
Covariate prescreening and variable selection procedureIn the multivariable model described above, adjustments are typically made to correct for baseline imbalances between groups and to adjust for variables known to influence the outcome independent of the intervention. Baseline characteristics will be pre-screened and assessed for an imbalance between the two intervention groups (Wilcoxon rank-sum test or Fisher’s exact test) and their association with the outcome (univariable mixed-effects model). Only those variables found to be moderately associated (p < 0.15) with the outcome or imbalanced (p < 0.10) between groups will be considered as potential covariates in the initial multivariable model. Backward elimination of insignificant variables will be used to select the main effects in the final model; all covariates that are significant at p < 0.10 will be kept in the final model.
Missing dataIn the case of missing data, missing patterns will be assessed by comparing patient characteristics between patients with and without missing data. Appropriate data analytic techniques will be used for analysis, which may include deletion, imputation, and inclusion of an indicator of missing values.
Study populationThis will include healthcare providers (doctors and nurses) that provided CCST for WLHIV and healthcare administrators (medical directors) in the NISA-MIRCs study sites.
RecruitmentHealthcare providers/administrators will be invited via letters and emails to participate in a survey and FGD.
Data collectionQuantitative data will be collected from the healthcare providers/administrators using the Provider REport of Sustainment Scale (PRESS) [74]. The PRESS is a brief and pragmatic three-item measure of sustainment that can be used across different EBP, provider types, and settings. The PRESS captures clinic staff’s report of their clinic, team, or agency’s continued use of an EBP or innovation in practice. The PRESS has excellent psychometric characteristics. Items are measured on a 5-point Likert scale ranging from (0 [not at all] to 4 [to a very great extent]. Qualitative data regarding sustainment will be collected using FGD with doctors, nurses, and administrators in each of the sites.
Sample sizeAbout 36–48 health care providers (3–4 per site) will be surveyed using PRESS. We will conduct 2 FGDs (Core and Core+) with 12 participants per group.
Data analysisWe will analyze data using a mixed-methods approach. From the quantitative data, we will classify sustainment status according to Wiltsey Stirman and colleague’s recommendations [75] and as used by Aarons and colleagues [76]. For the mixed-methods integration, we will use a QUAN+QUAL approach in which data are gathered and given equal weight [77]. We will triangulate qualitative and quantitative data to examine convergence, expansion, and complementarity when developing overall interpretations and conclusions [77,78,79,80,81,82,83]. We will create matrices to identify and summarize convergences and divergences in analyses of all data sources integrating results into a comprehensive picture [80]. We will first consider each type of analysis on its own terms and how they differ or converge [79, 84] by linking qualitative and quantitative databases and embedding one within the other so that each has a supportive function to play.
Study proceduresDue to the available infrastructure in the 12 study sites, CC screening in this study will be performed using VIA. In line with the standard of care in the sites, the decision to treat preinvasive cancer lesions will be based on the result of the screening test only, and not on a histologically confirmed diagnosis (screen and treat approach). Treatment of preinvasive cancer lesions will be through ablative therapy. Participants with preinvasive lesions that are not eligible for ablative treatment, or with suspected cancer lesions, will be referred to one of the regional oncology centers of excellence (Figure 4).
Fig. 4
Algorithm for VIA-based screening, treatment, and referral
Schedule of measurementWe will collect baseline data on the potential mechanisms (ORIC and MISII) and CC screening rates among WLHIV in the 12 facilities (Figure 5). In aim 2, each participant will be assessed at 12 months after enrollment for the receipt of CC screening (study M33). Treatment of precancerous lesions and referral of suspected cancer or lesions ineligible for treatment will be assessed at 12 and 18 months after enrollment (study M33 and M39). Posttreatment follow-up screening will be assessed at 27 and 33 months after recruitment (study M48 & M54). Data on specific potential mechanisms will be collected from the healthcare providers after recruitment and then 6 months, 12 months, and annually.
Fig. 5 Tracking adaptations
Tracking adaptationsWe will use quarterly “periodic reflections” [85] with the entire investigative team to consider any ad hoc adaptations that occurred at any of the sites. We will adapt periodic reflection focus-group guides for the discussion around what adaptations may have occurred, why they occurred, at what system or organizational level, who was involved, and the time frame. We will catalog adaptations and place them within the EPIS framework identifying the phase when they occurred and whether they arose from or impacted EPIS determinants or mechanisms in outer context, inner context, bridging factors, or the innovation itself (i.e., CCST). We will also place adaptations within the FRAME-IS model for cataloging and reporting adaptations [86, 87].
Data handlingWe will manage study data using REDCap (Research Electronic Data Capture; http://project-redcap.org/). REDCap provides user-friendly secure web-based case report forms and real-time data entry. We will use password-protected and encrypted tablets, laptops, and external drives that are institutionally certified and issued for data storage. Study data will be shared with only principal investigator-approved study staff via secure file transfer platforms.
留言 (0)