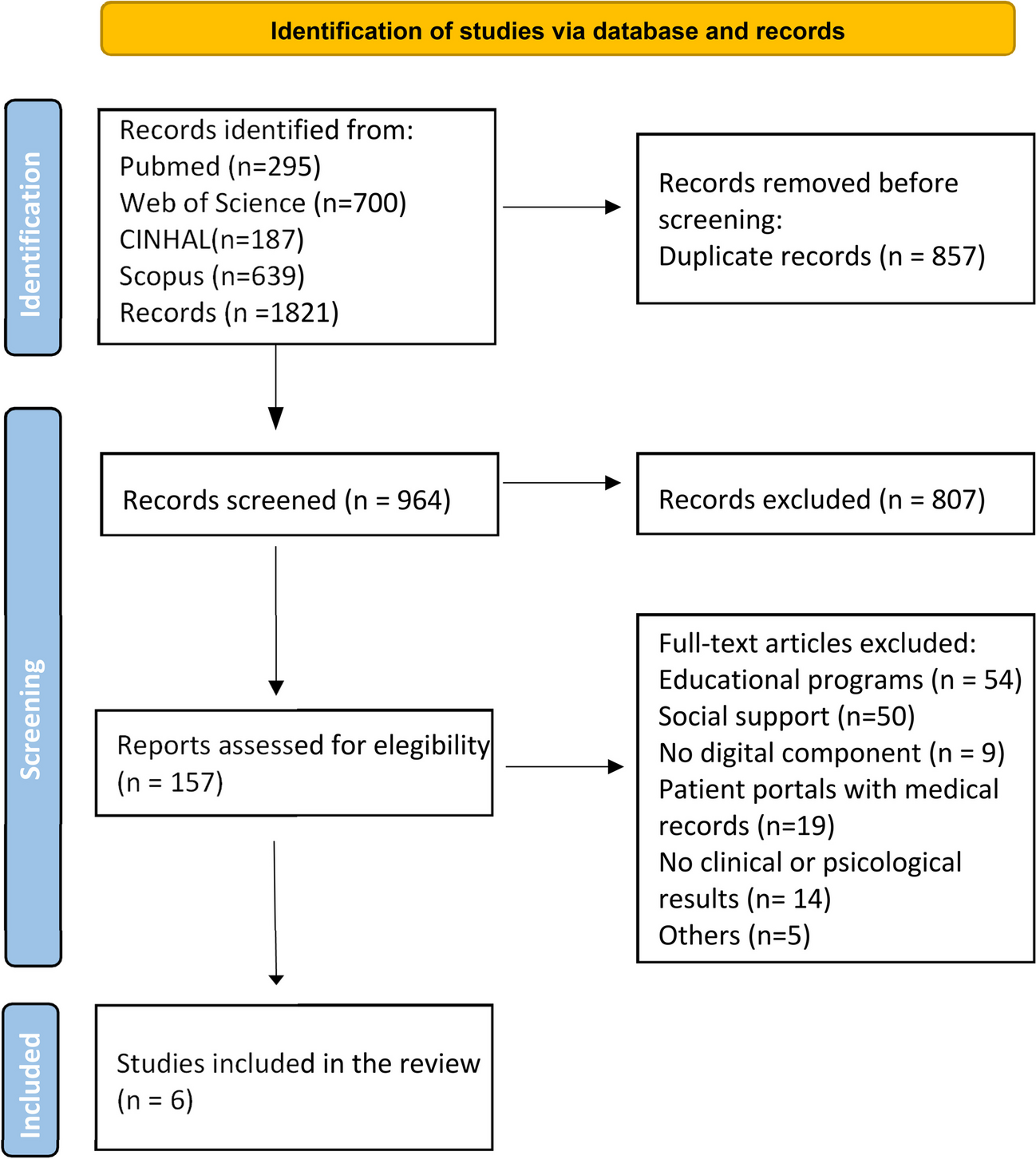
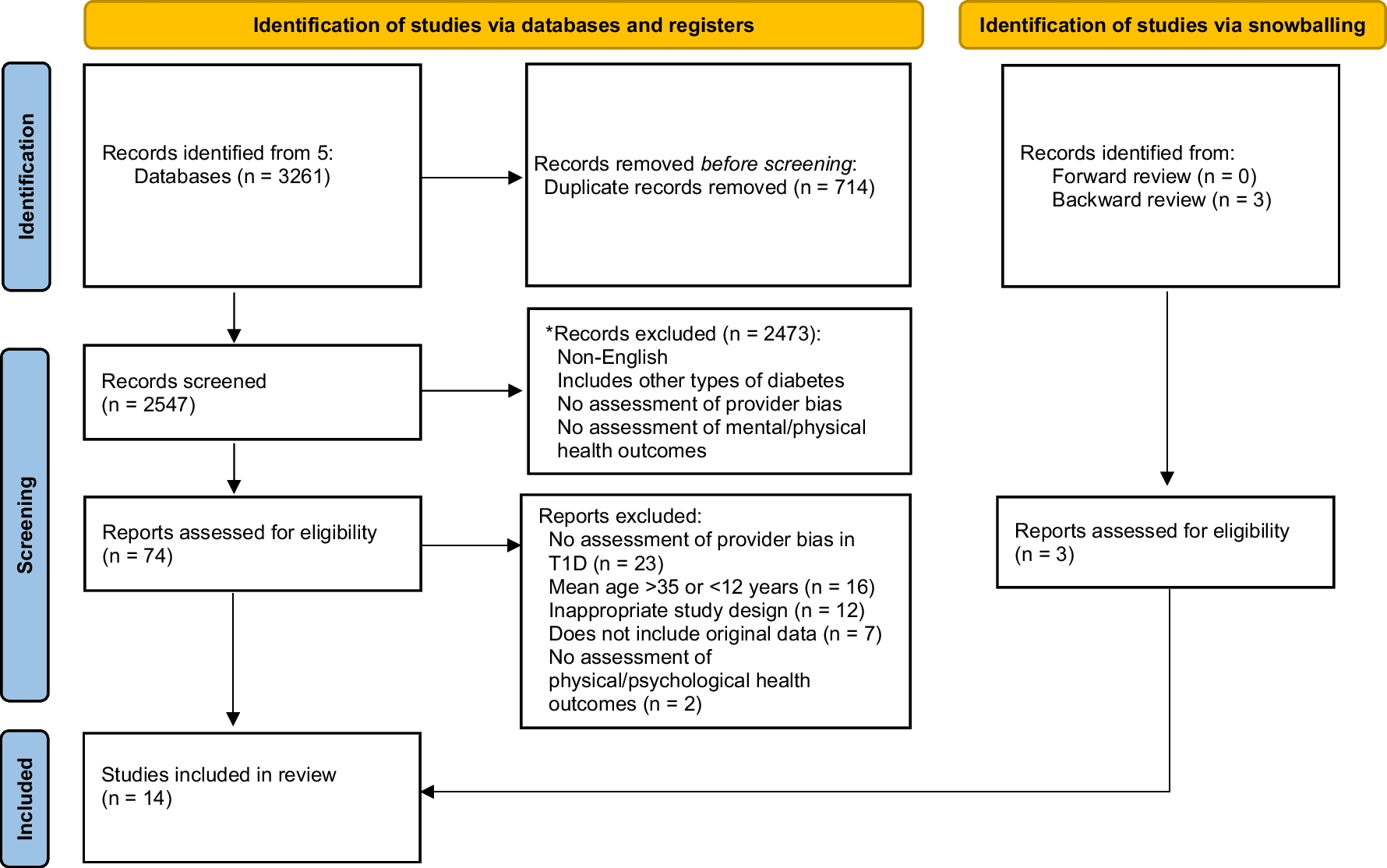
Five databases were used in the search, through which 1821 results were obtained. Once duplicate articles were removed, 964 studies were screened for relevancy. After reading the title and abstract, 157 were read completely. Of these articles, 151 were excluded for the following reasons: 54 of them were educational programs without peer interaction, 50 dealt with the importance of social support from friends and family and not between patients, 9 had no digital component, 19 evaluated a patient portal where they uploaded their medical records and communicated with healthcare professionals, 14 articles did not yield clinical or psychological outcomes and 5 were removed for other reasons (they did not talk about T2D, were communications of already selected articles, etc.) (Fig. 1). The remaining 6 studies were considered eligible for this review. The main characteristics of the studies are shown in Table 1 [20].
Table 1 Characteristics and results of studies of online communities in people with T2DThe results of the analysis of the studies are presented below, structured into the following sections: characteristics of the DOC, clinical outcomes, psychosocial outcomes and experiences of people with diabetes in using online communities.
Regarding the country of the studies, 50% (n = 3) came from the United States, and the remaining three studies were from South Korea, India and Spain.
Characteristics of Online Diabetes Communities
In this section we will explain the general aspects of the online communities analyzed, how they are dynamized and which members are in charge of moderating them and, finally, how people with T2D evaluate them.
