Given the unalterable nature of primary brain injury following traumatic brain injury (TBI), it becomes imperative to focus on mitigating secondary brain injury in order to optimize the prognosis for patients with TBI. Secondary injuries encompass the expansion of hematoma, development of cerebral edema, elevation of intracranial pressure, occurrence of infection, hypoxia, and coagulopathy. The cerebral tissue contains significant amounts of thromboplastin, which are released into the bloodstream at elevated concentrations following physical trauma to the parenchyma, thereby initiating disruptions in the coagulation process [24, 25]. Additionally, impaired cerebral endothelium activates platelets and initiates the coagulation cascade, resulting in intravascular thrombosis and depletion of coagulation factors [26].
The synthetic compound tranexamic acid (TXA), composed of lysine analogues, functions as a potent inhibitor of plasminogen activation. This mechanism facilitates the preservation of mature fibrin clots and ensures continuous coagulation. The rationale behind the enhanced clinical outcomes observed with TXA treatment in TBI lies in its potential to mitigate secondary brain injury through two mechanisms. Firstly, as an antifibrinolytic agent, TXA may exert its effect by inhibiting fibrinolysis and thereby impeding the progression of intracerebral hemorrhage—a common occurrence in TBI that has been identified as a significant independent predictor [27]. Secondly, through the inhibition of tissue plasminogen activator activity, TXA may also exert a potential role in ameliorating perilesional edema [28].
The CRASH-3 trial has demonstrated the safety of TXA in patients with TBI, and early administration within 3 h of injury significantly reduces mortality associated with head injuries [15]. Hence, the timing of tranexamic acid administration mentioned in the literature predominantly early intervention. The primary outcome for CRASH-3 was modified during the trial, shifting from all-cause mortality to head-injury-related mortality within 28 days following the injury [15]. Due to the inherent subjectivity in the classification of causes of death, this approach is susceptible to classification errors and has the potential to introduce bias into otherwise objective findings [29]. Therefore, the mortality mentioned in the article refers to all-cause mortality, rather than specifically deaths related to head injury.
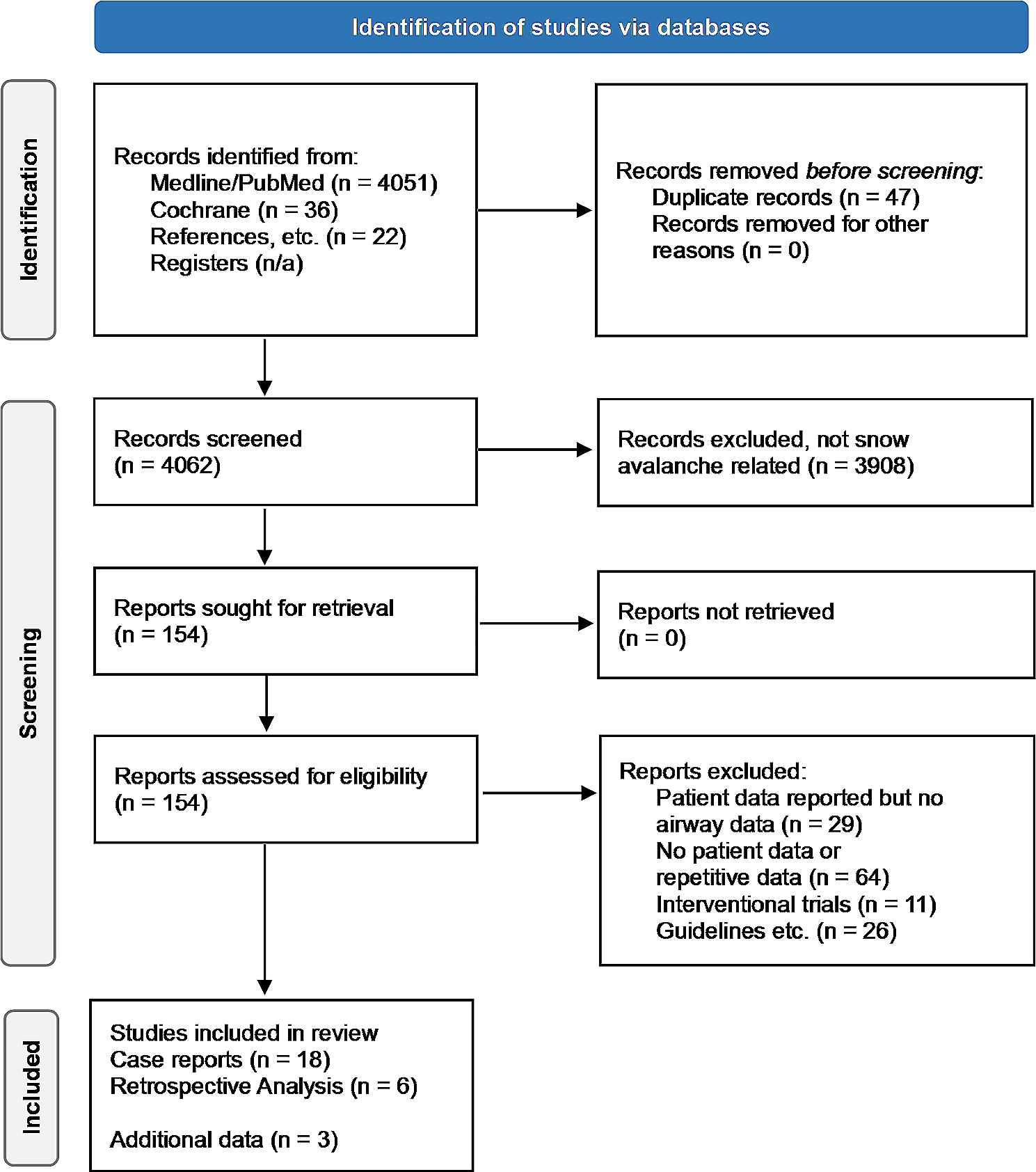
In this meta-analysis, 10 studies involving 11,299 patients were included. Our meta-analysis suggests that TXA can substantially reduce mortality compared to placebo for TBI. The expansion of intracranial hematoma can lead to an increase in intracranial pressure, cerebral herniation, and even fatality. The synthetic derivative of lysine, TXA, exerts its action by inhibiting fibrinolysis through the blockade of lysine binding sites on plasminogen. This mechanism attenuates fibrinolysis levels during the early stages following injury, thereby mitigating the expansion of intracranial hematoma. The nested analysis of CRASH-3 revealed that [30] individuals who succumbed to craniocerebral injury exhibited a median time-adjusted increase in intracranial hemorrhage of 37 ml/h, whereas those who perished from non-craniocerebral injury experienced an increase of only 11 ml/h. The meta-analysis conducted by July [31] demonstrated that treatment with TXA significantly reduced mortality (RR = 0.92, 95% CI 0.88–0.97, P = 0.002) and hematoma expansion rate (RR = 0.79, 95% CI 0.64–0.97, P = 0.03) compared to intravenous placebo. Additionally, tissue injury and the subsequent release of inflammatory mediators following TBI can induce endothelial dysfunction, while the released inflammatory mediators can further contribute to vascular endothelial cell injury and depletion of coagulation factors. The activation of the inflammatory response and sympathetic adrenal system can induce an upregulation of extracellular proteolytic enzymes, resulting in shedding of the polysaccharide coating. These processes collectively contribute to an augmentation in blood–brain barrier permeability, potentially serving as underlying mechanisms for the development of intracerebral hemorrhage and brain edema following TBI [32]. Anderson et al. [33] demonstrated that early administration of TXA in patients with moderate and severe TBI can mitigate the elevation of plasma syndecan-1 and angiopoietin-2, inhibit protease-mediated degradation of vascular polysaccharide coating, and attenuate endothelial injury.