General Features
Online diabetes communities can be set up on specific platforms or use available social networks. Related to this issue, both studies by Litchman et al. [25•, 26] and Herrero et al. [21•] used a diabetes-specific online community created on a web domain, while the other authors studied communities created on broader social networks such as Facebook [21•, 24]; Never Cafe [23•] or Second Life [22]. All of them still active.
Once we analyzed in more detail the characteristics of online communities, we found that the studies led by Litchman [25•, 26] used Beyond Type 2 [https://community.beyondtype2.org/), an online community created in 2009 by the non-profit organization Beyond Type 1. This community requires pre-registration for people with T2D to share their stories, connect with each other, and find resources on topics ranging from daily management to mental health management. The community has a group exclusively for Spanish-speaking people, tailored to the culture, customs and traditions. In addition, an email with new posts or news is sent monthly.
Nevertheless, in two of the articles, specific Facebook groups previously created are used [21•, 24]. As it is widely known, Facebook is a social network that requires the creation of a user to access. Facebook groups, which can be public or private, are small groups that allow quick and easy organization of people with similar interests or characteristics, who can share messages, images, and material on the group's wall. Both “Diabetes support” (https://www.facebook.com/groups/MyDiabetes/about) and “Diabetes contact group” (https://www.facebook.com/groups/1169185889761308) were created in 2016, to provide support and information about diabetes in addition to connecting people living with diabetes or their family and friends. The LCHF group (https://www.facebook.com/groups/LCHF4LIFE) originated in 2014 and focuses on learning and discussing the low-carbohydrate diet [24]. All of them are still active.
Never Café (https://cafe.naver.com/) is one of the most popular social networks in South Korea, very similar to the previous one. On this platform, the authors developed the community “Diabetes, my companion” with four main activities: diabetes information, action planning in everyday life, patients´ chat room and questions and answers [23•].
Johnson et al. [22] created SLIDES (Second Life Impacts Diabetes Education & Self-Management), an ad-hoc community within Second Life social network (https://secondlife.com/), a virtual world founded in 2003, in which, unlike the previous ones, you can interact with other people through a personalized avatar and exchange virtual products. The SLIDES community provided self-care education and support based on social cognitive theory according to the user´s characteristics. It contained different resources such as a bookstore with links to buy books and links to web pages. In addition, there were restaurants with nutritional information, a gym with exercise videos, and a community center with a classroom, a slide projector, and a forum that allowed participants to share information and personal experiences. Training classes on diabetes were also offered in this virtual center.
The description of the online communities used by the selected studies is summarized in Table 2.
Table 2 Description of the online communities analyzed in the studiesDynamization of Online Diabetes Communities
In online communities, patients support each other. However, sometimes a figure to moderate the group is necessary. The details of the dynamization are shown in Table 3.
Table 3 Description of the dynamization of online communitiesUse of Online Communities by People with T2D
Regarding the use of online communities, three of them reported different metrics to measure the degree of use [22, 23•, 25•]. Johnson et al. [22] tracked engagement rates and use. Participants logged in to the community an average of 38 times, with an average of 43 min per session, during the 6 months they participated in the study. 75% of logins occurred within the first three months and the majority within the first month. 75% of items such as food, books, menus, web pages, videos, and pharmacy items were "handled" by 19 of the participants while in the community. Participants interacted with these items a total of 1,180 times.
In order to assess participation, Kim et al. [23•] used the summary statistical report of the platform Never Café. The average number of monthly visits of each person to the platform was 8.53. Eighty-four of participants revisited the site within 12 months. And within the different sections of the website, 69.7% returned to search for information on diabetes, 67% to action planning, 45% to the questions and answers section, and 73.3% to the chat. In addition, all verbal and text communications were continuously recorded for the duration of the study. Regarding communication, the members used their voice most of the time when they were with other people and spent most of the time in the classroom (48.6%) where classes were held twice a week.
Litchman, Ng, et al. [25•] analyzed the engagement rate, defined as 3 or more daily messages per participant. The highest rate was 61.5%, with 13 active participants in the forum. They also received a daily e-mail with a summary of new messages, but it was not possible to check their reading.
In both Litchman studies [25•, 26], although they were encouraged to participate 3 times a week, they did not specify if they complied or not. Herrero et al. [21•] only asked if they were members or not and since when, and did not measure the degree of participation. Verma et al. [24] indicated that they interviewed people who were actively involved in the DOC, but did not define what active participation was indeed.