The administration of tranexamic acid, as compared to placebo, is associated with a significant reduction in both the extent and volume of hemorrhage growth in TBI. Hijazi et al. [34] employed a murine model of TBI to investigate the impact of tissue plasminogen activator (tPA) and urokinase plasminogen activator (uPA) gene knockout on persistent intracranial hemorrhage in TBI mice, revealing a significant reduction compared to wild-type mice. The tPA and uPA function as the two primary physiological triggers for initiating the activation of plasminogen. They proposed that TBI-induced endogenous hyperfibrinolysis acts as the primary determinant of hematoma expansion and coagulation abnormalities subsequent to TBI. The principal mediator of fibrinolysis is plasmin, which is generated via the cleavage of circulating plasminogen. The incidence of coagulation dysfunction in patients with TBI can reach up to 60%, primarily attributed to hyperfibrinolysis triggered by the surge of endogenous plasminogen activator [35]. The interaction between plasminogen and plasmin is impeded by TXA, thereby obstructing the activation of plasmin and inhibiting fibrinolysis. The size of hematoma diminishes proportionally with the initiation of TXA treatment at an earlier stage [36].
The findings of our study indicate that there is no statistically significant disparity in the number of patients necessitating neurosurgery following treatment with TXA. The decision to perform the operation may have been influenced by various other factors that could potentially attenuate the impact of TXA treatment in patients with TBI, such as the hematoma's location, patients' vital signs, clinical judgments made by physicians, and so on. The results of our analysis, however, still demonstrate the effective reduction of hematoma expansion and improvement in clinical outcomes by TXA. The achievement of a positive clinical outcome relies on the proper implementation of essential operations, which must be carried out as considered indispensable.
The TXA intervention did not yield a statistically significant difference in seizure occurrence compared to the placebo group among patients with TBI. The structural similarity between TXA and glycine allows for its competitive inhibition of glycine receptors in cortical and spinal cord neurons, as well as γ-aminobutyric acid receptors in cortical and medullary neurons of rats. This dual pathway inhibition can lead to an upregulation of excitatory synaptic stimulation, ultimately precipitating seizure occurrence [37]. The primary and secondary impairments to the blood–brain barrier in patients with TBI may contribute to an increased incidence of seizures associated with TXA. Additionally, the early administration of sedative medications in specific individuals with severe TBI may potentially obscure seizure symptoms.
No statistically significant difference was observed between the TXA intervention and placebo groups in terms of pulmonary embolism among patients with TBI. Theoretically, TXA's antifibrinolytic properties may potentially increase the risk of microvascular thrombosis or even pulmonary embolism (PE) if fibrinolysis is impaired or halted. The presence of PE, which can be induced by various confounding factors such as the interference of suspended red blood cells, plasma, and platelets, should also be considered as a potential confounder. Coagulation dysfunction following TBI is a complex and dynamic process, characterized by diverse phenotypes of dysfunction occurring at varying time intervals. The non-individualized administration of TXA may potentially contribute to the development of PE, although no relevant studies have yet confirmed this assertion. Nevertheless, the early administration of TXA in the immediate aftermath of injury remains a prevalent clinical practice.
The present study still possesses certain limitations. First, the present study incorporated the most comprehensive RCTs conducted to date, despite significant disparities in sample sizes observed across certain studies (exceeding 300 participants). Second, the type and severity of TBI, as well as the duration of TXA administration, varied across each included RCTs, potentially influencing the observed outcomes. Third, previous studies have presented incomplete raw data, potentially introducing biases that may impact the validity of the findings.








留言 (0)