Evidence in the Use of Online Diabetes Communities
The following sections describe the main clinical and psychosocial results addressed in the selected studies about online diabetes communities.
Clinical Results
In the studies analyzed, different clinical data were collected from patients, both directly related to diabetes and to general health condition, to assess the influence of the use of online communities on them (Table 4).
Table 4 Favorable clinical outcomes in results in the use of online communitiesIn order to analyze the improvement in glycemic control, changes in glycosylated hemoglobin (HbA1c), fasting blood glucose, and time in range were measured. Johnson et al. [22] observed a decrease in HbA1c of 0.59%, although it was not significant, while in the study by Kim et al. [23•] the intervention group presented a significantly lower level than the control group, for non-insulin users, at 3 (6.38; SD (Standard Deviation) = 0.34 vs. 7.25; SD = 0.24, p = 0.040) and 6 months (6.31; SD = 0.37 vs. 7.28; SD = 0.26, p = 0.036). With the same objective, they recorded fasting blood glucose, in which there were significant improvements in insulin-dependent people who participated in the intervention group at 6 months (135.80; SD = 12.37 vs. 175.82; SD = 15.34, p = 0.049). Also Litchman, Ng, et al. [25•] demonstrated that nine participants (37.5%) had a decrease of more than 0.5% HbA1c at 12 weeks, five (20.8%) had an increase of more than 0.5%, and 10 (41, 6%) had no significant changes. They used the time in range (between 70 and 180 mg/dl) in the same way, in which there were no statistically significant improvements either. However, there was an increase in glycemic variability (Z = − 2.172, p = 0.03).
Kim et al. [23•] found significant differences in the reduction of triglycerides (206.85, SD = 38.26 vs. 387.50, SD = 56.19, p = 0.013). However, there were no differences in the other measured outcomes such as blood pressure, weight, Body Mass Index or total cholesterol.
Nevertheless, Herrero et al. [21•] reported a greater number of complications derived from diabetes in people who used the DOC. There were differences between groups M = 1.95, SD = 1.28, for people with T2D not belonging to DOC and M = 4.77, SD = 0.72, for DOC users.
Psychosocial outcomes
Psychosocial data related to participants´ perceptions such as self-efficacy, self-care, social support, perceived presence and co-presence, quality of life, and knowledge about diabetes were collected in all studies (Table 5).
Table 5 Psychosocial resultsRegarding self-efficacy, Johnson et al. [22] used the Diabetes Empowerment Scale -Short Form (DES-SF). In a range from 1 to 5, at baseline of the study it was 3.89 points on average (SD = 0.81); however, it improved at 3 months (4.45, SD = 0.67, p = 0.036) and at 6 months (4.64, SD = 0.39, p = 0.02). While Litchman, Ng, et al. [25•] used the Self-efficacy Scale, whose score significantly improved after 12 weeks of community participation (68.6, SD = 18.3 vs. 82.7, SD = 14.5; p < 0.01).
Self-care was evaluated in three studies. Herrero et al. [21•] were based on the DSMQ (Diabetes Self -Management Questionnaire) by four subscales: glucose control, dietary control, physical activity, and use of the healthcare system; as well as a global score of all of them. People with T2D not belonging to online communities (32% of the sample) had a significantly higher score for diabetes self-management in all subscales: glucose control (4.34 vs. 2.51; p = 0.000), diet control (4.03 vs. 2.17; p = 0.000), healthcare (4.35 vs. 2.58; p = 0.000), physical activity (3.91 vs. 1.89; p = 0.000), diabetes care (4.05 vs. 2.90; p = 0.000); being 0 the minimum score and 10 being the maximum score. Both Johnson et al. [22] and Kim et al. [23•] assessed self-care using the Diabetes Self-Care Activities Scale (SDSCA), made up of 17 items that measure the number of days per week on which the indicated behavior is performed. It presents six subscales on a scale from 0 to 7: general diet, specific diet, physical activity and exercise, blood sugar testing, foot care, and medication. In the first of them, participants only showed a statistically significant improvement in the number of days per week spent to foot care. At baseline 3.68 days on average (SD = 2.08) and at 6 months 6.17 days (SD = 2.08) (p = 0.03). In contrast, in the study by Kim [23•] the only significant difference was in the improvement in medication behavior for insulin users in the intervention group at 3 and 6 months. (6.79, SD = 0.34 vs. 5.03, SD = 0.49, p = 0.004; 6.37, SD = 0.52 vs. 4.68, SD = 0.65, p = 0.047; respectively) [23•].




留言 (0)